Edited, memorised or added to reading queue
on 28-Sep-2016 (Wed)
Do you want BuboFlash to help you learning these things? Click here to log in or create user.
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Abdo Pain
Cholecystitis (highest to lowest PPV) RUQ pain, fever, jaundice IBS algorithm <span>Objective General inspection Change in mental status (infection - UTI) Shock (perforated viscera, GI hemorrhage, severe pancreatitis, MI, sepsis) Vitals Upper abdo pain - pay attention to Cardiac (ischemia) & lung (pneumonia) exams Tachypneic (pneumonia) Abdo peritoneal signs Carnett’s sign (high ppv for abdo wall pain) ↑ pain when supine pt raises head & shoulder, tensing abdo wall Murphy’s sign (high ppv for choleycystitis) Psoas sign (high ppv for appendicitis) Sever pain out of proportion (ischemic bowel, pancreatitis) restless/writhing (biliary/renal colic, testicular torsion) LLQ tenderness (diverticulitis) Rectal & pelvic exams if lower abdo & pelvic pain DRE - fecal impaction, palpable mass, occult blood in stool Tenderness & fullness on R of rectum suggests retrocecal appendix Pelvic - vaginal discharge (vaginitis), cervical motion tenderness & peritoneal signs (ectopic pregnancy or other gyne complications e.g. tubo-ovarian abscess) S&S of surgical abdo Fever Protracted (prolonged) vomiting syncope/pre-syncope Evidence of GI blood loss
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Abdo Pain
Fever Protracted (prolonged) vomiting syncope/pre-syncope Evidence of GI blood loss Psychosocial factors assc w/ chr & recurrent abdo pain <span>Assessment Common causes IBS (discomfort/pain assc w/ altered bowel habits >3d/mo in prev 3 mo) Less common but important causes Appendicitis Acute cholecystitis Diverticulitis Acute pancreatitis Perforated ulcer Bowel infarction Plan (for acute abdo pain) - acute abdo = sudden, non-traumatic disorder needing urgent dx & tx Labs CBC (infection/blood loss)

| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open itObjective General inspection Change in mental status (infection - UTI) Shock (perforated viscera, GI hemorrhage, severe pancreatitis, MI, sepsis) Vitals Upper abdo pain - pay attention to Cardiac (ischemia) & lung (pneumonia) exams Tachypneic (pneumonia) 
Original toplevel document
Abdo PainCholecystitis (highest to lowest PPV) RUQ pain, fever, jaundice IBS algorithm <span>Objective General inspection Change in mental status (infection - UTI) Shock (perforated viscera, GI hemorrhage, severe pancreatitis, MI, sepsis) Vitals Upper abdo pain - pay attention to Cardiac (ischemia) & lung (pneumonia) exams Tachypneic (pneumonia) Abdo peritoneal signs Carnett’s sign (high ppv for abdo wall pain) ↑ pain when supine pt raises head & shoulder, tensing abdo wall Murphy’s sign (high ppv for choleycystitis) Psoas sign (high ppv for appendicitis) Sever pain out of proportion (ischemic bowel, pancreatitis) restless/writhing (biliary/renal colic, testicular torsion) LLQ tenderness (diverticulitis) Rectal & pelvic exams if lower abdo & pelvic pain DRE - fecal impaction, palpable mass, occult blood in stool Tenderness & fullness on R of rectum suggests retrocecal appendix Pelvic - vaginal discharge (vaginitis), cervical motion tenderness & peritoneal signs (ectopic pregnancy or other gyne complications e.g. tubo-ovarian abscess) S&S of surgical abdo Fever Protracted (prolonged) vomiting syncope/pre-syncope Evidence of GI blood loss
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open itive General inspection Change in mental status (infection - UTI) Shock (perforated viscera, GI hemorrhage, severe pancreatitis, MI, sepsis) Vitals <span>Upper abdo pain - pay attention to Cardiac (ischemia) & lung (pneumonia) exams Tachypneic (pneumonia) Abdo peritoneal signs Carnett’s sign (high ppv for abdo wall pain) ↑ pain when supine pt raises head & shoulder, ten
Original toplevel document
