Edited, memorised or added to reading queue
on 04-Feb-2022 (Fri)
Do you want BuboFlash to help you learning these things? Click here to log in or create user.
Flashcard 7055697906956
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 7055701839116
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 7055705771276
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 7055711014156

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 7055712324876
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 7055715470604

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
sis".) DEFINITION AND TERMINOLOGY — The American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5) lists five key features that characterize <span>delirium [3]: ●Disturbance in attention (reduced ability to direct, focus, sustain, and shift attention) and awareness. ●The disturbance develops over a short period of time (usually hours to days), represents a change from baseline, and tends to fluctuate during the course of the day. ●An additional disturbance in cognition (memory deficit, disorientation, language, visuospatial ability, or perception). ●The disturbances are not better explained by another preexisting, evolving, or established neurocognitive disorder, and do not occur in the context of a severely reduced level of arousal, such as coma. ●There is evidence from the history, physical examination, or laboratory findings that the disturbance is caused by a medical condition, substance intoxication or withdrawal, or medication side effect. Additional features that may accompany delirium and confusion include the following: ●Psychomotor behavioral disturbances such as hypoactivity, hyperactivity with increased sympathetic
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
s evidence from the history, physical examination, or laboratory findings that the disturbance is caused by a medical condition, substance intoxication or withdrawal, or medication side effect. <span>Additional features that may accompany delirium and confusion include the following: ●Psychomotor behavioral disturbances such as hypoactivity, hyperactivity with increased sympathetic activity, and impairment in sleep duration and architecture. ●Variable emotional disturbances, including fear, depression, euphoria, or perplexity. There is no generally accepted consensus regarding the distinction between delirium and confusional states. The terms "acute confusional state" and "encephalopathy" are often used synon
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ates. The terms "acute confusional state" and "encephalopathy" are often used synonymously with delirium. The more general term "confusion" is used to indicate a problem with coherent thinking. <span>Confused patients are unable to think with normal speed, clarity, or coherence [4]. Confusion is typically associated with a depressed sensorium and a reduced attention span, and it is an essential component of delirium. The term "acute confusional state" refers to an acute state of altered consciousness characterized by disordered attention along with diminished speed, clarity, and coherence of thought
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
nerally accepted consensus regarding the distinction between delirium and confusional states. The terms "acute confusional state" and "encephalopathy" are often used synonymously with delirium. <span>The more general term "confusion" is used to indicate a problem with coherent thinking. Confused patients are unable to think with normal speed, clarity, or coherence [4]. Confusion is typically associated with a depressed sensorium and a reduced attention span, and it is an essential component of delirium. The term "acute confusional state" refers to an acute state of altered consciousness characterized by disordered attention along with diminished speed, clarity, and coherence of thought [4]. Although this definition encompasses delirium as well, some experts use "confusional state" to convey the additional meaning of reduced alertness and altered psychomotor activity [4]. In this paradigm, delirium is a special type of confusional state characterized by increased vigilance, with psychomotor and autonomic overactivity; the delirious patient displays agitation, excitement, tremulousness, hallucinations, fantasies, and delusions. In this discussion, the term "delirium" will be used in the sense of the DSM-5 definition. The additional components of agitation, tremor, and hallucinations are allowed for but are not
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
l, in which low-voltage, fast-wave activity predominated. These findings are so consistent that EEG can be used to resolve uncertainty in patients in whom the diagnosis of delirium is in doubt. <span>The results of brainstem auditory evoked potential, somatosensory evoked potentials, and neuroimaging studies have supported an important role for subcortical (eg, thalamus, basal ganglia, and pontine reticular formation) as well as cortical structures in the pathogenesis of delirium [13]. These findings correlate with clinical reports that patients with subcortical strokes and basal ganglia abnormalities (including Parkinson disease) have a higher susceptibility to delirium. Neurotransmitter and humoral mechanisms — Acetylcholine plays a key role in the pathogenesis of delirium [14,15]. Anticholinergic drugs cause delirium when given to healthy volunteers a
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
reports that patients with subcortical strokes and basal ganglia abnormalities (including Parkinson disease) have a higher susceptibility to delirium. Neurotransmitter and humoral mechanisms — <span>Acetylcholine plays a key role in the pathogenesis of delirium [14,15]. Anticholinergic drugs cause delirium when given to healthy volunteers and are even more likely to lead to acute confusion in frail older adults. This effect can be reversed with cholinesterase inhibitors such as physostigmine. (See "Anticholinergic poisoning".) Further support for the role of acetylcholine is derived from observations that medical conditions precipitating delirium, such as hypoxia, hypoglycemia, and thiamine deficiency, decrea
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
s and are even more likely to lead to acute confusion in frail older adults. This effect can be reversed with cholinesterase inhibitors such as physostigmine. (See "Anticholinergic poisoning".) <span>Further support for the role of acetylcholine is derived from observations that medical conditions precipitating delirium, such as hypoxia, hypoglycemia, and thiamine deficiency, decrease acetylcholine synthesis in the central nervous system (CNS). In addition, serum anticholinergic activity, measured with binding assays employing purified preparations of brain muscarinic receptors, correlates with the severity of delirium in postoperative and medical patients [14,16]. Finally, Alzheimer disease, which is characterized by a loss of cholinergic neurons, increases the risk of delirium due to anticholinergic medications. The anticholinergic mechanism is important for clinicians to keep in mind, since many drugs used by older adults (including several not traditionally viewed to have "anticholinergic eff
Flashcard 7055729888524
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
in), endorphins, serotonin, norepinephrine, and gamma-aminobutyric acid (GABA), among others [13]. However, it is difficult to exclude the confounding effects of underlying illness or dementia. <span>Proinflammatory cytokines such as interleukins and tumor necrosis factor-alpha also may have a role in the pathogenesis of delirium. These agents have strong CNS effects when injected into experimental animals or when administered for therapeutic purposes (eg, interferons in chronic hepatitis). Cytokine activation may account for delirium (particularly hyperactive forms of the disturbance) in situations such as sepsis (where mental changes may actually precede fever), cardiopulmonary bypass [19], and acute hip fracture [20]. Risk factors — Delirium is a multifactorial disorder. Factors that increase the risk for delirium and confusional states can be classified into those that increase baseline vulnerabilit
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
l disorder. Factors that increase the risk for delirium and confusional states can be classified into those that increase baseline vulnerability and those that precipitate the disturbance [21]. <span>The most commonly identified risk factors are underlying brain diseases such as dementia, stroke, or Parkinson disease; these are present in nearly one-half of older patients with delirium. In a meta-analysis of published prospective studies of delirium, the prevalence of delirium superimposed upon dementia ranged from 22 to 89 percent [22]. Often, the dementia went unrec
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
l disorder. Factors that increase the risk for delirium and confusional states can be classified into those that increase baseline vulnerability and those that precipitate the disturbance [21]. <span>The most commonly identified risk factors are underlying brain diseases such as dementia, stroke, or Parkinson disease; these are present in nearly one-half of older patients with delirium. In a meta-analysis of published prospective studies of delirium, the prevalence of delirium superimposed upon dementia ranged from 22 to 89 percent [22]. Often, the dementia went unrecognized prior to the onset of delirium. Similarly, in a study of 78 older patients with femoral neck fractures who were followed for five years, dementia developed in 69 percent of the 29 patients with postoperative delirium versus only 20 percent of the 49 patients without postoperative delirium [23]. Other factors that increase the vulnerability to delirium include advanced age and sensory impairment. Precipitating factors — Factors that may precipitate delirium are numerous and var
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
who were followed for five years, dementia developed in 69 percent of the 29 patients with postoperative delirium versus only 20 percent of the 49 patients without postoperative delirium [23]. <span>Other factors that increase the vulnerability to delirium include advanced age and sensory impairment. Precipitating factors — Factors that may precipitate delirium are numerous and varied (table 1). Some common examples include polypharmacy (particularly psychoactive drugs), infection,
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
20 percent of the 49 patients without postoperative delirium [23]. Other factors that increase the vulnerability to delirium include advanced age and sensory impairment. Precipitating factors — <span>Factors that may precipitate delirium are numerous and varied (table 1). Some common examples include polypharmacy (particularly psychoactive drugs), infection, dehydration, immobility (including restraint use), malnutrition, and the use of bladder catheters. Drugs that may precipitate delirium and confusion are noted in the table (table 2). CLINICAL PRESENTATION — As previously noted, several key features characterize delirium and confusional states (see 'Definition and terminology' above) [3]. A disturbance of consciousne
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
on are noted in the table (table 2). CLINICAL PRESENTATION — As previously noted, several key features characterize delirium and confusional states (see 'Definition and terminology' above) [3]. <span>A disturbance of consciousness and altered cognition are essential components. The condition typically develops over a short period of time and tends to fluctuate during the course of the day. The disturbance is typically caused by a medical condition, substance intoxication, or medication side effect. These criteria form a useful framework for understanding the clinical pres
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
condition, substance intoxication, or medication side effect. These criteria form a useful framework for understanding the clinical presentation of the disorder. Disturbance of consciousness — <span>One of the earliest manifestations of delirium is a change in the level of awareness and the ability to focus, sustain, or shift attention. This loss of mental clarity is often subtle and may precede more flagrant signs of delirium by one day or more. Thus, family members or caregivers who report that a patient "isn't acting quite right" should be taken seriously, even if delirium is not obvious to the examining clinician. Distractibility, one of the hallmarks of delirium, is often evident in conversation. It is important that the examiner be sensitive to the patient's flow of thought and not attribute ta
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
y one day or more. Thus, family members or caregivers who report that a patient "isn't acting quite right" should be taken seriously, even if delirium is not obvious to the examining clinician. <span>Distractibility, one of the hallmarks of delirium, is often evident in conversation. It is important that the examiner be sensitive to the patient's flow of thought and not attribute tangential or disorganized speech to age, dementia, or fatigue. Patients will appear obviously drowsy, lethargic, or even semicomatose in more advanced cases of delirium. The opposite extreme, hypervigilance, may also occur in cases of alcohol or se
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
often evident in conversation. It is important that the examiner be sensitive to the patient's flow of thought and not attribute tangential or disorganized speech to age, dementia, or fatigue. <span>Patients will appear obviously drowsy, lethargic, or even semicomatose in more advanced cases of delirium. The opposite extreme, hypervigilance, may also occur in cases of alcohol or sedative drug withdrawal, but such a presentation is less common in older persons. (See "Management of moderate and severe alcohol withdrawal syndromes".) Change in cognition — Delirious individuals have cognitive and perceptual problems, including memory loss, disori
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
es of alcohol or sedative drug withdrawal, but such a presentation is less common in older persons. (See "Management of moderate and severe alcohol withdrawal syndromes".) Change in cognition — <span>Delirious individuals have cognitive and perceptual problems, including memory loss, disorientation, and difficulty with language and speech. Formal mental status testing can be used to document the degree of impairment, but more important than the test score are the patient's overall accessibility and attentiveness while attempting to answer the questions. It is important to ascertain the patient's level of functioning prior to the onset of delirium from family members, caregivers, or other reliable informants, since dementia can impair cognitive ability and frequently underlies delirium. Perceptual disturbances typically accompany delirium. Patients may misidentify the clinician or believe that objects or shadows in the room represent a person. Vague delusions of harm o
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
level of functioning prior to the onset of delirium from family members, caregivers, or other reliable informants, since dementia can impair cognitive ability and frequently underlies delirium. <span>Perceptual disturbances typically accompany delirium. Patients may misidentify the clinician or believe that objects or shadows in the room represent a person. Vague delusions of harm often accompany these misperceptions. Hallucinations can be visual, auditory, or somatosensory, usually with lack of insight: the patients believe they are real. Hallucinations can be simple (eg, shadows or shapes) or complex (as people and faces). Sounds can also consist of simple sounds or hearing voices with clear speech. A variety of language difficulties can occur. Patients may lose the ability to write or to speak a second language. One personal experience involved a patient who immigrated to North Am
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ients believe they are real. Hallucinations can be simple (eg, shadows or shapes) or complex (as people and faces). Sounds can also consist of simple sounds or hearing voices with clear speech. <span>A variety of language difficulties can occur. Patients may lose the ability to write or to speak a second language. One personal experience involved a patient who immigrated to North America as an adolescent; she spoke only Italian during her delirium, recovering her grasp of English after her pneumonia was treated. Temporal course — Delirium develops over hours to days and typically persists for days to months. The acuteness of the presentation is the most helpful feature in differentiating deliri
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
