Do you want BuboFlash to help you learning these things? Or do you want to add or correct something? Click here to log in or create user.
heat stroke
#harrison #has-images #heatstroke #medicine #paper1med
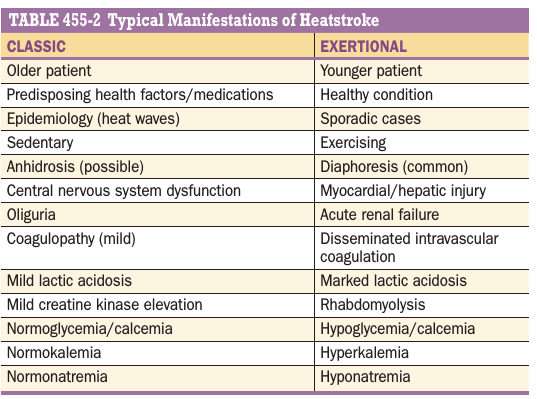
The clinical manifestations of heatstroke reflect a total loss of ther- moregulatory function. Typical vital-sign abnormalities include tac- hypnea, various tachycardias, hypotension, and a widened pulse pressure. Although there is no single specific diagnostic test, the historical and physical triad of exposure to a heat stress, CNS dysfunc- tion, and a core temperature >40.5°C helps establish the preliminary diagnosis. Some patients with impending heat stroke will initially appear lucid. The definitive diagnosis should be reserved until the other potential causes of hyperthermia are excluded. Many of the usual laboratory abnormalities seen with heatstroke overlap with other con- ditions. If the patient’s mental status does not improve with cooling, toxicologic screening may be indicated, and cranial CT and spinal fluid analysis can be considered. The premonitory clinical characteristics may be nonspecific and include weakness, dizziness, disorientation, ataxia, and gastrointestinal or psychiatric symptoms. These prodromal symptoms often resemble heat exhaustion. The sudden onset of heatstroke occurs when the main- tenance of adequate perfusion requires peripheral vasoconstriction to stabilize the mean arterial blood pressure. As a result, the cutaneous radiation of heat ceases. At this juncture, the core temperature rises dramatically. Since many patients with heatstroke also meet the crite- ria for systemic inflammatory response syndrome and have a broad differential diagnosis, rapid cooling is essential during the extensive diagnostic evaluation (Table 455-1). There are two forms of heatstroke with significantly different man- ifestations (Table 455-2). Classic (epidemic) heatstroke (CHS) usually occurs during long periods of high ambient temperature and humidity, as during summer heat waves. Patients with CHS commonly have chronic diseases that predispose to heat-related illness, and they may have limited access to oral fluids. Heat dissipation mechanisms are overwhelmed by both endogenous heat production and exogenous heat stress. Patients with CHS are often compliant with prescribed medica- tions that can impair tolerance to a heat stress. In many of these dehy- drated CHS patients, sweating has ceased and the skin is hot and dry. If cooling is delayed, severe hepatic dysfunction, renal failure, dis- seminated intravascular coagulation, and fulminant multisystem organ failure may occur. Hepatocytes are very heat sensitive. On presenta- tion, the serum level of aspartate aminotransferase (AST) is routinely elevated. Eventually, levels of both AST and alanine aminotransferase (ALT) often increase to >100 times the normal values. Coagulation studies commonly demonstrate decreased platelets, fibrinogen, and prothrombin. Most patients with CHS require cautious crystalloid resuscitation, electrolyte monitoring, and—in certain refractory cases— consideration of central venous pressure (CVP) measurements. Hyper- natremia is secondary to dehydration in CHS. Many patients exhibit significant stress leukocytosis, even in the absence of infection. Patients with exertional heatstroke (EHS), in contrast to those with CHS, are often young and previously healthy, and their diagnosis is usually more obvious from the history. Athletes, laborers, and mili- tary recruits are common victims. Unlike those with CHS, many EHS patients present profusely diaphoretic despite significant dehydration. As a result of muscular exertion, rhabdomyolysis and acute renal fail- ure are more common in EHS. Studies to detect rhabdomyolysis and its complications, including hypocalcemia and hyperphosphatemia, should be considered. Hyponatremia, hypoglycemia, and coagu- lopathies are frequent findings. Elevated creatine kinase and lactate dehydrogenase levels also suggest EHS. Oliguria is a common finding. Renal failure can result from direct thermal injury, untreated rhabdo- myolysis, or volume depletion. Common urinalysis findings include microscopic hematuria, myoglobinuria, and granular or red cell casts. With both CHS and EHS, heat-related reversible increases in cardiac biomarker levels are often present. Heatstroke often causes thermal car- diomyopathy. As a result, the CVP may be elevated despite significant dehydration. In addition, the patient often presents with potentially deceptive noncardiogenic pulmonary edema and basilar rales despite being significantly hypovolemic. The electrocardiogram commonly displays a variety of tachyarrhythmias, nonspecific ST-T wave changes, and heat-related ischemia or infarction. Rapid cooling—not the admin- istration of antiarrhythmic medications—is essential. Above 42°C (107.6°F), heat can rapidly produce direct cellular injury. Thermosensitive enzymes become nonfunctional, and eventually there is irreversible uncoupling of oxidative phosphorylation. The produc- tion of heat-shock proteins increases, and cytokines mediate a systemic inflammatory response. The vascular endothelium is also damaged, and this injury activates the coagulation cascade. Significant shunting away from the splanchnic circulation produces gastrointestinal ische- mia. Endotoxins further impair normal thermoregulation. As a result, if cooling is delayed, severe hepatic dysfunction, permanent renal failure, disseminated intravascular coagulation, and fulminant multisystem organ failure may occur.
If you want to change selection, open document below and click on "Move attachment"
pdfs
- owner: nerdparty67 - (no access) - HARRISON Principles of Internal Medicine 20th Edition.pdf, p3345
- owner: Anonymouse - (no access) - @MBS_MedicalBooksStore_2018_Harrison's.pdf, p3391
Summary
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Details
Discussion
Do you want to join discussion? Click here to log in or create user.