Abdo PainCholecystitis (highest to lowest PPV) RUQ pain, fever, jaundice IBS algorithm <span>Objective General inspection Change in mental status (infection - UTI) Shock (perforated viscera, GI hemorrhage, severe pancreatitis, MI, sepsis) Vitals Upper abdo pain - pay attention to Cardiac (ischemia) & lung (pneumonia) exams Tachypneic (pneumonia) Abdo peritoneal signs Carnett’s sign (high ppv for abdo wall pain) ↑ pain when supine pt raises head & shoulder, tensing abdo wall Murphy’s sign (high ppv for choleycystitis) Psoas sign (high ppv for appendicitis) Sever pain out of proportion (ischemic bowel, pancreatitis) restless/writhing (biliary/renal colic, testicular torsion) LLQ tenderness (diverticulitis) Rectal & pelvic exams if lower abdo & pelvic pain DRE - fecal impaction, palpable mass, occult blood in stool Tenderness & fullness on R of rectum suggests retrocecal appendix Pelvic - vaginal discharge (vaginitis), cervical motion tenderness & peritoneal signs (ectopic pregnancy or other gyne complications e.g. tubo-ovarian abscess) S&S of surgical abdo Fever Protracted (prolonged) vomiting syncope/pre-syncope Evidence of GI blood loss
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open ite pancreatitis, MI, sepsis) Vitals Upper abdo pain - pay attention to Cardiac (ischemia) & lung (pneumonia) exams Tachypneic (pneumonia) <span>Abdo peritoneal signs Carnett’s sign (high ppv for abdo wall pain) ↑ pain when supine pt raises head & shoulder, tensing abdo wall Murphy’s sign (high ppv for choleycystitis) Psoas sign (high ppv for appendicitis) Sever pain out of proportion (ischemic bowel, pancreatitis) restless/writhing (biliary/renal colic, testicular torsion) LLQ tenderness (diverticulitis) Rectal & pelvic exams if lower abdo & pelvic pain DRE - fecal impaction, palpable mass, occult blood in stool Tenderness & ful
Original toplevel document
Abdo PainCholecystitis (highest to lowest PPV) RUQ pain, fever, jaundice IBS algorithm <span>Objective General inspection Change in mental status (infection - UTI) Shock (perforated viscera, GI hemorrhage, severe pancreatitis, MI, sepsis) Vitals Upper abdo pain - pay attention to Cardiac (ischemia) & lung (pneumonia) exams Tachypneic (pneumonia) Abdo peritoneal signs Carnett’s sign (high ppv for abdo wall pain) ↑ pain when supine pt raises head & shoulder, tensing abdo wall Murphy’s sign (high ppv for choleycystitis) Psoas sign (high ppv for appendicitis) Sever pain out of proportion (ischemic bowel, pancreatitis) restless/writhing (biliary/renal colic, testicular torsion) LLQ tenderness (diverticulitis) Rectal & pelvic exams if lower abdo & pelvic pain DRE - fecal impaction, palpable mass, occult blood in stool Tenderness & fullness on R of rectum suggests retrocecal appendix Pelvic - vaginal discharge (vaginitis), cervical motion tenderness & peritoneal signs (ectopic pregnancy or other gyne complications e.g. tubo-ovarian abscess) S&S of surgical abdo Fever Protracted (prolonged) vomiting syncope/pre-syncope Evidence of GI blood loss
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open itpendicitis) Sever pain out of proportion (ischemic bowel, pancreatitis) restless/writhing (biliary/renal colic, testicular torsion) LLQ tenderness (diverticulitis) <span>Rectal & pelvic exams if lower abdo & pelvic pain DRE - fecal impaction, palpable mass, occult blood in stool Tenderness & fullness on R of rectum suggests retrocecal appendix Pelvic - vaginal discharge (vaginitis), cervical motion tenderness & peritoneal signs (ectopic pregnancy or other gyne complications e.g. tubo-ovarian abscess) <span><body><html>
Original toplevel document