volved a patient who immigrated to North America as an adolescent; she spoke only Italian during her delirium, recovering her grasp of English after her pneumonia was treated. Temporal course — <span>Delirium develops over hours to days and typically persists for days to months. The acuteness of the presentation is the most helpful feature in differentiating delirium from dementia. In addition, the features of delirium are unstable, typically becoming most severe in the evening and at night. It is not unusual for a patient with delirium to appear relatively lucid during morning rounds. Clinicians, particularly physicians, are apt to miss the diagnosis if they rely upon only a single-point assessment; evidence of the behavior change should be actively solicited from all staff, especially those working evening and night shifts. There is often a prodromal phase, especially in older patients, that later blends into quiet/hypoactive delirium or erupts into an agitated confusional state. Prodromal features include
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
s the diagnosis if they rely upon only a single-point assessment; evidence of the behavior change should be actively solicited from all staff, especially those working evening and night shifts. <span>There is often a prodromal phase, especially in older patients, that later blends into quiet/hypoactive delirium or erupts into an agitated confusional state. Prodromal features include complaints of fatigue, sleep disturbance (excessive daytime somnolence or insomnia), depression, anxiety, restlessness, irritability, and hypersensitivity to light or sound. With progression there are perceptual disturbances and cognitive impairment. These symptoms may fluctuate. Hypoactive delirium can, however, begin without a prodromal phase, and agitated behavior may appear as the first manifestation of delirium without a prodromal or hypoactive phase. Older
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
pression, anxiety, restlessness, irritability, and hypersensitivity to light or sound. With progression there are perceptual disturbances and cognitive impairment. These symptoms may fluctuate. <span>Hypoactive delirium can, however, begin without a prodromal phase, and agitated behavior may appear as the first manifestation of delirium without a prodromal or hypoactive phase. Older patients — Patients with delirium are sick by definition. However, older patients with delirium often do not look sick apart from their behavioral change. Thus, delirium may be th
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
oactive delirium can, however, begin without a prodromal phase, and agitated behavior may appear as the first manifestation of delirium without a prodromal or hypoactive phase. Older patients — <span>Patients with delirium are sick by definition. However, older patients with delirium often do not look sick apart from their behavioral change. Thus, delirium may be the only finding suggesting acute illness in older demented patients. Caregivers must be educated that sudden changes in mental functioning are not expected with most progressive dementias and require prompt medical attention. Other features — Delirium may present with a variety of clinical manifestations that are not essential diagnostic features, including psychomotor agitation, sleep-wake reversals, irrita
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
illness in older demented patients. Caregivers must be educated that sudden changes in mental functioning are not expected with most progressive dementias and require prompt medical attention. <span>Other features — Delirium may present with a variety of clinical manifestations that are not essential diagnostic features, including psychomotor agitation, sleep-wake reversals, irritability, anxiety, emotional lability, and hypersensitivity to lights and sounds. These features are not seen in all patients with delirium and can be evident in patients with dementia; their presence neither rules in nor rules out the diagnosis. The most common presentation in older patients is a relatively quiet, withdrawn state that frequently is mistaken for depression. The relationship between clinical manifestations and outcome has not been well studied, although a report of outcomes of delirium following hip fracture repair suggested that patients w
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
TION — There are two important aspects to the diagnostic evaluation of delirium: recognizing that the disorder is present and uncovering the underlying medical illness that has caused delirium. <span>Recognizing the disorder — As previously mentioned, clinicians often fail to recognize delirium; in some reports, this happens in more than 70 percent of cases. Behavioral problems or cognitive impairment may be readily apparent but wrongly attributed to the patient's age, to dementia, or to other mental disorders. In one study, over 40 percent of patients referred to a consulting liaison psychiatrist for the evaluation or treatment of depression ultimately were found to have delirium [24]. Clinical confirmation — The Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5) criteria (see 'Definition and terminology' above) form a practical framework for
Flashcard 7055751122188
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
tal disorders. In one study, over 40 percent of patients referred to a consulting liaison psychiatrist for the evaluation or treatment of depression ultimately were found to have delirium [24]. <span>Clinical confirmation — The Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5) criteria (see 'Definition and terminology' above) form a practical framework for assessing delirium [26]: ●A change in the level of consciousness is often the first observable clue. Clinicians must not "normalize" lethargy or somnolence by assuming that illness, sleep loss, fatigue, or anxiety are causing the changes. ●In cases where the patient appears awake, the ability to focus, sustain, or shift attention can be assessed during attempts to obtain a history; a global assessment of the patient's "accessibility" during conversation or the performance of a mental status examination is a sensitive indicator of delirium. ●Conversation with the patient may elicit memory difficulties, disorientation, or speech that is tangential, disorganized, or incoherent. The clinician should be aware of superficially appropriate conversation that follows social norms but is poor in content. ●When in doubt, formal mental status testing should be performed, such as the Mini-Mental State Examination or brief bedside tests of attention (table 3). Serial-sevens and spelling a word such as "farm" or "world" backward are other simple tests of attention. (See "The mental status examination in adults", section on 'Cognitive screening tests'.) Determining that cognitive impairment or perceptual problems are not due to a prior or progressing dementia can be challenging and requires knowledge of the patient's baseline level of
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
erial-sevens and spelling a word such as "farm" or "world" backward are other simple tests of attention. (See "The mental status examination in adults", section on 'Cognitive screening tests'.) <span>Determining that cognitive impairment or perceptual problems are not due to a prior or progressing dementia can be challenging and requires knowledge of the patient's baseline level of functioning. The diagnosis is made more easily if there has been a prior assessment of cognitive abilities. In other instances, informants must be immediately sought to establish chronology. These s
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
givers (eg, nursing staff familiar with the patient), family members, and informal caregivers, particularly those who may have observed fluctuations in the patient's mental functions. History — <span>Some historical clues to the underlying etiology of delirium and confusion can be obtained from relatives (eg, recent febrile illness, history of organ failure, a medication list, history of alcoholism or drug abuse, or recent depression). It is otherwise often difficult to impossible to obtain a history in the confused or uncooperative patient. As an example, myocardial infarction may cause sufficient confusion that the patient cannot relate a history of chest pain. General examination — A comprehensive physical examination is often difficult or impossible in the confused or uncooperative patient. Clinicians should instead perform a focused assessm
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ossible to obtain a history in the confused or uncooperative patient. As an example, myocardial infarction may cause sufficient confusion that the patient cannot relate a history of chest pain. <span>General examination — A comprehensive physical examination is often difficult or impossible in the confused or uncooperative patient. Clinicians should instead perform a focused assessment, concentrating upon vital signs, the state of hydration, skin condition, and potential infectious foci. The patient's general appearance may be suggestive (eg, the dusky appearance seen with chronic pulmonary disease, the jaundiced appearance of hepatic failure, or the stigmata of renal f
Flashcard 7055758200076
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
confused or uncooperative patient. Clinicians should instead perform a focused assessment, concentrating upon vital signs, the state of hydration, skin condition, and potential infectious foci. <span>The patient's general appearance may be suggestive (eg, the dusky appearance seen with chronic pulmonary disease, the jaundiced appearance of hepatic failure, or the stigmata of renal failure). Needle tracks strongly suggest drug abuse. Cherry-red lips indicate possible carbon monoxide poisoning. The breath may smell of alcohol, fetor hepaticus, uremic fetor, or ketones. Hyperventilation offers a limited number of possible etiologies. (See 'Diagnostic tests' below.) A bitten tongue or posterior fracture-dislocation of the shoulder suggests a convulsive seizure (over 40 percent of such patients remain in nonconvulsive
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
monoxide poisoning. The breath may smell of alcohol, fetor hepaticus, uremic fetor, or ketones. Hyperventilation offers a limited number of possible etiologies. (See 'Diagnostic tests' below.) <span>A bitten tongue or posterior fracture-dislocation of the shoulder suggests a convulsive seizure (over 40 percent of such patients remain in nonconvulsive status epilepticus [NCSE]). There may also be signs of head injury. Subhyaloid or retinal hemorrhages raise the possibility of an intracranial hemorrhage, usually from a ruptured berry aneurysm. Alcohol or sedative-drug withdrawal may cause a delirium characterized by autonomic nervous system activation (tachycardia, sweating, flushing, dilated pupils) in younger persons, but t
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
tatus epilepticus [NCSE]). There may also be signs of head injury. Subhyaloid or retinal hemorrhages raise the possibility of an intracranial hemorrhage, usually from a ruptured berry aneurysm. <span>Alcohol or sedative-drug withdrawal may cause a delirium characterized by autonomic nervous system activation (tachycardia, sweating, flushing, dilated pupils) in younger persons, but these responses are blunted or absent in the geriatric population. Anticholinergic toxicity in older adults can cause delirium without peripheral signs of atropine poisoning (eg, fever, mydriasis, tachycardia). Sepsis may present as delirium without obvious fever (sometimes even with hypothermia) or localizing signs (eg, rebound tenderness from a perforated viscus). (See "Approach to infection in the older adult".) Pitfalls in the examination must be kept in mind: temperature may be under 38.3ºC (101ºF) even in the presence of serious infections, auscultatory and radiographic findings of pneumonia
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
sent as delirium without obvious fever (sometimes even with hypothermia) or localizing signs (eg, rebound tenderness from a perforated viscus). (See "Approach to infection in the older adult".) <span>Pitfalls in the examination must be kept in mind: temperature may be under 38.3ºC (101ºF) even in the presence of serious infections, auscultatory and radiographic findings of pneumonia may be subtle or absent, and abdominal catastrophes may present without peritoneal signs in frail older patients. False-positive findings occur as well (eg, nuchal rigidity may not signify meningitis). Neurologic examination — The neurologic examination is often confounded by inattention and altered consciousness in patients with delirium. Certain aspects of the examination may be dif
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
Certain aspects of the examination may be difficult or unreliable in uncooperative patients (eg, sensory testing), or reflect chronic rather than acute central nervous system (CNS) conditions. <span>However, an assessment emphasizing the level of consciousness, degree of attention or inattention, visual fields, and unambiguous cranial nerve and motor deficits is important to identify individuals with a higher likelihood of focal neurologic disease. Posterior cortical strokes, for example, can present as delirium with few findings other than hemianopia, and in some cases may present with no focal symptoms or signs. The absence of focal examination findings does not exclude the possibility of focal or multifocal neurologic lesions as the cause of the delirium. In the absence of an obvious cause for
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ocal neurologic disease. Posterior cortical strokes, for example, can present as delirium with few findings other than hemianopia, and in some cases may present with no focal symptoms or signs. <span>The absence of focal examination findings does not exclude the possibility of focal or multifocal neurologic lesions as the cause of the delirium. In the absence of an obvious cause for delirium, further testing including neuroimaging, lumbar puncture, and electroencephalography (EEG) is indicated. The physical signs of metabolic/toxic delirium can include nonrhythmic, asynchronous muscle jerking (multifocal myoclonus); flapping motions of an outstretched, dorsiflexed hand (asteri
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ic lesions as the cause of the delirium. In the absence of an obvious cause for delirium, further testing including neuroimaging, lumbar puncture, and electroencephalography (EEG) is indicated. <span>The physical signs of metabolic/toxic delirium can include nonrhythmic, asynchronous muscle jerking (multifocal myoclonus); flapping motions of an outstretched, dorsiflexed hand (asterixis); and postural action tremor. These are nonspecific findings and do not help establish any particular medical etiology within the metabolic/toxic category. Selective loss of the vestibular-ocular reflex, or nystagmus with unexplained ocular palsies that spare pupillary reactivity to light, raise the possibility of Wernicke encephalopathy. Clinical instruments — The Confusion Assessment Method (CAM) is a simple tool that can be used by clinicians to integrate their observations and identify when delirium is the most proba
Flashcard 7055768423692
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
of the vestibular-ocular reflex, or nystagmus with unexplained ocular palsies that spare pupillary reactivity to light, raise the possibility of Wernicke encephalopathy. Clinical instruments — <span>The Confusion Assessment Method (CAM) is a simple tool that can be used by clinicians to integrate their observations and identify when delirium is the most probable diagnosis (table 4). In medical and surgical settings, the CAM has a sensitivity of 94 to 100 percent and a specificity of 90 to 95 percent [27,28]. The CAM has become a standard screening device in clinical studies of delirium, conducted across multiple settings including emergency departments and long-term care [29]. It takes fiv
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ical condition can precipitate delirium in a susceptible person; multiple underlying conditions are often found [36]. The history and physical examination will guide most of the investigations. <span>The conditions noted most commonly in prospective studies of the disorder include: ●Fluid and electrolyte disturbances (dehydration, hyponatremia, and hypernatremia) ●Infections (urinary tract, respiratory tract, skin, and soft tissue) ●Drug or alcohol toxicity ●Withdrawal from alcohol ●Withdrawal from barbiturates, benzodiazepines, and selective serotonin reuptake inhibitors ●Metabolic disorders (hypoglycemia, hypercalcemia, uremia, liver failure, thyrotoxicosis) ●Low perfusion states (shock, heart failure) ●Postoperative states, especially in older adults Less common causes that should be considered include hypoxemia, hypercarbia, Wernicke encephalopathy, adrenal failure, primary CNS infection, seizures, trauma, and paraneoplastic syndro
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
hibitors ●Metabolic disorders (hypoglycemia, hypercalcemia, uremia, liver failure, thyrotoxicosis) ●Low perfusion states (shock, heart failure) ●Postoperative states, especially in older adults <span>Less common causes that should be considered include hypoxemia, hypercarbia, Wernicke encephalopathy, adrenal failure, primary CNS infection, seizures, trauma, and paraneoplastic syndromes. A cost-effective work-up for delirium focuses upon these most likely possibilities. Medication review — Drug toxicity accounts for approximately 30 percent of all cases of delirium [17]
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
, adrenal failure, primary CNS infection, seizures, trauma, and paraneoplastic syndromes. A cost-effective work-up for delirium focuses upon these most likely possibilities. Medication review — <span>Drug toxicity accounts for approximately 30 percent of all cases of delirium [17]. Thus, the most important initial step is a medication review. The most common offenders are listed in the table (table 2) [17]. Clinicians should be careful not to neglect over-the-counter agents, drugs prescribed by other physicians, or drugs belonging to other household members. A simple but high-yield diagnostic procedure is to ask a family member to clean out the medicine cabinet and bring the contents for review. DIFFERENTIAL DIAGNOSIS — Careful attention to the key features of acute onset, fluctuating course, altered consciousness, and cognitive decline should readily distinguish delirium from
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
and no obvious medical illness may be suffering the effects of impaired circadian regulation or nocturnal factors in the institutional environment (eg, shift changes, noise, reduced staffing). <span>Focal syndromes — A number of lobar or focal neurologic syndromes may mimic delirium. ●Temporal-parietal – Patients with Wernicke aphasia may appear delirious in that they do not comprehend or obey and seem confused. However, the problem is restricted to language, while
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
lation or nocturnal factors in the institutional environment (eg, shift changes, noise, reduced staffing). Focal syndromes — A number of lobar or focal neurologic syndromes may mimic delirium. ●<span>Temporal-parietal – Patients with Wernicke aphasia may appear delirious in that they do not comprehend or obey and seem confused. However, the problem is restricted to language, while other aspects of mental function are intact. Furthermore, fluent paraphasias are typically present with Wernicke and offer a major clue to the correct diagnosis. Bitemporal dysfunction, if transient, may produce a transient global amnesia (TGA), in which the deficit is restricted to memory. With more extensive bitemporal dysfunction, visual agnosia and cortical deafness (either bitemporal or left temporal) or the Klüver-Bucy syndrome (apathy, visual agnosia, increased sexual activity, and increased oral behavior) may be seen. ●Occipital – Anton syndrome of cortical blindness and confabulation might be confused with delirium. Careful examination, however, will reveal a lack of vision. ●Frontal – Patients with
Flashcard 7055777598732
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ual agnosia and cortical deafness (either bitemporal or left temporal) or the Klüver-Bucy syndrome (apathy, visual agnosia, increased sexual activity, and increased oral behavior) may be seen. ●<span>Occipital – Anton syndrome of cortical blindness and confabulation might be confused with delirium. Careful examination, however, will reveal a lack of vision. ●Frontal – Patients with bifrontal lesions (eg, from tumor or trauma) often show akinetic mutism, lack of spontaneity, lack of judgment, problems with recent or working memory, blunted
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
sed oral behavior) may be seen. ●Occipital – Anton syndrome of cortical blindness and confabulation might be confused with delirium. Careful examination, however, will reveal a lack of vision. ●<span>Frontal – Patients with bifrontal lesions (eg, from tumor or trauma) often show akinetic mutism, lack of spontaneity, lack of judgment, problems with recent or working memory, blunted or labile emotional responses, and incontinence. These features may closely resemble delirium. Neuroimaging may be required to differentiate frontal lesions from delirium and confusional states in difficult cases. Confusion or delirium due to acute or subacute brain lesions, such as stroke or multifocal white matter inflammation, may occur without focal deficits on examination [38-41]. One retros
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
found stroke as the cause in nine patients (7 percent) [39]. Of these, three patients (2.7 percent) with stroke had no focal neurologic findings, and one of these was a subarachnoid hemorrhage. <span>Risk factors for delirium in the setting of stroke include preexisting cognitive impairment, infection, right hemispheric stroke, anterior circulation large vessel stroke, and greater stroke severity [41]. Confusion or delirium may follow head injury even in the absence of focal neurologic deficits. Nonconvulsive status epilepticus — Nonconvulsive status epilepticus (NCSE) is underrecogni
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
responses, and incontinence. These features may closely resemble delirium. Neuroimaging may be required to differentiate frontal lesions from delirium and confusional states in difficult cases. <span>Confusion or delirium due to acute or subacute brain lesions, such as stroke or multifocal white matter inflammation, may occur without focal deficits on examination [38-41]. One retrospective study of 127 consecutive neurology consultations for isolated acute mental status change found stroke as the cause in nine patients (7 percent) [39]. Of these, three patients (2.7 percent) with stroke had no focal neurologic findings, and one of these was a subarachnoid hemorrhage. Risk factors for delirium in the setting of stroke include preexisting cognitive impairment, infection, right hemispheric stroke, anterior circulation large vessel stroke, and greater stroke severity [41]. Confusion or delirium may follow head injury even in the absence of focal neurologic deficits. Nonconvulsive status epilepticus — Nonconvulsive status epilepticus (NCSE) is underrecogni
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
for delirium in the setting of stroke include preexisting cognitive impairment, infection, right hemispheric stroke, anterior circulation large vessel stroke, and greater stroke severity [41]. <span>Confusion or delirium may follow head injury even in the absence of focal neurologic deficits. Nonconvulsive status epilepticus — Nonconvulsive status epilepticus (NCSE) is underrecognized, particularly in older patients. NCSE requires an electroencephalogram (EEG) for detection
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
culation large vessel stroke, and greater stroke severity [41]. Confusion or delirium may follow head injury even in the absence of focal neurologic deficits. Nonconvulsive status epilepticus — <span>Nonconvulsive status epilepticus (NCSE) is underrecognized, particularly in older patients. NCSE requires an electroencephalogram (EEG) for detection and continuous EEG for management. Often patients show no classic ictal features, but the following features should suggest the possibility of seizures: prominent bilateral facial twitching, unexplained nystagmoid eye movements during obtunded periods, spontaneous hippus, prolonged "postictal state," automatisms (lip smacking, chewing, or swallowing movements), and acute aphasia or neglect without a structural lesion [42]. NCSE should also be considered in the absence of these findings when the etiology of a confusional state remains obscure [43]. Dementia — Dementia may sometimes be confused with delirium or confusion and vice-versa. However, characteristic differences in progression and cognitive features usually distinguish th
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
te aphasia or neglect without a structural lesion [42]. NCSE should also be considered in the absence of these findings when the etiology of a confusional state remains obscure [43]. Dementia — <span>Dementia may sometimes be confused with delirium or confusion and vice-versa. However, characteristic differences in progression and cognitive features usually distinguish these disorders. ●In contrast to delirium, cognitive change in Alzheimer disease is typically insidious, progressive, and without much fluctuation, and occurs over a much longer time (months to years). Attention is relatively intact, as are remote memories in the earlier stages. (See "Clinical features and diagnosis of Alzheimer disease", section on 'Clinical features'.) ●Dementia with Lewy bodies (DLB) is similar to Alzheimer disease but can be more easily confused with delirium because fluctuations and visual hallucinations are common and prominent. (See "Clinical features and diagnosis of dementia with Lewy bodies".) Primary psychiatric illnesses — Delirium is commonly misdiagnosed as depression. Both are associated with poor sleep and difficulty with attention or concentration. Agitated depression
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
used with delirium because fluctuations and visual hallucinations are common and prominent. (See "Clinical features and diagnosis of dementia with Lewy bodies".) Primary psychiatric illnesses — <span>Delirium is commonly misdiagnosed as depression. Both are associated with poor sleep and difficulty with attention or concentration. Agitated depression may be especially problematic. However, depression is associated with dysphoria, and there is less fluctuation than in delirium. Mania can be confused with hyperactive delirium with agitation, delusions, and psychotic behavior. However, mania is usually associated with a history of previous episodes of mania or depression. In schizophrenia, the delusions are usually highly systematized, the history is longer, and the sensorium is otherwise clear. DIAGNOSTIC TESTS Laboratory tests — A number of laboratory tests may be considered in the patient with delirium. However, the desire for diagnostic completeness can increase costs and p
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ighly systematized, the history is longer, and the sensorium is otherwise clear. DIAGNOSTIC TESTS Laboratory tests — A number of laboratory tests may be considered in the patient with delirium. <span>However, the desire for diagnostic completeness can increase costs and possibly delay the prompt treatment of more obvious disorders. Targeted testing is appropriate in most instances. ●Serum electrolytes, creatinine, glucose, calcium, complete blood count, and urinalysis and urine culture are reasonable for most patients when a cause is not immediately obvious. ●Drug
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
lirium. However, the desire for diagnostic completeness can increase costs and possibly delay the prompt treatment of more obvious disorders. Targeted testing is appropriate in most instances. ●<span>Serum electrolytes, creatinine, glucose, calcium, complete blood count, and urinalysis and urine culture are reasonable for most patients when a cause is not immediately obvious. ●Drug levels should be ordered where appropriate. However, clinicians must be aware that delirium can occur even with "therapeutic" levels of such agents as digoxin, lithium, or quinidi
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
st instances. ●Serum electrolytes, creatinine, glucose, calcium, complete blood count, and urinalysis and urine culture are reasonable for most patients when a cause is not immediately obvious. <span>●Drug levels should be ordered where appropriate. However, clinicians must be aware that delirium can occur even with "therapeutic" levels of such agents as digoxin, lithium, or quinidine. ●Toxic screen of blood and urine should be obtained from patients with acute delirium or confusion when a cause is not immediately obvious. Again, clinicians must be aware that some common drugs (eg, risperidone) are not assessed in routine laboratory screens. Therefore, overdose of these drugs cannot be excluded by negative results from a toxic screen. ●Blood gas determination is often helpful. In hyperventilating patients, respiratory alkalosis is most commonly due to early sepsis, hepatic failure, early salicylate intoxication, or c
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
be aware that some common drugs (eg, risperidone) are not assessed in routine laboratory screens. Therefore, overdose of these drugs cannot be excluded by negative results from a toxic screen. ●<span>Blood gas determination is often helpful. In hyperventilating patients, respiratory alkalosis is most commonly due to early sepsis, hepatic failure, early salicylate intoxication, or cardiopulmonary causes. A metabolic acidosis usually reflects uremia, diabetic ketoacidosis, lactic acidosis, late phases of sepsis or salicylate intoxication, or toxins including methanol and ethylene glycol. A chest x-ray is usually performed. ●Further testing, such as liver function tests, should be based upon the history and clinical examination. A report of slow cognitive decline over several months, for example, will incr
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
reflects uremia, diabetic ketoacidosis, lactic acidosis, late phases of sepsis or salicylate intoxication, or toxins including methanol and ethylene glycol. A chest x-ray is usually performed. ●<span>Further testing, such as liver function tests, should be based upon the history and clinical examination. A report of slow cognitive decline over several months, for example, will increase the importance of evaluating thyroid function and vitamin B12 levels. Neuroimaging — Neuroimaging with head computed tomography (CT) may be used selectively rather than routinely for most patients with delirium. However, neuroimaging is necessary if no ob
Flashcard 7055795686668
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
and clinical examination. A report of slow cognitive decline over several months, for example, will increase the importance of evaluating thyroid function and vitamin B12 levels. Neuroimaging — <span>Neuroimaging with head computed tomography (CT) may be used selectively rather than routinely for most patients with delirium. However, neuroimaging is necessary if no obvious cause of delirium is apparent on first evaluation. The need for imaging should be guided by patient history and findings on neurologic examination. Neuroimaging may not be necessary if a patient with acute delirium meets the following c
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ever, neuroimaging is necessary if no obvious cause of delirium is apparent on first evaluation. The need for imaging should be guided by patient history and findings on neurologic examination. <span>Neuroimaging may not be necessary if a patient with acute delirium meets the following conditions: the initial clinical evaluation discloses an obvious treatable medical illness or problem, there is no evidence of trauma, no new focal neurologic signs are present, and the patient is arousable and able to follow simple commands. However, neuroimaging should be reconsidered if the patient doesn't improve as expected. Neuroimaging may still be required if the delirium does not improve despite appropriate treatment of the underlying medical problem. In addition, imaging should be considered if the neu
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
new focal neurologic signs are present, and the patient is arousable and able to follow simple commands. However, neuroimaging should be reconsidered if the patient doesn't improve as expected. <span>Neuroimaging may still be required if the delirium does not improve despite appropriate treatment of the underlying medical problem. In addition, imaging should be considered if the neurologic examination is confounded by diminished patient responsiveness or cooperation. There have been no well-designed prospective studies to assess the yield of neuroimaging in patients with delirium. Abnormalities on head CT are commonly seen, but they usually represen
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
plan in six [38]. Most studies were performed for an indication of "altered mental status" and findings included cerebral infarction in 13, intracranial hemorrhage in two, and tumor in three. ●<span>In another review of 279 head CT scans performed in the emergency department in patients older than 70 years, 42 (15 percent) revealed an acute condition [40]. Of these, 40 were found in patients with either significantly impaired consciousness (eg, unable to open eyes, speak, or follow simple commands) and/or new focal neurologic findings. Fewer data exist for magnetic resonance imaging (MRI) evaluation of patients with delirium. However, MRI is more sensitive than head CT for acute stroke, posterior fossa lesions, and wh
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
tion [40]. Of these, 40 were found in patients with either significantly impaired consciousness (eg, unable to open eyes, speak, or follow simple commands) and/or new focal neurologic findings. <span>Fewer data exist for magnetic resonance imaging (MRI) evaluation of patients with delirium. However, MRI is more sensitive than head CT for acute stroke, posterior fossa lesions, and white matter lesions; however, such findings may not influence immediate treatment course in critically ill patients [46]. In patients with delirium of unknown cause and negative head CT, MRI may be useful to exclude acute or subacute stroke and multifocal inflammatory lesions (eg, as seen in reversible posterior leukoencephalopathy and acute disseminated encephalomyelitis). Lumbar puncture — Older patients with bacterial meningitis are more likely to present with delirium rather than the classic triad of fever, headache, and meningismus. Bacterial meningit