Abdo PainCholecystitis (highest to lowest PPV) RUQ pain, fever, jaundice IBS algorithm <span>Objective General inspection Change in mental status (infection - UTI) Shock (perforated viscera, GI hemorrhage, severe pancreatitis, MI, sepsis) Vitals Upper abdo pain - pay attention to Cardiac (ischemia) & lung (pneumonia) exams Tachypneic (pneumonia) Abdo peritoneal signs Carnett’s sign (high ppv for abdo wall pain) ↑ pain when supine pt raises head & shoulder, tensing abdo wall Murphy’s sign (high ppv for choleycystitis) Psoas sign (high ppv for appendicitis) Sever pain out of proportion (ischemic bowel, pancreatitis) restless/writhing (biliary/renal colic, testicular torsion) LLQ tenderness (diverticulitis) Rectal & pelvic exams if lower abdo & pelvic pain DRE - fecal impaction, palpable mass, occult blood in stool Tenderness & fullness on R of rectum suggests retrocecal appendix Pelvic - vaginal discharge (vaginitis), cervical motion tenderness & peritoneal signs (ectopic pregnancy or other gyne complications e.g. tubo-ovarian abscess) S&S of surgical abdo Fever Protracted (prolonged) vomiting syncope/pre-syncope Evidence of GI blood loss
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
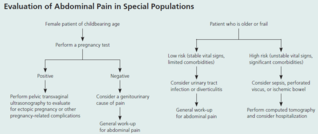
Open itPlan (for acute abdo pain) - acute abdo = sudden, non-traumatic disorder needing urgent dx & tx Labs CBC (infection/blood loss) Amylase + lipase (pancreatitis) LFT (RUQ pain) Urinalysis (hematuria, dysuria, flank pain - UTI/kidney stone) Beta hcg (women in childbearing age) Chlamydia + gonorrhea (women @ risk of STIs) Imaging (based on location) U/S (RUQ pain) abdo/transvag ultrasound for pregnant women, even for LLQ/RLQ pain Transvag u/s for ectop
Original toplevel document
Abdo Pain#13; Appendicitis Acute cholecystitis Diverticulitis Acute pancreatitis Perforated ulcer Bowel infarction <span>Plan (for acute abdo pain) - acute abdo = sudden, non-traumatic disorder needing urgent dx & tx Labs CBC (infection/blood loss) Amylase + lipase (pancreatitis) LFT (RUQ pain) Urinalysis (hematuria, dysuria, flank pain - UTI/kidney stone) Beta hcg (women in childbearing age) Chlamydia + gonorrhea (women @ risk of STIs) Imaging (based on location) U/S (RUQ pain) abdo/transvag ultrasound for pregnant women, even for LLQ/RLQ pain Transvag u/s for ectopic pregnancy CT w/ IV contrast media (adults w/ acute RLQ pain) CT w/ oral + IV contrast media (LLQ pain) - for sigmoid diverticulitis LUQ pain (many causes so depends) Suggested esophageal/gastric patho = endoscopy or upper GI series Others = CT (can image pancreas, spleen, kidneys, intestines, vasculature) Xray Free air under diaphragm (=perforation of GI tract) Abn calcifications (10% gallstones, 90% kidney stones) Mult dilated loops of bowel & air-fluid lvls (bowel obstruction) May see with paralytic ileus *occult UTI, perforated viscus, ischemic bowel ds* - potentially fatal, often missed or dx late in elderly pt CONSIDER IN ALL OLDER PTS w/ abdo pain Initial investigations & basic management for chr/recurrent abdo pain IBS Exercise: vigorous 3-5/week (all types of IBS)
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open ititis) LFT (RUQ pain) Urinalysis (hematuria, dysuria, flank pain - UTI/kidney stone) Beta hcg (women in childbearing age) Chlamydia + gonorrhea (women @ risk of STIs) <span>Imaging (based on location) U/S (RUQ pain) abdo/transvag ultrasound for pregnant women, even for LLQ/RLQ pain Transvag u/s for ectopic pregnancy CT w/ IV contrast media (adults w/ acute RLQ pain) CT w/ oral + IV contrast media (LLQ pain) - for sigmoid diverticulitis LUQ pain (many causes so depends) Suggested esophageal/gastric patho = endoscopy or upper GI series Others = CT (can image pancreas, spleen, kidneys, intestines, vasculature) Xray Free air under diaphragm (=perforation of GI tract) Abn calcifications (10% gallstones, 90% kidney stones) Mult dilated loops of bowel & air-fluid lvls (bowel obstruction) May see with paralytic ileus *occult UTI, perforated viscus, ischemic bowel ds* - potentially fatal, often missed or dx late in elderly pt CONSIDER IN ALL OLDER PTS w/ abdo pain<span></bo
Original toplevel document