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ful to exclude acute or subacute stroke and multifocal inflammatory lesions (eg, as seen in reversible posterior leukoencephalopathy and acute disseminated encephalomyelitis). Lumbar puncture — <span>Older patients with bacterial meningitis are more likely to present with delirium rather than the classic triad of fever, headache, and meningismus. Bacterial meningitis is an uncommon disorder, and routine cerebrospinal fluid (CSF) evaluation may not be necessary in all febrile or septic-appearing older patients with delirium as long as other infectious foci are obvious. However, CSF analysis may be the only diagnostic tool that will identify bacterial or aseptic meningitis and encephalitis. In a retrospective study of 81 older patients who were admitted to the hospital for the evaluation of fever and mental status changes, CSF cultures were negative for bacterial growth in
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
r patients with delirium as long as other infectious foci are obvious. However, CSF analysis may be the only diagnostic tool that will identify bacterial or aseptic meningitis and encephalitis. <span>In a retrospective study of 81 older patients who were admitted to the hospital for the evaluation of fever and mental status changes, CSF cultures were negative for bacterial growth in 80 of 81 patients [47]. However, one case of bacterial meningitis and one case of aseptic meningitis were diagnosed by CSF findings. In a retrospective review of 232 lumbar punctures performed in hospitalized patients for the indication of altered mental status, 11 percent were abnormal; the yield was highest in those suspected of community-acquired meningitis [48]. Lumbar puncture is mandatory when the cause of delirium is not obvious. Clinicians should also have a low threshold for obtaining CSF in febrile patients with delirium, even when alternate explanatory conditions for delirium are present or suspected. Neuroimaging should be obtained prior to lumbar puncture in patients with coma, focal signs, papilledema, or suspicion of increased intracranial pressure because of the very low but rea
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
s not obvious. Clinicians should also have a low threshold for obtaining CSF in febrile patients with delirium, even when alternate explanatory conditions for delirium are present or suspected. <span>Neuroimaging should be obtained prior to lumbar puncture in patients with coma, focal signs, papilledema, or suspicion of increased intracranial pressure because of the very low but real risk of precipitating transtentorial herniation. If lumbar puncture is delayed and the suspicion of bacterial meningitis is high, empiric antibiotic treatment should be considered. (See "Lumbar puncture: Technique, indications, contraindications, and complications in adults", section on 'Complications' and "Clinical features and diagnosis of acute bacterial mening
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
Technique, indications, contraindications, and complications in adults", section on 'Complications' and "Clinical features and diagnosis of acute bacterial meningitis in adults".) EEG testing — <span>Electroencephalography (EEG) is useful in patients with altered consciousness in order to [49,50]: ●Exclude seizures, especially nonconvulsive or subclinical seizures ●Confirm the diagnosis of certain metabolic encephalopathies or infectious encephalitides that have characteristic EEG patterns Nonconvulsive seizures lack motor manifestations or convulsions, but they may impair consciousness. Nonconvulsive status epilepticus (NCSE) may cause continuous or fluctuating impairment of consciousness, and EEG is the only method that can make the diagnosis. One report evaluated 198
Flashcard 7055808007436
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
metabolic encephalopathies or infectious encephalitides that have characteristic EEG patterns Nonconvulsive seizures lack motor manifestations or convulsions, but they may impair consciousness. <span>Nonconvulsive status epilepticus (NCSE) may cause continuous or fluctuating impairment of consciousness, and EEG is the only method that can make the diagnosis. One report evaluated 198 EEGs performed for the indication of altered consciousness without convulsions and found definite or probable NCSE in 74 (37 percent) [51]. In another study, continuous EEG monitoring was performed for unexplained decrease in consciousness or detection of subclinical seizures in 570 critically ill patients [52]. Seizures were detected in 110 patients (19 percent), and the seizures were exclusively nonconvulsive in 92 percent of these individuals. Coma patients frequently required greater than 24 hours of monitoring to detect the first electrographic seizure. Metabolic encephalopathies may show diffuse bilateral slowing of background rhythm and moderate or high-wave amplitude. Triphasic waves are associated with hepatic encephalopathy but c
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
the seizures were exclusively nonconvulsive in 92 percent of these individuals. Coma patients frequently required greater than 24 hours of monitoring to detect the first electrographic seizure. <span>Metabolic encephalopathies may show diffuse bilateral slowing of background rhythm and moderate or high-wave amplitude. Triphasic waves are associated with hepatic encephalopathy but can be seen in other severe metabolic disturbances including uremic and septic encephalopathy [53,54]. Viral encephalitis is typically associated with diffuse background slowing and occasional epileptiform activity or electrographic seizures. Herpes simplex encephalitis may be associated with high-amplitude periodic complexes in the temporal lobe leads. EEG evaluation should be obtained for any patient with altered consciousness of unknown etiology [42]. Patients with a remote or recent history of head trauma, stroke, seizures, or foca
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
kground slowing and occasional epileptiform activity or electrographic seizures. Herpes simplex encephalitis may be associated with high-amplitude periodic complexes in the temporal lobe leads. <span>EEG evaluation should be obtained for any patient with altered consciousness of unknown etiology [42]. Patients with a remote or recent history of head trauma, stroke, seizures, or focal brain lesions may be at higher risk of convulsive and nonconvulsive seizures. However, neither clinical signs nor prior history predicted which of the 198 EEGs showed nonconvulsive status in the study cited above [51]. SOCIETY GUIDELINE LINKS — Links to society and government-sponsored guidelines from selected countries and regions around the world are provided separately. (See "Society guideline link
Flashcard 7055818755340
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
is based primarily upon expert consensus and observational studies, and only a small number of controlled clinical trials, which are difficult to perform in patients with cognitive impairment. <span>The preponderance of evidence is most compelling for primary prevention of delirium using nonpharmacologic, multicomponent approaches targeted broadly at high-risk patients [1-3]. Prevention and therapy of delirium are based on the following principles: ●Avoiding factors known to cause or aggravate delirium, such as multiple medications, dehydration, immobilization, sensory impairment, and disruption of the sleep-wake cycle ●Identifying and treating the underlying acute illness ●Providing supportive and restorative care to prevent further physical and cognitive decline ●Where appropriate, controlling dangerous and severely disruptive behaviors using low-dose, short-acting pharmacologic agents so the first three steps can be accomplished The prevention, treatment, and prognosis of delirium will be reviewed here. The definition, epidemiology, pathogenesis, clinical features, and diagnosis of delirium are discussed separa
Flashcard 7055822949644
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
able risk factors appear to reduce the incidence of delirium [3,4]. Modifying risk factors — A number of factors have been identified as causing or contributing to delirium in at-risk patients. <span>Examples of interventions designed to mitigate risk factors for delirium include: ●Orientation protocols – Provision of clocks, calendars, windows with outside views, and verbally reorienting patients may mitigate confusion that results from disorientation in unfamiliar environments. ●Cognitive stimulation – Patients with cognitive impairment, in particular, may benefit from activity such as regular visits from family and friends. At the same time, sensory overstimulation should be avoided, particularly at night. ●Facilitation of physiologic sleep – Nursing and medical procedures, including the administration of medications, should be avoided during sleeping hours when possible. Night-time noise should be reduced. One randomized trial found that the use of earplugs at night was associated with a lower incidence of confusion in intensive care unit (ICU) patients [5]. ●Early mobilization and minimized use of physical restraints for patients with limited mobility – One study in mechanically ventilated, critically ill patients found that early institution of physical and occupational therapy along with consequent interruption in use of sedatives was associated with a lower number of hospital days with delirium [6]. ●Visual and hearing aids for patients with these impairments ●Avoiding and/or monitoring the use of problematic medications – Medications are often implicated in precipitating delirium, particularly in those already at risk (table 1). Benzodiazep
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
erapy along with consequent interruption in use of sedatives was associated with a lower number of hospital days with delirium [6]. ●Visual and hearing aids for patients with these impairments ●<span>Avoiding and/or monitoring the use of problematic medications – Medications are often implicated in precipitating delirium, particularly in those already at risk (table 1). Benzodiazepines, in particular, are often implicated. In one systematic review, the authors concluded that benzodiazepines should be avoided in high-risk patients, while caution should be used in prescribing opioids, dihydropyridines, and antihistamines [7]. In one large cluster-randomized control study based in nursing homes, implementation of a computerized system to identify the use of problematic medications and trigger a medication review was associated with a lower incidence of delirium (HR = 0.42) [8]. ●Avoiding and treating medical complications – A number of medical conditions are known to cause or aggravate delirium; these should be managed aggressively and prevented where possible
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
homes, implementation of a computerized system to identify the use of problematic medications and trigger a medication review was associated with a lower incidence of delirium (HR = 0.42) [8]. ●<span>Avoiding and treating medical complications – A number of medical conditions are known to cause or aggravate delirium; these should be managed aggressively and prevented where possible. Some studies have focused specifically on early volume repletion for patients with delirium. While one small study failed to show a benefit for hydration management on the incidence of delirium in a long-term care setting, the small number of patients (98) and short time period of intervention (four weeks) limited the ability of this study to demonstrate efficacy [9]. Hypoxemia and infections are other common complications in high-risk settings and patients. These may contribute to delirium and should be actively monitored for and treated when identified. An interventional program administered via a geriatric consultant team that emphasized avoiding medical complications achieved a one-third reduction in the incidence of delirium among 126 older adult patients undergoing hip surgery [10]. ●Managing pain – Pain may be a significant risk factor for delirium. The use of nonopioid medications should be used where possible, as these are less likely to aggravate delirium. Clin
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
geriatric consultant team that emphasized avoiding medical complications achieved a one-third reduction in the incidence of delirium among 126 older adult patients undergoing hip surgery [10]. ●<span>Managing pain – Pain may be a significant risk factor for delirium. The use of nonopioid medications should be used where possible, as these are less likely to aggravate delirium. Clinicians must balance the benefits of using opioids to treat significant pain with the potential for an opioid-related delirium. Nonpharmacologic interventions are appealing in this setting. In one study, fascia iliaca compartment block after hip surgery was associated with a reduced incidence of postoperative delirium in intermediate-risk, but not in high-risk, patients [1
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
d lack of information regarding long-term outcomes [13]. Ketamine does not appear to be more generally useful in the prevention of postoperative delirium, as discussed in the following section. <span>Certain classes of opioids are probably best avoided in older patients and others prone to delirium. Meperidine, in particular, has been shown in multiple prospective studies to increase the risk for delirium [14-16]. Cancer patients with terminal delirium and pain may benefit from switching from shorter-acting opioids to long-acting agents such as methadone [17]. Clinicians should also consider the possibility that opioid-induced hyperalgesia may cause breakthrough pain and should consider using nonopioid analgesia for pain control. (See "Prevention and management of side effects in patients receiving opioids for chronic pain", section on 'Opioid-induced hyperalgesia'.) Use of nursing protocols to better manage pa
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
n", section on 'Opioid-induced hyperalgesia'.) Use of nursing protocols to better manage pain has been demonstrated to reduce the severity and duration, but not the incidence, of delirium [18]. <span>In one study, a multicomponent intervention used standardized protocols to screen and control for six risk factors for delirium in 852 hospitalized patients aged 70 or older: cognitive impairment, sleep deprivation, immobility, visual impairment, hearing impairment, and dehydration [19]. Interventions such as those listed above were targeted to the identified risk factors. This program resulted in a significant reduction in the number of delirium episodes compared with usual care (62 versus 90) and in the total number of days with delirium (105 versus 161); there was no effect upon delirium severity or the rate of recurrence. The investigators have since reported that community hospitals were able to successfully implement this program when there was a commitment of resources by hospital leadership and appropriate adaptation of protocols to local needs [20]. Subsequent randomized studies have confirmed that such multicomponent interventions can reduce the incidence of delirium and/or related complications [3,21-23]. Medications to prevent delirium — The available evidence does not support the use of medications to prevent delirium in high-risk settings such as acute care, intensive care, cardiac su
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
,29]. However, clinical trials have not demonstrated a reduction in the prevalence or incidence of delirium, and side effects have been greater in patients receiving these medications [29-33]. ●<span>Antipsychotic agents, given prophylactically and in low dose, have been studied in the postoperative and critical care setting, and have been associated with inconsistent and, at best, modest benefits in the incidence, severity, and duration of delirium [34-40]. In one of these studies, treatment was associated with increased severity and longer duration of delirium [39]. A 2013 systematic review and meta-analysis of six studies concluded that such treatment reduced the incidence of delirium, but not the severity or duration; nor was the incidence of associated adverse events reduced [37]. In this analysis, second-generation antipsychotics appeared to be more beneficial compared with haloperidol. ●Dexmedetomidine administration has been studied in the treatment and prevention of delirium in the postoperative and critical care setting, with mixed results. In one randomized trial,
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
are, intensive care, cardiac surgery, or other postoperative care [24-27]. Investigators continue to study the potential benefit of cholinesterase inhibitors, antipsychotic agents, and others: ●<span>Cholinesterase inhibitors (eg, rivastigmine, donepezil) have been proposed as a means to prevent delirium in selected patients and high-risk settings (eg, older patients with or without dementia, postoperative and poststroke settings) [28,29]. However, clinical trials have not demonstrated a reduction in the prevalence or incidence of delirium, and side effects have been greater in patients receiving these medications [29-33]. ●Antipsychotic agents, given prophylactically and in low dose, have been studied in the postoperative and critical care setting, and have been associated with inconsistent and, at best,
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
rcent; OR 0.35, 95% CI 0.22-0.54). Some, but not all, studies have found similar results [41-43]. Adverse effects of dexmedetomidine include dose-dependent bradycardia and hypotension [44-46]. ●<span>Gabapentin, in pilot study, reduced the incidence of postoperative delirium, perhaps by reducing pain and opioid administration [47]. ●Melatonin has shown inconsistent efficacy in the prevention of delirium. In two small trials in older inpatients (67,145 patients) with medical illness, the melatonin agonists, ramelte
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ifference in delirium incidence between the ketamine and placebo groups [52]. Negative experiences such as hallucinations and nightmares were higher in patients receiving ketamine. MANAGEMENT — <span>The principles underlying the management of delirium are summarized in the algorithm (algorithm 1). The algorithm includes two pathways that are followed simultaneously: one to manage the behavior disturbance, and another to find and treat the underlying medical disorder. An important caveat is that the symptoms of delirium can have a prolonged duration, extending many weeks into the postacute period after the underlying causes and risk factors have been corrected. Treatment of underlying conditions — Virtually any medical condition can precipitate delirium in a susceptible patient; multiple underlying conditions are often found [53]. When the und
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ness responsible for delirium is identified, specific therapy is directed toward the medical condition. (See "Acute toxic-metabolic encephalopathy in adults", section on 'Specific etiologies'.) <span>The conditions noted most commonly in prospective studies of delirium include: ●Metabolic encephalopathy – These include the following, which are discussed in detail separately. (See "Acute toxic-metabolic encephalopathy in adults".) •Fluid and electrolyte disturbances (dehydration, hyponatremia/hypernatremia, hypo/hypercalcemia) •Infections (sepsis, urinary tract, respiratory tract, skin and soft-tissue) •Organ failure (uremia, liver failure, hypoxemia/hypercarbia) •Hypoglycemia ●Drug toxicity – Drug toxicity causes or contributes to approximately 30 percent of all cases of delirium (table 1) [54]. Clinicians must be aware that delirium can occur even with "therapeutic" levels of such agents as digoxin or lithium, particularly in at-risk patients. Certain acute drug-poisoning syndromes can be rapidly treated with the appropriate antidote. (See "General approach to drug poisoning in adults".) ●Withdrawal from alcohol and sedatives – The treatment of alcohol withdrawal is discussed separately. (See "Management of moderate and severe alcohol withdrawal syndromes", section on 'Management'.) While Wernicke encephalopathy is not common, many older hospitalized patients have biochemical evidence of thiamine deficiency [55]. In addition, chronic alcoholism is often difficult t
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
drawal from alcohol and sedatives – The treatment of alcohol withdrawal is discussed separately. (See "Management of moderate and severe alcohol withdrawal syndromes", section on 'Management'.) <span>While Wernicke encephalopathy is not common, many older hospitalized patients have biochemical evidence of thiamine deficiency [55]. In addition, chronic alcoholism is often difficult to detect in this population, and symptoms of persistent alcoholic delirium may be difficult to distinguish from those of Wernicke encephalopathy [56]. Thiamine supplementation is inexpensive and virtually risk free; it should be provided to all hospitalized patients with evidence of nutritional deficiency. (See "Wernicke encephalopathy".) Supportive medical care — The delirious patient is at risk for complications of immobility and confusion, leading to a high prevalence of irreversible functional decline. It has long be
Flashcard 7055838416140
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
d comprehensive intervention to treat underlying causes and prevent subsequent complications such as immobility, aspiration, and skin breakdown. Unfortunately, there are few controlled studies. <span>One study found that early identification and comprehensive geriatric consultation for patients with established delirium had little impact on length of stay, functional outcome, or survival [57]; another found that multicomponent interventions shortened the duration of delirium but had no impact on mortality or nursing home use [58]. Stronger evidence supports the use of these interdisciplinary efforts for prevention of delirium. (See 'Modifying risk factors' above.) Nonetheless, an interdisciplinary approach to delirium should focus upon maintaining adequate hydration and nutrition, enhancing mobility and range of motion, treating pain and discomfo
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
but had no impact on mortality or nursing home use [58]. Stronger evidence supports the use of these interdisciplinary efforts for prevention of delirium. (See 'Modifying risk factors' above.) <span>Nonetheless, an interdisciplinary approach to delirium should focus upon maintaining adequate hydration and nutrition, enhancing mobility and range of motion, treating pain and discomfort, preventing skin breakdown, ameliorating incontinence (seen in over half of delirious patients), and minimizing the risk of aspiration pneumonitis. This team approach should also include family or other caregivers who may feel frightened or exhausted; delirium can be the "last straw" for those who have been caring for the demented.
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
y or other caregivers who may feel frightened or exhausted; delirium can be the "last straw" for those who have been caring for the demented. Caregiver resources must be realistically assessed. <span>Because delirium may require weeks or months to fully resolve, management often extends into subacute settings [59,60]. Transfers of care to new settings are periods of particular vulnerability for older patients, and it is important to effectively communicate information about mental status to the accepting treatment team [61]. Managing agitation — Managing disruptive behavior, particularly agitation and combative behavior, is a challenging aspect of delirium therapy. This hyperactive delirium is less common i
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
periods of particular vulnerability for older patients, and it is important to effectively communicate information about mental status to the accepting treatment team [61]. Managing agitation — <span>Managing disruptive behavior, particularly agitation and combative behavior, is a challenging aspect of delirium therapy. This hyperactive delirium is less common in older patients and, when it occurs, alternates with periods of hypoactive delirium, which may be less obvious to the clinical staff [62]. Periods of disruptive and hyperactive behavior place the patient at risk for falls, wandering off, or inadvertently removing intravenous lines and feeding tubes. When delirium is manifest by agitation, symptom control is occasionally necessary to prevent harm or to allow evaluation and treatment. While nonpharmacologic interventions should be th
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ous to the clinical staff [62]. Periods of disruptive and hyperactive behavior place the patient at risk for falls, wandering off, or inadvertently removing intravenous lines and feeding tubes. <span>When delirium is manifest by agitation, symptom control is occasionally necessary to prevent harm or to allow evaluation and treatment. While nonpharmacologic interventions should be the mainstay of treatment, a cautious trial of psychotropic medication may be warranted in these circumstances. Unfortunately, there are limited data to guide treatment as the available studies have significant methodologic limitations [25,26]. It has also been observed that use of psychotropic medication to manage delirium appears to correlate more strongly with caregiver distress than with the actual severity of delirium symptoms [63]. Nonpharmacologic interventions — Mild confusion and agitation may respond to interpersonal and environmental manipulations. The hospital environment, characterized by high ambient noise
Flashcard 7055848115468
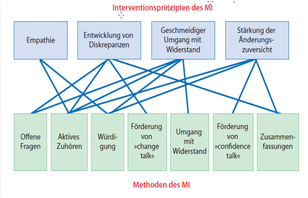
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 7055852834060
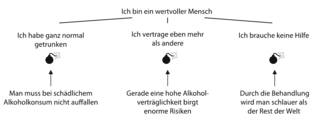
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
tters can also be used to effect. Delusions and hallucinations should be neither endorsed nor challenged. Other specific interventions are discussed above. (See 'Modifying risk factors' above.) <span>Physical restraints should be used only as a last resort, if at all, as they frequently increase agitation and create additional problems, such as loss of mobility, pressure ulcers, aspiration, and prolonged delirium. In one study, restraint use among patients in a medical inpatient unit was associated with a threefold increased odds of persistent delirium at time of hospital discharge [65]. Alternatives to restraint use, such as constant observation (preferably by someone familiar to the patient such as a family member), may be more effective. Antipsychotic medications — When indicated, antipsychotic agents are generally used to treat severe agitation in the patient with delirium, because these symptoms are associated with se
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
rge [65]. Alternatives to restraint use, such as constant observation (preferably by someone familiar to the patient such as a family member), may be more effective. Antipsychotic medications — <span>When indicated, antipsychotic agents are generally used to treat severe agitation in the patient with delirium, because these symptoms are associated with self-harm and effective alternatives are not available. No medication is currently approved by the US Food and Drug Administration (FDA) for the management of delirium, so the use of these agents for such an indication is off-label. Based on limited evidence, we suggest low-dose haloperidol (0.5 to 1 mg) be used as needed to control moderate to severe agitation or psychotic symptoms, up to a maximum dose of 5 mg pe
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
e not available. No medication is currently approved by the US Food and Drug Administration (FDA) for the management of delirium, so the use of these agents for such an indication is off-label. <span>Based on limited evidence, we suggest low-dose haloperidol (0.5 to 1 mg) be used as needed to control moderate to severe agitation or psychotic symptoms, up to a maximum dose of 5 mg per day. Continuous or prophylactic dosing is not recommended. Higher doses may be used in closely monitored settings (intensive care unit [ICU]) where the goals and sedation needs are different (see "Sedative-analgesic medications in critically ill adults: Properties, dosage regimens, and adverse effects", section on 'Antipsychotics'). Haloperidol can be administered orally, i
Flashcard 7055858339084
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
where the goals and sedation needs are different (see "Sedative-analgesic medications in critically ill adults: Properties, dosage regimens, and adverse effects", section on 'Antipsychotics'). <span>Haloperidol can be administered orally, intramuscularly (IM), or intravenously. The onset of action may be as soon as 5 to 20 minutes after intravenous administration or longer with the IM or oral route. An immediate response is not expected. Intravenous haloperidol has been associated with clinically significant QT prolongation requiring additional precautions with its use. (See "Acquired long QT syndrome: Definitions, causes, and pathophysiology", section on 'Medications'.) We recommend only short-term use of antipsychotic agents, as these agents have bee
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
with clinically significant QT prolongation requiring additional precautions with its use. (See "Acquired long QT syndrome: Definitions, causes, and pathophysiology", section on 'Medications'.) <span>We recommend only short-term use of antipsychotic agents, as these agents have been associated with a higher risk of mortality and possibly stroke when used in patients with dementia [66]. (See "Management of neuropsychiatric symptoms of dementia".) Data supporting the use of antipsychotic agents for managing delirium are limited [25,67,68]. In one of the largest randomiz
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
aller trials have suggested that these agents may reduce the severity of delirium episodes [34,70,71], but overall, the evidence supporting the use of pharmacologic agents is inconclusive [27]. <span>Because of the longer clinical experience with haloperidol, it remains the standard therapy in this setting [72]. The newer atypical antipsychotic agents, quetiapine, risperidone, ziprasidone, and olanzapine, have fewer side effects in other clinical settings, and in small studies they appear to have similar efficacy to haloperidol [73-75]. A meta-analysis of three small studies that compared haloperidol with risperidone and olanzapine found that the three agents were similarly effective in treating delirium [76]. A small clinical trial compared escalating doses of quetiapine with placebo as add-on treatment to as-needed haloperidol in 36 patients in the ICU with delirium [77]. Quetiapine was associated with a shorter duration of delirium, reduced agitation, and higher rates of discharge to home after hospitalization. By contrast, a randomized trial comparing haloperidol, ziprasidone, and placebo in ICU patients found that active treatment did not improve outcomes when measured by number of days alive without altered mental status or the incidence of adverse events [68]. Extrapyramidal side effects are higher in patients treated with high-dose haloperidol (>4.5 mg per day), but were similar among patients treated with low-dose haloperidol, olanzapine
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ne, and placebo in ICU patients found that active treatment did not improve outcomes when measured by number of days alive without altered mental status or the incidence of adverse events [68]. <span>Extrapyramidal side effects are higher in patients treated with high-dose haloperidol (>4.5 mg per day), but were similar among patients treated with low-dose haloperidol, olanzapine, and risperidone in one study [76,78]; in general, haloperidol should be avoided in favor of atypical antipsychotics in patients with parkinsonism. Sedation and hypotension can also occur as a side effect of these medications [77]. (See "Prognosis and treatment of dementia with Lewy bodies" and "Management of nonmotor symptoms in Parkinson disease".) Benzodiazepines — Benzodiazepines have a limited role in the tr
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
also occur as a side effect of these medications [77]. (See "Prognosis and treatment of dementia with Lewy bodies" and "Management of nonmotor symptoms in Parkinson disease".) Benzodiazepines — <span>Benzodiazepines have a limited role in the treatment of delirium; they are primarily indicated in cases of sedative drug and alcohol withdrawal or when antipsychotic drugs are contraindicated. Surveys of practicing clinicians suggest that benzodiazepines are overprescribed for patients with delirium [79]. (See "Sedative-analgesic medications in critically ill adults: Selection, initiation, maintenance, and withdrawal".) Benzodiazepines (eg, lorazepam 0.5 to 1 mg) have a more rapid onset
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
est that benzodiazepines are overprescribed for patients with delirium [79]. (See "Sedative-analgesic medications in critically ill adults: Selection, initiation, maintenance, and withdrawal".) <span>Benzodiazepines (eg, lorazepam 0.5 to 1 mg) have a more rapid onset of action (five minutes after parenteral administration) than the antipsychotics, but they can worsen confusion and sedation [70]. In a prospective study of ICU patients, lorazepam was an independent risk factor for incident delirium, increasing the risk by approximately 20 percent [80]. A systematic review of benzodiazepine use in delirium found two studies comparing benzodiazepine versus antipsychotic agents; one study found no advantage, the other found decreased effectiveness of benzodiazepines compared with antipsychotics [81]. In two randomized trials of sedative treatment in mechanically ventilated ICU patients, the benzodiazepine midazolam was associated with significantly more delirium compared with dexmedetomidine treatment (77 versus 54 percent) [82], while similar outcomes were observed with lorazepam and dexmedetomidine [83]. Cholinesterase inhibitors — Cholinesterase inhibitors do not have a role in the treatment or symptom management of delirium. A randomized clinical trial compared rivastigmine with place