Abdo Pain#13; Appendicitis Acute cholecystitis Diverticulitis Acute pancreatitis Perforated ulcer Bowel infarction <span>Plan (for acute abdo pain) - acute abdo = sudden, non-traumatic disorder needing urgent dx & tx Labs CBC (infection/blood loss) Amylase + lipase (pancreatitis) LFT (RUQ pain) Urinalysis (hematuria, dysuria, flank pain - UTI/kidney stone) Beta hcg (women in childbearing age) Chlamydia + gonorrhea (women @ risk of STIs) Imaging (based on location) U/S (RUQ pain) abdo/transvag ultrasound for pregnant women, even for LLQ/RLQ pain Transvag u/s for ectopic pregnancy CT w/ IV contrast media (adults w/ acute RLQ pain) CT w/ oral + IV contrast media (LLQ pain) - for sigmoid diverticulitis LUQ pain (many causes so depends) Suggested esophageal/gastric patho = endoscopy or upper GI series Others = CT (can image pancreas, spleen, kidneys, intestines, vasculature) Xray Free air under diaphragm (=perforation of GI tract) Abn calcifications (10% gallstones, 90% kidney stones) Mult dilated loops of bowel & air-fluid lvls (bowel obstruction) May see with paralytic ileus *occult UTI, perforated viscus, ischemic bowel ds* - potentially fatal, often missed or dx late in elderly pt CONSIDER IN ALL OLDER PTS w/ abdo pain Initial investigations & basic management for chr/recurrent abdo pain IBS Exercise: vigorous 3-5/week (all types of IBS)
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open itAbn calcifications (10% gallstones, 90% kidney stones) Mult dilated loops of bowel & air-fluid lvls (bowel obstruction) May see with paralytic ileus <span>*occult UTI, perforated viscus, ischemic bowel ds* - potentially fatal, often missed or dx late in elderly pt CONSIDER IN ALL OLDER PTS w/ abdo pain<span><body><html>
Original toplevel document
Abdo Pain#13; Appendicitis Acute cholecystitis Diverticulitis Acute pancreatitis Perforated ulcer Bowel infarction <span>Plan (for acute abdo pain) - acute abdo = sudden, non-traumatic disorder needing urgent dx & tx Labs CBC (infection/blood loss) Amylase + lipase (pancreatitis) LFT (RUQ pain) Urinalysis (hematuria, dysuria, flank pain - UTI/kidney stone) Beta hcg (women in childbearing age) Chlamydia + gonorrhea (women @ risk of STIs) Imaging (based on location) U/S (RUQ pain) abdo/transvag ultrasound for pregnant women, even for LLQ/RLQ pain Transvag u/s for ectopic pregnancy CT w/ IV contrast media (adults w/ acute RLQ pain) CT w/ oral + IV contrast media (LLQ pain) - for sigmoid diverticulitis LUQ pain (many causes so depends) Suggested esophageal/gastric patho = endoscopy or upper GI series Others = CT (can image pancreas, spleen, kidneys, intestines, vasculature) Xray Free air under diaphragm (=perforation of GI tract) Abn calcifications (10% gallstones, 90% kidney stones) Mult dilated loops of bowel & air-fluid lvls (bowel obstruction) May see with paralytic ileus *occult UTI, perforated viscus, ischemic bowel ds* - potentially fatal, often missed or dx late in elderly pt CONSIDER IN ALL OLDER PTS w/ abdo pain Initial investigations & basic management for chr/recurrent abdo pain IBS Exercise: vigorous 3-5/week (all types of IBS)
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1401981373708
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itPain relief w/ bowel mvnt, More freq stools w/ onset of pain, Loose stools w/ onset of pain, Passage of mucus, Sensation of incomplete evacuation, abdo distention Manning criteria (3 or more of) for IBS
Original toplevel document
Abdo Pain; Not just hx of fever/ds, physical findings too (e.g. distention, tenderness, rectal blood, etc) Onset, duration, severity, quality, exacerbating/remitting factors <span>Pain relief w/ bowel mvnt, More freq stools w/ onset of pain, Loose stools w/ onset of pain, Passage of mucus, Sensation of incomplete evacuation, abdo distention Manning criteria (3 or more of) for IBS Red flags New onset of pain, Change in pain, Altered bowel habits in elderly Check if all 3 are particular to elderly, or just the altered
Flashcard 1401983733004