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ntly more delirium compared with dexmedetomidine treatment (77 versus 54 percent) [82], while similar outcomes were observed with lorazepam and dexmedetomidine [83]. Cholinesterase inhibitors — <span>Cholinesterase inhibitors do not have a role in the treatment or symptom management of delirium. A randomized clinical trial compared rivastigmine with placebo in 104 hospitalized intensive care patients with delirium who were also prescribed haloperidol. The trial was stopped early because of higher mortality in the rivastigmine group (22 versus 8 percent) [84]. Median duration of delirium was also longer in the rivastigmine group (5 versus 3 days, p = 0.06). Cholinesterase inhibitors are also not helpful in the prevention of delirium. (See 'Prevention' above.) Other sedative agents — Other sedative agents (eg, dexmedetomidine, propofol, as well as benzodiazepines and antipsychotics) are often used in the critical care setting to manage anxiet
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
lphenidate or modafinil cannot be recommended for treating hypoactive delirium because of the potential risk of precipitating agitation or worsening psychotic symptoms [90]. Terminal delirium — <span>Delirium is common in palliative care settings and causes significant distress to family members [91]. Underlying causes are often multifactorial, but up to 50 percent of episodes are reversible, particularly when the underlying cause is either dehydration or medication related [92,93]. Hyperactive as well as hypoactive presentations of terminal delirium are both common; the former may require management with antipsychotic medication, usually haloperidol, as described
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
liative care in hospice or hospital settings found patients in the placebo arm had fewer distressing delirium symptoms and better overall survival [97]. (See 'Antipsychotic medications' above.) <span>In one small case series, methadone appeared to be effective in the treatment of both refractory pain and terminal delirium when antipsychotic medication was not [17]. Midazolam sedation has also been described as a therapeutic option in this setting [98,99]. (See "Overview of managing common non-pain symptoms in palliative care", section on 'Palliative sedation'.) Ethical considerations — The treatment of patients with delirium is complicat
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
on 'Palliative sedation'.) Ethical considerations — The treatment of patients with delirium is complicated by the critical nature of their illness and their impaired capacity to make decisions. <span>The doctrine of "implied consent" allows the emergency treatment of patients with delirium in order to stabilize a life-threatening process [100]. However, it is important to document the assessment of cognitive abilities and decision-making capacity. Current practice leaves considerable room for improvement. As an example, in a prospective study of 173 medical and surgical procedures performed in patients with delirium at a univers
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
percent. Relying upon implied consent or substituted judgment in cases of delirium introduces other difficulties since clinicians and proxies do not always make the same decisions as patients. <span>Every effort should be made to determine what the patient's own treatment preferences are, and to not assume that decision-making capacity is "all or none." In some cases, for example, psychopharmacologic treatment of delirium may restore sufficient mental capacity to allow a discussion of treatment preferences [102]. In addition, since delirium typically fluctuates in severity, there may also be periods of lucidity in which a discussion of treatment preferences may take place. OUTCOMES — Delirium has an enormous impact upon the health of older persons. Patients with delirium experience prolonged hospitalizations, functional and cognitive decline, higher morta
Flashcard 7055872757004
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
sed one-year mortality compared with those whose symptoms had resolved more quickly, regardless of whether or not patients also had underlying dementia [115]. Persistent cognitive dysfunction — <span>Signs of delirium may persist for 12 months or longer, particularly in those with underlying dementia [118]. One long-term follow-up study found that after two years, only one-third of patients who had experienced delirium still lived independently in the community [119]. Another prospective s
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
onpharmacologic interventions' above.) ●Frequent reassurance, touch, and verbal orientation from familiar persons can lessen disruptive behaviors. (See 'Nonpharmacologic interventions' above.) ●<span>A cautious trial of psychotropic medication should be reserved for as-needed treatment of severe agitation or psychosis with the potential for harm. In this setting, we suggest using low-dose haloperidol (0.5 to 1 mg orally [PO] or intramuscularly [IM]) (Grade 2C). Other antipsychotic agents (quetiapine, risperidone, ziprasidone, olanzapine) are reasonable alternatives. (See 'Antipsychotic medications' above.) •Haloperidol is associated with a low frequency of sedation and hypotension. •Haloperidol should be avoided in patients with underlying parkinsonism, for whom atypical antipsychotics (eg, quetiapine) are preferred. •Short-term use of antipsychotic agents is advised. •Clinicians should recognize when the caregiver's distress, rather than reduction of the severity or duration of delirium, is often a motivating factor in the decision to prescribe psychotropic medication. ●Benzodiazepines should be avoided in patients with or at risk for delirium, except in cases of sedative drug and alcohol withdrawal or when antipsychotic medications are contraindicated. (See 'Benzodiazepines' above.) ●Cholinesterase inhibitors are not effective in preventing or treating the symptoms of delirium, and often create undesirable side effects. (See 'Cholinesterase inhibitors' above.) ●Del
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
INFECTION — Fundamental alterations in quantitative and qualitative immune responses occur with aging, a process that has been called immune senescence. (See "Immune function in older adults".) <span>Age-related physiologic changes include: ●Increased risk of invasion by pathogenic organisms due to alterations in the barriers posed by the skin, lungs, and gastrointestinal tract (and other mucosal linings) [2]. ●Increased risk of intracellular pathogens due to changes in cellular and humoral immunity, including decreases in specific cell populations, loss of the proliferative capacity of immune cells, and decreased production of specific cytokines (eg, interleukin 2) [3,4]. ●Impaired defense against fungal and viral pathogens due to impaired signal transduction after cytokine binding. ●Decreased antibody response to vaccines, related to reductions in toll-like receptors [5], senescence of CD8 cells [6], reductions in naïve CD4 cells [7], and changes in B-cell biology [8]. ●Impaired immunoglobulin production and specificity of antibody responses associated with reductions in naïve B cells [9,10]. Older adults with chronic diseases (eg, diabetes, chronic obstructive pulmonary disease, or heart failure) have greater impairment in immunity, resulting in greater susceptibility to co
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ductions in naïve CD4 cells [7], and changes in B-cell biology [8]. ●Impaired immunoglobulin production and specificity of antibody responses associated with reductions in naïve B cells [9,10]. <span>Older adults with chronic diseases (eg, diabetes, chronic obstructive pulmonary disease, or heart failure) have greater impairment in immunity, resulting in greater susceptibility to common infections and poorer vaccine responses [3]. The risk of infection in older patients is often heightened by communal residence or other social institutions such as nursing homes, daycare programs, or senior centers [11-17]. PRESEN
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
iabetes, chronic obstructive pulmonary disease, or heart failure) have greater impairment in immunity, resulting in greater susceptibility to common infections and poorer vaccine responses [3]. <span>The risk of infection in older patients is often heightened by communal residence or other social institutions such as nursing homes, daycare programs, or senior centers [11-17]. PRESENTATION OF DISEASE — It has long been recognized that older adults can have severe infection that does not manifest with the typical signs or symptoms characterizing disease in you
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
been recognized that older adults can have severe infection that does not manifest with the typical signs or symptoms characterizing disease in younger adults [18,19]. Suspicion for infection — <span>Older adults with infection may lack fever or localizing, infection-specific symptoms or signs. As an example, rather than a fever, productive cough, and pleuritic chest pain, pneumonia in an older adult may present as a low-grade temperature elevation to 99ºF and an increased oxygen requirement. Infection in older patients may be associated with nonspecific symptoms such as increased confusion, falling, and anorexia [20]. However, these nonspecific symptoms are common in older
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ample, rather than a fever, productive cough, and pleuritic chest pain, pneumonia in an older adult may present as a low-grade temperature elevation to 99ºF and an increased oxygen requirement. <span>Infection in older patients may be associated with nonspecific symptoms such as increased confusion, falling, and anorexia [20]. However, these nonspecific symptoms are common in older adults and do not have high positive predictive value for infection [21]; they do not necessitate empiric treatment but should prompt attempts to elicit localizing signs on physical examination, medication review, and other diagnostic tests or supportive measures such as oral hydration. The presence of new fever, hypothermia, delirium, or new-onset hyperglycemia should prompt an evaluation of infection. However, behavioral changes in by themselves do not require an exh
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ate empiric treatment but should prompt attempts to elicit localizing signs on physical examination, medication review, and other diagnostic tests or supportive measures such as oral hydration. <span>The presence of new fever, hypothermia, delirium, or new-onset hyperglycemia should prompt an evaluation of infection. However, behavioral changes in by themselves do not require an exhaustive evaluation for infection. If empiric treatment is initiated, it is important to discontinue it promptly if diagnostic tests are negative [22-24]. Older adults with cognitive impairment tend to have behavioral changes due to a variety of reasons including waxing and waning of underlying cognitive impairment. In these situations, c
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
heir primary care provider is important. Cognitive impairment further contributes to the atypical presentation of infections in older adults due to the reduced capacity to communicate symptoms. <span>Clinicians may need to pursue objective assessments such as laboratory and radiologic evaluations at a lower threshold in cognitively impaired patients, unless advanced directives and goals of care dictate otherwise. However, in situations of only new-onset behavioral symptoms without any other localizing symptoms and in absence of delirium, further evaluation for infection may not be useful. In these cases, noninfectious etiologies should be carefully considered [20]. Given the often atypical and subtle ways in which infection presents in older adults, there has been substantial interest in biomarkers such as C-reactive protein and procalcitonin to h
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ns including waxing and waning of underlying cognitive impairment. In these situations, careful clinical evaluation (including presence of delirium) by their primary care provider is important. <span>Cognitive impairment further contributes to the atypical presentation of infections in older adults due to the reduced capacity to communicate symptoms. Clinicians may need to pursue objective assessments such as laboratory and radiologic evaluations at a lower threshold in cognitively impaired patients, unless advanced directives and g
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
thout any other localizing symptoms and in absence of delirium, further evaluation for infection may not be useful. In these cases, noninfectious etiologies should be carefully considered [20]. <span>Given the often atypical and subtle ways in which infection presents in older adults, there has been substantial interest in biomarkers such as C-reactive protein and procalcitonin to help identify infection. Unfortunately, varying cutoffs for "normal" values have led to wide variation in sensitivity and specificity for these assays [25,26]. The use of procalcitonin in evaluation of infection and antibiotic use is discussed in detail elsewhere. (See "Sepsis syndromes in adults: Epidemiology, definitions, clinical presentation, diagnosis, and prognosis", section on 'Laboratory signs' and "Evaluation and management of suspected sepsis and septic shock in adults", section on 'De-escalation and duration of antibiotics' and "Procalcitonin use in lower respiratory tract infections".) Fever definition — Relatively healthy, community-dwelling older adults may be appropriately managed using conventional definitions of fever. In these patients, a temperature >38°C (1
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
gement of suspected sepsis and septic shock in adults", section on 'De-escalation and duration of antibiotics' and "Procalcitonin use in lower respiratory tract infections".) Fever definition — <span>Relatively healthy, community-dwelling older adults may be appropriately managed using conventional definitions of fever. In these patients, a temperature >38°C (100.4ºF) indicates a potential for serious infection, while hypothermia relative to baseline body temperature may signify severe infection or even sepsis [27]. However, in frail, older adults, fever is absent in 30 to 50 percent, even in the setting of serious infections such as pneumonia or endocarditis [28,29]. Thus, we use a lower threshold
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
patients, a temperature >38°C (100.4ºF) indicates a potential for serious infection, while hypothermia relative to baseline body temperature may signify severe infection or even sepsis [27]. <span>However, in frail, older adults, fever is absent in 30 to 50 percent, even in the setting of serious infections such as pneumonia or endocarditis [28,29]. Thus, we use a lower threshold for fever in frail, older patients: ●Single oral temperature >37.8°C (>100ºF) ●Persistent oral or tympanic membrane temperature ≥37.2°C (99.0ºF) ●Rise in temperature of ≥1.1°C (≥2°F) above baseline temperature The blunted febrile response in older adults is due to impairment in multiple systems responsible for thermoregulation (eg, shivering, vasoconstriction, hypothalamic regulation, and the
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
der patients: ●Single oral temperature >37.8°C (>100ºF) ●Persistent oral or tympanic membrane temperature ≥37.2°C (99.0ºF) ●Rise in temperature of ≥1.1°C (≥2°F) above baseline temperature <span>The blunted febrile response in older adults is due to impairment in multiple systems responsible for thermoregulation (eg, shivering, vasoconstriction, hypothalamic regulation, and thermogenesis by brown adipose tissue) [30]. Revisions of parameters used to identify "fever" in frail older adults have thus been suggested [27,31,32]. Infections can also present with hypothermia. Following criteria are recommended to define hypothermia: ●Two or more temperature measurements ≤95.9°F (≤36.0°C) [33]; or ●Two or more tem
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ogenesis by brown adipose tissue) [30]. Revisions of parameters used to identify "fever" in frail older adults have thus been suggested [27,31,32]. Infections can also present with hypothermia. <span>Following criteria are recommended to define hypothermia: ●Two or more temperature measurements ≤95.9°F (≤36.0°C) [33]; or ●Two or more temperature measurements documenting a decrease in temperature of >2°F (>1.1°C) from the baseline [20] ANTIBIOTIC MANAGEMENT — Antibiotic management in older patients is influenced by age-related pharmacokinetic changes, comorbidities, and risk of exposure to, or infection with, multidru
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
erature measurements ≤95.9°F (≤36.0°C) [33]; or ●Two or more temperature measurements documenting a decrease in temperature of >2°F (>1.1°C) from the baseline [20] ANTIBIOTIC MANAGEMENT — <span>Antibiotic management in older patients is influenced by age-related pharmacokinetic changes, comorbidities, and risk of exposure to, or infection with, multidrug resistant organisms. Absorption of oral or enteric drugs is often diminished due to increase in gastric pH and gastric emptying, atrophy of mucosal surfaces, and reduced gastric motility. Systemic distribution of antibiotics may be influenced by factors such as drug solubility, serum proteins, and cardiac output. Since most antibiotics are eliminated by hepatic and renal metabolism, rates of elimination are usually impacted. In addition, patient adherence may be decreased due to poor cognitive function, impaired hearing or vision, polypharmacy, and medication side effects. In general, antibiotic use is very common in older adults and a significant proportion are inappropriately prescribed due to lack of appropriate indication, overly broad spectrum, or a longer duration than necessary. Choice of agent — The choice of initial antibiotic is generally the same as in younger patients for most routine infections. Choice of agent should be guided by the knowledge of local a
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
infections. Choice of agent should be guided by the knowledge of local antimicrobial susceptibility and resistance patterns through facility antibiograms or public health information networks. <span>Watchful waiting with close monitoring and hydration may be appropriate in milder cases of infection while conducting diagnostic workup, particularly in milder cases of urinary tract infection (UTI) without concerning physical findings. However, consideration for broader empiric coverage may be warranted in some situations: ●Increased risk of infection with drug-resistant organisms, due to residence in an institution, recent hospitalization, dialysis treatment, recent antibiotic exposure, or indwelling devices [13,14]. ●Broader initial coverage may be appropriate in seriously ill older adults in whom sepsis, severe pneumonia, or other life-threatening infections are more likely to be suspected [34]. However, it is very important to narrow the antibiotic regimen when cultures are available to decrease the risk of engendering antibiotic resistance and of Clostridioides difficile dise
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
[13,14]. ●Broader initial coverage may be appropriate in seriously ill older adults in whom sepsis, severe pneumonia, or other life-threatening infections are more likely to be suspected [34]. <span>However, it is very important to narrow the antibiotic regimen when cultures are available to decrease the risk of engendering antibiotic resistance and of Clostridioides difficile disease. Antibiotic interactions are also a major consideration in antibiotic selection, as these may occur with many medications commonly prescribed in older adults, particularly those with a n
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
4]. However, it is very important to narrow the antibiotic regimen when cultures are available to decrease the risk of engendering antibiotic resistance and of Clostridioides difficile disease. <span>Antibiotic interactions are also a major consideration in antibiotic selection, as these may occur with many medications commonly prescribed in older adults, particularly those with a narrow therapeutic index. For example, significant interactions with commonly prescribed antibiotics are seen for warfarin, antacids and H2 receptor antagonists, and digoxin. For some antibiotics, the direction of the interaction may be hard to predict and may even be biphasic (eg, rifampin increases concentrations of some drugs initially, but induction of hepatic enzymes may lead to reduced drug concentrations in a few days). Dosing — The distribution, metabolism, and excretion of many drugs is altered with age [35], most importantly due to a decrease in glomerular filtration rate (GFR). (See "Drug prescribi
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
auses of infection among institutionalized older patients than those who are community-dwelling [11,12,37]. Additionally, patients with indwelling devices are at particularly high risk [13,14]. <span>Antibiotic resistance is fostered in the nursing home setting by debilitated hosts, close proximity of residents, and persistent antibiotic pressure. Over 50 percent of older adults in nursing homes carry a drug-resistant organism [38]. Major strategies to enhance antimicrobial stewardship in nursing homes include: avoiding treatment of asymptomatic bacteriuria, specifically addressing avoidance of antibiotics in end-o
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
rsing home setting by debilitated hosts, close proximity of residents, and persistent antibiotic pressure. Over 50 percent of older adults in nursing homes carry a drug-resistant organism [38]. <span>Major strategies to enhance antimicrobial stewardship in nursing homes include: avoiding treatment of asymptomatic bacteriuria, specifically addressing avoidance of antibiotics in end-of-life discussions, and focusing on the shortest effective duration of therapy for specific syndromes [16,39-41]. The Centers for Disease Control and Prevention (CDC) has described 10 core elements of antimicrobial stewardship which include leadership support, accountability, drug expertise, a plan o
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
adults. This review will not attempt to review all infections affecting older adults. Multiple topics in UpToDate address issues related to these and other infections. Urinary tract infection — <span>Urinary tract infection (UTI) is the most common infectious illness in adults age 65 and over, and in general it is diagnosed and managed in the same way as in the general population [42,43]. However, establishing the diagnosis in older patients is complicated due to the higher prevalence of chronic urinary symptoms and cognitive impairment, which make it difficult to identify specific UTI symptoms. This diagnostic challenge, in addition to the high prevalence of asymptomatic bacteriuria in this population, often leads to overdiagnosis and unnecessary treatment [44]. Therefore, it is important to have a high threshold for urine testing to avoid this pitfall. We recommend urine testing only in the presence of classic signs and symptoms of UTI (acute dysuria, new or worsening urgency or frequency, new incontinence, gross hematuria, and suprap
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
tomatic bacteriuria in this population, often leads to overdiagnosis and unnecessary treatment [44]. Therefore, it is important to have a high threshold for urine testing to avoid this pitfall. <span>We recommend urine testing only in the presence of classic signs and symptoms of UTI (acute dysuria, new or worsening urgency or frequency, new incontinence, gross hematuria, and suprapubic or costovertebral angle tenderness) or physiologic signs of serious acute illness (eg, fever, other major vital sign abnormalities, changes in level of consciousness). Signs of systemic infection, particularly in the absence of urinary symptoms, should prompt evaluation for other sources of infection. Restricting urine testing for these clinical features is particularly challenging in certain populations: ●Patients with chronic lower urinary tract symptoms – It can sometimes be diffi
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
absence of urinary symptoms, should prompt evaluation for other sources of infection. Restricting urine testing for these clinical features is particularly challenging in certain populations: ●<span>Patients with chronic lower urinary tract symptoms – It can sometimes be difficult to tease out new symptoms in patients who have chronic incontinence, frequency, or urgency. It is important for the clinician to have a good understanding of the patient’s usual symptoms in order to detect any meaningful and persistent changes. For example, in a woman with chronic incontinence, new onset of dysuria or gross hematuria would be an appropriate trigger for urine testing. ●Patients with nonspecific symptoms (such as mental status changes) – Many clinicians consider nonspecific symptoms such as functional decline and behavioral or mental status changes as
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
woman with chronic incontinence, new onset of dysuria or gross hematuria would be an appropriate trigger for urine testing. ●Patients with nonspecific symptoms (such as mental status changes) – <span>Many clinicians consider nonspecific symptoms such as functional decline and behavioral or mental status changes as indicative of a UTI in older patients [45]. Too often, "checking a urinalysis and culture" is a reflex that does not take into account the consequence of potentially unnecessary antibiotics. Although older adults may present with atypical signs and symptoms, most older adults with an infection will also present with some localizing signs and symptoms [20]. We do not check urine testing based on such nonspecific symptoms in the absence of findings concerning for systemic infection as above. Growing evidence indicates that these nonspecific features are not reliable predictors of bacteriuria or UTI [46-49], and there is no evidence that treating bacteriuria in patients with delirium, falls, or confusion improves outcomes [50,51]. Furthermore, patients with dementia have normal fluctuations in behavior, and because of the frequency of asymptomatic bacteriuria in this population, urine testing will often yield a p
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
features are not reliable predictors of bacteriuria or UTI [46-49], and there is no evidence that treating bacteriuria in patients with delirium, falls, or confusion improves outcomes [50,51]. <span>Furthermore, patients with dementia have normal fluctuations in behavior, and because of the frequency of asymptomatic bacteriuria in this population, urine testing will often yield a positive culture; this can erroneously link such normal fluctuations with bacteriuria, resulting in repeated unnecessary antibiotic treatment and subsequent development of resistant organisms. Urinary tract symptoms are difficult to elicit in patients with cognitive impairment; in such cases, clinical suspicion for UTI often rests on the emergence of new symptoms as noted by clinicians who know the patient well. Other criteria have been proposed to clarify the symptoms that warrant testing and potential treatment for a presumptive UTI in residents of long-term care facilities (table 1) [52]. Cl
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
fficult to elicit in patients with cognitive impairment; in such cases, clinical suspicion for UTI often rests on the emergence of new symptoms as noted by clinicians who know the patient well. <span>Other criteria have been proposed to clarify the symptoms that warrant testing and potential treatment for a presumptive UTI in residents of long-term care facilities (table 1) [52]. Clinical algorithms using such criteria have been shown to decrease antibiotic prescriptions for suspected UTI in nursing home settings [53]. Being judicious about urine testing is important in these populations because neither positive urinalyses nor culture results necessarily indicate a true infection. Urinalysis results h
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
idents of long-term care facilities (table 1) [52]. Clinical algorithms using such criteria have been shown to decrease antibiotic prescriptions for suspected UTI in nursing home settings [53]. <span>Being judicious about urine testing is important in these populations because neither positive urinalyses nor culture results necessarily indicate a true infection. Urinalysis results have low specificity for UTI. Although they can be used to rule out UTI in those with a low pre-test probability, the presence of positive leukocyte esterase or nitrite on dipstick does not rule in a UTI. (See "Sampling and evaluation of voided urine in the diagnosis of urinary tract infection in adults", section on 'Accuracy'.) Furthermore, the presence of bacteria on culture does not e
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
e leukocyte esterase or nitrite on dipstick does not rule in a UTI. (See "Sampling and evaluation of voided urine in the diagnosis of urinary tract infection in adults", section on 'Accuracy'.) <span>Furthermore, the presence of bacteria on culture does not equate to a UTI. The urinary tract is increasingly recognized as a non-sterile environment with a generally beneficial microbiome, which may provide protection against infection, and for which treatment with antibiotics may be harmful [54,55]. Asymptomatic bacteriuria occurs in up to 6 to 16 percent of older women in the community and 25 to 54 percent of women in nursing homes, with a frequency in men about half those figures [56]. With the use of chronic catheters, rates are even higher (about 85 percent for condom catheters and nearly 100 percent for indwelling catheters). Diagnosis of UTI is discussed in detail elsewhere. (See "Acute simple cystitis in women", section on 'Diagnosis' and "Acute complicated urinary tract infection (including pyelonephritis
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
in detail elsewhere. (See "Acute simple cystitis in women", section on 'Diagnosis' and "Acute complicated urinary tract infection (including pyelonephritis) in adults", section on 'Diagnosis'.) <span>When the diagnosis of UTI is in doubt (eg, pyuria and bacteriuria in the setting of ambivalent symptoms), a reasonable management strategy in patients who do not appear seriously ill is to defer antibiotic treatment for one week with follow-up [43], since 25 to 50 percent of older women with UTI symptoms will improve without therapy in this time frame [57]. Although a large retrospective database analysis of patients ≥65 years of age with lower UTI suggested an association between delaying antimicrobial therapy and subsequent bloodstream infection within 60 days, multiple limitations of this study reduce confidence in the findings [58]. Furthermore, in a subsequent analysis of the same dataset by different researchers, delayed antibiotic therapy was not associated with subsequent bloodstream infections [59]. However, this analyses did find evidence of some increase in mortality in the delayed therapy group. These discordant findings could be explained by residual confounding and suggest that more research is warranted to further guide practice. We recommend against antibiotic "trials" as these may cause drug toxicity, drug-drug interactions, and antimicrobial resistance. Numerous studies suggest that there is no clinical benef
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
e increase in mortality in the delayed therapy group. These discordant findings could be explained by residual confounding and suggest that more research is warranted to further guide practice. <span>We recommend against antibiotic "trials" as these may cause drug toxicity, drug-drug interactions, and antimicrobial resistance. Numerous studies suggest that there is no clinical benefit to treatment of asymptomatic bacteriuria and that such treatment can lead to significant side effects, expense, and potential for selection of resistant organisms. (See "Asymptomatic bacteriuria in adults".) For patients diagnosed with UTI, the management is the same as in the general population and depends on whether the infection is thought to be primarily in the bladder (ie, simple cysti
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
f asymptomatic bacteriuria and that such treatment can lead to significant side effects, expense, and potential for selection of resistant organisms. (See "Asymptomatic bacteriuria in adults".) <span>For patients diagnosed with UTI, the management is the same as in the general population and depends on whether the infection is thought to be primarily in the bladder (ie, simple cystitis) or whether the UTI is complicated by upper tract (pyelonephritis), prostatic, or systemic involvement. Escherichia coli, Klebsiella pneumoniae, and Enterococcus faecalis are implicated in the majority of UTIs in older adults [60]. The approach to management of cystitis and complicated UTI is discussed in detail elsewhere. (See "Acute simple cystitis in women" and "Acute simple cystitis in men" and "Acute complicated urinary tract infection (including pyelonephritis) in adults".) The management of cathete
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
of prognostic formulas to assess severity and determine indications for hospitalization. However, these formulas are intended to supplement rather than override the judgment of the clinicians. <span>For older adults, other issues that are important to the decision to hospitalize include social support, ability to take oral medicines, living conditions, underlying psychiatric issues, cognitive impairment, or functional impairment. The microbiology of pneumonia in older adults differs from that of young adults. Streptococcus pneumoniae is still the predominant organism, but polymicrobial infection and Gram-negativ