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itS&S of surgical abdo Fever Protracted (prolonged) vomiting syncope/pre-syncope Evidence of GI blood loss
Original toplevel document
Abdo Painretrocecal appendix Pelvic - vaginal discharge (vaginitis), cervical motion tenderness & peritoneal signs (ectopic pregnancy or other gyne complications e.g. tubo-ovarian abscess) <span>S&S of surgical abdo Fever Protracted (prolonged) vomiting syncope/pre-syncope Evidence of GI blood loss Psychosocial factors assc w/ chr & recurrent abdo pain Assessment Common causes IBS (discomfort/pain assc w/ a

| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
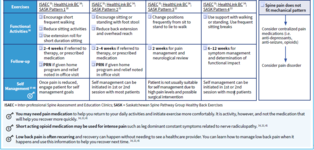
Back Pain
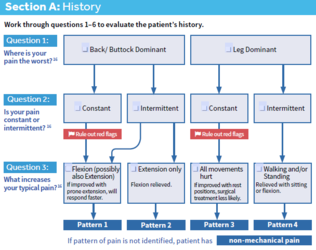
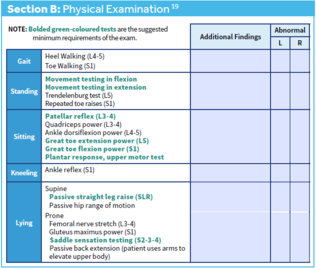
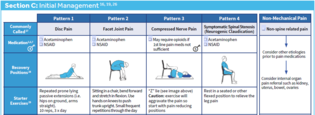
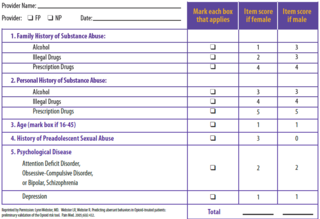
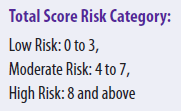
Back Pain (acute and chronic) *Just use the core back tool, it’s so good* Subjective Objective Plan Opioid Risk Tool </bod
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Back Pain
Back Pain (acute and chronic) *Just use the core back tool, it’s so good* Subjective Objective Plan Opioid Risk Tool
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Back Pain
#13; Back Pain (acute and chronic) *Just use the core back tool, it’s so good* Subjective Objective <span>Plan Opioid Risk Tool <span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Back Pain
#13; Back Pain (acute and chronic) *Just use the core back tool, it’s so good* Subjective Objective <span>Plan Opioid Risk Tool <span><body><html>
Flashcard 1402094882060
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Article 1402100387084
#has-images
D et Coaching Adjustments Manual Everything you need to succesflly cut to shreds R B JP Purchased by Richie Han, richiehanschool@gmail.com #6478326 1 Table of content Part 1 Why Successful People Don’t Just Make Random Cuts To Their Calorie Intake 4 Part 2 Forget Your Calculations - Why We Need To Track & Make Adjustments As We Diet 7 Part 3 Expect Fluctuations, Identify Stalls, And Anticipate Whooshes 10 Part 4 How I Recommend You Track Your Progress 14 Part 5 How Quickly Should I Cut? 19 Part 6 The Role Of The Diet Break 24 Part 7 When & How To Make Adjustments To Your Calorie Intake 27 Part 8 Full Examples Of How I Coached The Clients You Voted On 38 Part 9 Coming Back Up To Maintenance To Maximally Maintain Your Shreds 48 R BODY JP Purchased by Richie Han, richiehanschool@gmail.com #6478326 2 This book is not intended for the treatment or prevention of disease, nor as a substitute for medical treatment, nor as an alternative to medical advice. Use of
Flashcard 1402200788236
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
d. This can actually work fairly well if you’re pumped full of drugs that help to maintain your muscle mass, and keep your hormones in check, but for the rest of us it’s really not a good idea. Why is this not a good idea? <span>• If we slash calorie intake too much we risk losing muscle mass. - There are limits to how much fat we can lose each day, and the leaner we get, the less we can lose. More on this in part 5. • You’ll have less energy for your workouts, and without sufficient training intensity your ability to maintain your muscle mass will be hampered. • You’ll run out of places to
d. This can actually work fairly well if you’re pumped full of drugs that help to maintain your muscle mass, and keep your hormones in check, but for the rest of us it’s really not a good idea. Why is this not a good idea? <span>• If we slash calorie intake too much we risk losing muscle mass. - There are limits to how much fat we can lose each day, and the leaner we get, the less we can lose. More on this in part 5. • You’ll have less energy for your workouts, and without sufficient training intensity your ability to maintain your muscle mass will be hampered. • You’ll run out of places to