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
mportant to the decision to hospitalize include social support, ability to take oral medicines, living conditions, underlying psychiatric issues, cognitive impairment, or functional impairment. <span>The microbiology of pneumonia in older adults differs from that of young adults. Streptococcus pneumoniae is still the predominant organism, but polymicrobial infection and Gram-negative organisms (Haemophilus influenzae, Legionella pneumophila, Moraxella catarrhalis, Klebsiella spp) occur more commonly, particularly in patients with chronic obstructive pulmonary disease or among those who reside in long-term care facilities [65,66]. Antibiotic treatment for pneumonia in older adults follows standard guidelines. However, the risk of methicillin-resistant S. aureus (MRSA) and Gram-negative organisms should be taken i
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
, Moraxella catarrhalis, Klebsiella spp) occur more commonly, particularly in patients with chronic obstructive pulmonary disease or among those who reside in long-term care facilities [65,66]. <span>Antibiotic treatment for pneumonia in older adults follows standard guidelines. However, the risk of methicillin-resistant S. aureus (MRSA) and Gram-negative organisms should be taken into account for patients who reside in nursing homes. (See "Treatment of community-acquired pneumonia in adults in the outpatient setting" and "Treatment of community-acquired pneumonia in adults who require hospitalization" and "Treatment
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
he outpatient setting" and "Treatment of community-acquired pneumonia in adults who require hospitalization" and "Treatment of hospital-acquired and ventilator-associated pneumonia in adults".) <span>Immunization for influenza and pneumococcus are the most important pneumonia preventive strategies. While pneumococcal vaccination may not prevent pneumonia in older adults, rates of bacteremia and invasive pneumococcal disease are decreased in immunized patients, and mortality in older patients hospitalized with pneumonia is lower among those who were vaccinated prior to admission [67,68]. (See "Pneumococcal vaccination in adults" and "Seasonal influenza vaccination in adults".) Older adults are at higher risk for aspiration pneumonia. A number of interventions (eg, posit
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ients hospitalized with pneumonia is lower among those who were vaccinated prior to admission [67,68]. (See "Pneumococcal vaccination in adults" and "Seasonal influenza vaccination in adults".) <span>Older adults are at higher risk for aspiration pneumonia. A number of interventions (eg, positioning, dietary changes, drugs, oral hygiene, oral rinse solutions, tube feeding) have been proposed to prevent aspiration with limited data to document effectiveness [69-75]. Discontinuation of proton pump inhibitors is also a preventive strategy [76]. Other techniques for the prevention and treatment of aspiration in hospitalized patients are discussed separately. (See "Aspiration pneumonia in adults".) Influenza epidemics dispropor
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ics disproportionately affect older adults, with higher rates of morbidity and mortality [77-80], the treatment of which is discussed elsewhere. (See "Seasonal influenza in adults: Treatment".) <span>Reactivation tuberculosis is also more common in older adults since they are more likely to have been exposed to Mycobacterium tuberculosis in the first half of the 20th century. Treatment is discussed elsewhere. (See "Treatment of latent tuberculosis infection in HIV-uninfected nonpregnant adults".) Bacteremia — When compared with young adults, the presentation
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
erium tuberculosis in the first half of the 20th century. Treatment is discussed elsewhere. (See "Treatment of latent tuberculosis infection in HIV-uninfected nonpregnant adults".) Bacteremia — <span>When compared with young adults, the presentation of bacteremia may be more subtle in older patients, with a lower likelihood of chills, sweating or fever. Thus, it may be appropriate to order blood cultures without these signs and symptoms but when sepsis is suspected, such as in the setting of tachycardia or hypotension [25]. Gastrointestinal and genitourinary sources of bacteremia are more common in older adults, as is isolation of Gram-negative rods, a trend that continues to increase throughout the eighth
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
sweating or fever. Thus, it may be appropriate to order blood cultures without these signs and symptoms but when sepsis is suspected, such as in the setting of tachycardia or hypotension [25]. <span>Gastrointestinal and genitourinary sources of bacteremia are more common in older adults, as is isolation of Gram-negative rods, a trend that continues to increase throughout the eighth and ninth decades of life [81]. Bacteremia carries a poorer prognosis with advanced age. For example, nosocomial Gram-negative bacteremia has a mortality rate of 5 to 35 percent in young adults and 37 to 50 percent in
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
itourinary sources of bacteremia are more common in older adults, as is isolation of Gram-negative rods, a trend that continues to increase throughout the eighth and ninth decades of life [81]. <span>Bacteremia carries a poorer prognosis with advanced age. For example, nosocomial Gram-negative bacteremia has a mortality rate of 5 to 35 percent in young adults and 37 to 50 percent in older adults [82]. Nosocomial bacteremia in older adults is highly associated with the presence of invasive devices such as intravenous or urinary catheters and is most commonly due to MRSA [83]. The treatment of bacteremia is discussed in detail elsewhere. (See "Gram-negative bacillary bacteremia in adults" and "Clinical approach to Staphylococcus aureus bacteremia in adults".)
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
acteremia is discussed in detail elsewhere. (See "Gram-negative bacillary bacteremia in adults" and "Clinical approach to Staphylococcus aureus bacteremia in adults".) Fever of unknown origin — <span>Fever of unknown origin (FUO) is defined as temperature >38.3°C (101°F) for at least three weeks and undiagnosed after one week of medical evaluation. The causes of FUO in older patients differ somewhat from those in younger adults. In particular, giant cell (temporal) arteritis and polymyalgia rheumatica are important considerations
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
likely to have been exposed to M. tuberculosis, which was more prevalent in the first half of the 20th century. (See "Etiologies of fever of unknown origin in adults", section on 'Infections'.) <span>Although the prevalence of malignancies increase with age, malignant disease as a cause of FUO occurs with similar frequency in old and young adults [85,86]. In both age groups, non-Hodgkin lymphoma accounts for the majority of such cases. (See "Etiologies of fever of unknown origin in adults", section on 'Malignancy'.) Infective endocarditis — Infective endocarditis (IE) is often related to degenerative valvular disease,
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
in adults".) Fever of unknown origin — Fever of unknown origin (FUO) is defined as temperature >38.3°C (101°F) for at least three weeks and undiagnosed after one week of medical evaluation. <span>The causes of FUO in older patients differ somewhat from those in younger adults. In particular, giant cell (temporal) arteritis and polymyalgia rheumatica are important considerations in older patients, and patients age >60 years with FUO should have a rheumatological evaluation including early temporal artery biopsy, particularly if the erythrocyte sedimentation rate or liver enzymes are elevated [84]. (See "Diagnosis of giant cell arteritis".) In the absence of specific risk factors, older adults in resource-rich settings are more likely to have been exposed to M. tuberculosis, which was more prevalent in the first half of the 20th century. (See "Etiologies of fever of unknown origin in adults", section on 'Infections'.) Although the prevalence of malignancies increase with age, malignant disease as a cause of FUO occurs w
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
in adults", section on 'Malignancy'.) Infective endocarditis — Infective endocarditis (IE) is often related to degenerative valvular disease, mitral valve prolapse, or a prosthetic valve [87]. <span>Older adults have a fivefold higher risk of IE than the general population [88]. A low threshold for suspecting IE and for pursuing transesophageal echocardiography (TEE) if transthoracic echocardiography (TTE) is negative is warranted. The diagnosis of IE may be more difficult in older patients and is often delayed due to atypical clinical presentations and difficulty in interpreting echocardiographic findings. Certai
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
is warranted. The diagnosis of IE may be more difficult in older patients and is often delayed due to atypical clinical presentations and difficulty in interpreting echocardiographic findings. <span>Certain classic signs and symptoms of IE such as fever, leukocytosis, embolic events, splenomegaly, skin lesions (Osler nodes, Janeway lesions), and conjunctival hemorrhages are less common with advanced age [89]. Several features of IE in older adults complicate the use of echocardiography. The higher prevalence of calcified valvular lesions and prosthetic valves makes echocardiographic findings
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
skin lesions (Osler nodes, Janeway lesions), and conjunctival hemorrhages are less common with advanced age [89]. Several features of IE in older adults complicate the use of echocardiography. <span>The higher prevalence of calcified valvular lesions and prosthetic valves makes echocardiographic findings more difficult to interpret in older adults, particularly when using TTE [90]. In addition, older adults tend to have smaller and fewer vegetations than younger adults and a higher rate of intracardiac abscess and prosthetic perivalvular complications [89]. For these reasons, it is recommended that a lower threshold for obtaining TEE be employed in older adult patients suspected of having IE. However, it is important to be aware of the pot
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
impairment, polypharmacy, or multiple comorbidities. (See "Clinical manifestations and evaluation of adults with suspected left-sided native valve endocarditis", section on 'Echocardiography'.) <span>Streptococci and staphylococci are recovered from approximately 80 percent of older adults with IE [87], although enterococcal and Gram-negative organisms occur more commonly than in younger patients, likely due to a greater incidence of gastrointestinal and genitourinary sources of bacteremia. Antimicrobial treatment of infective endocarditis is discussed elsewhere. (See "Antimicrobial therapy of left-sided native valve endocarditis" and "Antimicrobial therapy of prosthetic v
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
nfective endocarditis is discussed elsewhere. (See "Antimicrobial therapy of left-sided native valve endocarditis" and "Antimicrobial therapy of prosthetic valve endocarditis".) HIV infection — <span>Because HIV has primarily afflicted younger adults (in their 20s and 30s), most of the HIV literature defines “older adults” as those age 50 years or over. The success of antiretroviral therapy (ART) has resulted in the long-term survival of many patients with HIV, increasing the number of older adults with this chronic infection. In gener
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
eractions with antiretroviral agents, and age-related comorbid conditions. These are discussed in greater detail elsewhere. (See "HIV infection in older adults".) Prosthetic device infections — <span>The prevalence of implanted prosthetic devices (eg, prosthetic joints, cardiac pacemakers, artificial heart valves, vascular grafts) increases with advancing age. A two-stage procedure with device removal, prolonged antibiotic administration, and subsequent reimplantation of the device is usually considered the gold standard of therapy. However, in older adults, the goals of treatment and the importance of maximizing functional status may affect treatment choice. For example, long periods of debility and being bed-bound are more likely to result in loss of functional status and independence in older adults, and these outcomes are rarely consider
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
VID-19, including the impact of older age, are discussed elsewhere. (See "COVID-19: Clinical features" and "COVID-19: Diagnosis" and "COVID-19: Clinical features", section on 'Increasing age'.) <span>COVID-19 is a respiratory tract illness that commonly causes fever, cough, fatigue, anorexia, shortness of breath, myalgias, sore throat, headache, chills, and new loss of taste or smell [92,93]. Early reports suggest that shortness of breath is perhaps more frequent among older adults (12 percent for patients >60 years versus 3 percent for patients <60 years) [94]. Much like other infections, the fever response may be blunted, and the classic symptoms of dyspnea and cough may not be robust. Similar to other infections, older adults with COVID-19 may present with subtle or nonspecific findings [95] Asymptomatic infection is also common [96]. In the appropriate clinical settings (community spread or proximity to known cases), clinicians should have a low threshold for considering COVID-19 in older adults with nonspecific sym
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
of dyspnea and cough may not be robust. Similar to other infections, older adults with COVID-19 may present with subtle or nonspecific findings [95] Asymptomatic infection is also common [96]. <span>In the appropriate clinical settings (community spread or proximity to known cases), clinicians should have a low threshold for considering COVID-19 in older adults with nonspecific symptoms such as falls, confusion or worsening functional impairment [97]. It is important to recognize the full spectrum of these findings in older adults in order to prevent COVID-19 transmission from asymptomatic or presymptomatic individuals. A large numbe
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
atients in isolation at the end of life. These are discussed separately. (See "Palliative care: The last hours and days of life", section on 'COVID-19 communication resources'.) IMMUNIZATIONS — <span>Immunization schedules for adults in good health (figure 1) and those with chronic medical conditions (figure 2) are discussed elsewhere. (See "Standard immunizations for nonpregnant adults".) Vaccines for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) are discussed separately. (See "COVID-19: Vaccines".) TRAVEL CONSIDERATIONS FOR OLDER ADULTS — Older adults are among the most widely traveled members of society. In general, immunization strategies and travel advice are the same as for yo
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
mong the most widely traveled members of society. In general, immunization strategies and travel advice are the same as for younger adults. (See "Travel advice" and "Immunizations for travel".) <span>However, some live-attenuated organism vaccines may be harmful in some older individuals and should only be given when the risk is high and there is no alternative [101]. The best-studied of these is yellow fever vaccine. Death and hospitalization following yellow fever vaccination are 3.5 times more likely in those aged 65 to 74 years and nine times more likely in those >75 years compared with younger individuals [102]. (See "Yellow fever: Treatment and prevention", section on 'Whom to vaccinate'.) Chemoprophylaxis for malaria may be challenging in older persons, particularly those with heart disease due to side effects of certain agents (eg, mefloquine may produce dizziness, chan
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ose aged 65 to 74 years and nine times more likely in those >75 years compared with younger individuals [102]. (See "Yellow fever: Treatment and prevention", section on 'Whom to vaccinate'.) <span>Chemoprophylaxis for malaria may be challenging in older persons, particularly those with heart disease due to side effects of certain agents (eg, mefloquine may produce dizziness, change in mental status, and bradycardia or prolonged QT intervals). There are many alternative regimens for malaria prophylaxis, but familiarity with current resistance patterns is essential and should guide one’s choice for chemoprophylaxis. Clinicians are referred to the Centers for Disease Control and Prevention (CDC) website for the latest recommendations based on geography and local resistance patterns. (See "Prevention