Edited, memorised or added to reading queue
on 01-Nov-2016 (Tue)
Do you want BuboFlash to help you learning these things? Click here to log in or create user.
Flashcard 1411340700940
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itExcitatory postsynaptic potentials (EPSPs) are synaptic inputs that depolarize the postsynaptic cell
Original toplevel document (pdf)
cannot see any pdfsFlashcard 1411342273804
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itExcitatory postsynaptic potentials (EPSPs) are synaptic inputs that depolarize the postsynaptic cell
Original toplevel document (pdf)
cannot see any pdfsFlashcard 1411343846668
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itExcitatory postsynaptic potentials (EPSPs) are synaptic inputs that depolarize the postsynaptic cell
Original toplevel document (pdf)
cannot see any pdfsFlashcard 1411345419532
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itHyposmotic urine is produced when there are low circulating levels of ADH (e.g., water drinking, central diabetes insipidus) or when ADH is ineffective (e.g., nephrogenic diabetes insipidus)
Original toplevel document (pdf)
cannot see any pdfsFlashcard 1411346992396
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itHyposmotic urine is produced when there are low circulating levels of ADH (e.g., water drinking, central diabetes insipidus) or when ADH is ineffective (e.g., nephrogenic diabetes insipidus)
Original toplevel document (pdf)
cannot see any pdfsFlashcard 1411348565260
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itHyposmotic urine is produced when there are low circulating levels of ADH (e.g., water drinking, central diabetes insipidus) or when ADH is ineffective (e.g., nephrogenic diabetes insipidus)
Original toplevel document (pdf)
cannot see any pdfsFlashcard 1411350138124
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itHyposmotic urine is produced when there are low circulating levels of ADH (e.g., water drinking, central diabetes insipidus) or when ADH is ineffective (e.g., nephrogenic diabetes insipidus)
Original toplevel document (pdf)
cannot see any pdfs| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411352759564
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Oxytocin is used to improve inadequate contractions when dystocia is diagnosed or to initiate contractions when labour induction is required
Flashcard 1411354332428
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Oxytocin is used to improve inadequate contractions when dystocia is diagnosed or to initiate contractions when labour induction is required
Flashcard 1411355905292
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Oxytocin is used to improve inadequate contractions when dystocia is diagnosed or to initiate contractions when labour induction is required
Flashcard 1411357478156
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Oxytocin is used to improve inadequate contractions when dystocia is diagnosed or to initiate contractions when labour induction is required
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411360361740
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Contra-indications to oxytocin administration in pregnancy: • Severe vaginal bleeding • Placenta previa • Hypotension • Abnormal lie (transverse, footling breech) • Prior classical or inverted-T uterine incision • Pelvic structural deformities wh
Flashcard 1411361934604
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Contra-indications to oxytocin administration in pregnancy: • Severe vaginal bleeding • Placenta previa • Hypotension • Abnormal lie (transverse, footling breech) • Prior classical or inverted-T uterine incision • Pelvic structural deformities which would lead to obstr
Flashcard 1411363507468
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Contra-indications to oxytocin administration in pregnancy: • Severe vaginal bleeding • Placenta previa • Hypotension • Abnormal lie (transverse, footling breech) • Prior classical or inverted-T uterine incision • Pelvic structural deformities which would lead to obstructed labour
Flashcard 1411365080332
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Contra-indications to oxytocin administration in pregnancy: • Severe vaginal bleeding • Placenta previa • Hypotension • Abnormal lie (transverse, footling breech) • Prior classical or inverted-T uterine incision • Pelvic structural deformities which would lead to obstructed labour
Flashcard 1411366653196
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Contra-indications to oxytocin administration in pregnancy: • Severe vaginal bleeding • Placenta previa • Hypotension • Abnormal lie (transverse, footling breech) • Prior classical or inverted-T uterine incision • Pelvic structural deformities which would lead to obstructed labour
Flashcard 1411368226060
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
ontra-indications to oxytocin administration in pregnancy: • Severe vaginal bleeding • Placenta previa • Hypotension • Abnormal lie (transverse, footling breech) • Prior classical or inverted-T uterine incision • <span>Pelvic structural deformities which would lead to obstructed labour<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411371896076
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Adverse Effects of oxytocin administration in pregnancy: • Fetal compromise (from uterine hyperstimulation = contraction >2 min long or >5 contractions/10 min) • Uterine rupture (hyperstimulation) • Water intoxication (ADH effect) • Hypoten
Flashcard 1411373468940
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Adverse Effects of oxytocin administration in pregnancy: • Fetal compromise (from uterine hyperstimulation = contraction >2 min long or >5 contractions/10 min) • Uterine rupture (hyperstimulation) • Water intoxication (ADH effect) • Hypotension (Vasodilatation)</s
Flashcard 1411375041804
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Adverse Effects of oxytocin administration in pregnancy: • Fetal compromise (from uterine hyperstimulation = contraction >2 min long or >5 contractions/10 min) • Uterine rupture (hyperstimulation) • Water intoxication (ADH effect) • Hypotension (Vasodilatation)
Flashcard 1411376614668
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Adverse Effects of oxytocin administration in pregnancy: • Fetal compromise (from uterine hyperstimulation = contraction >2 min long or >5 contractions/10 min) • Uterine rupture (hyperstimulation) • Water intoxication (ADH effect) • Hypotension (Vasodilatation)
Flashcard 1411378187532
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
head>Adverse Effects of oxytocin administration in pregnancy: • Fetal compromise (from uterine hyperstimulation = contraction >2 min long or >5 contractions/10 min) • Uterine rupture (hyperstimulation) • Water intoxication (ADH effect) • Hypotension (Vasodilatation)<html>
Flashcard 1411379760396
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
of oxytocin administration in pregnancy: • Fetal compromise (from uterine hyperstimulation = contraction >2 min long or >5 contractions/10 min) • Uterine rupture (hyperstimulation) • Water intoxication (ADH effect) • <span>Hypotension (Vasodilatation)<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411382643980
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
For augmentation of labour using oxytocin (different protocols may be used – this is one example): • Initial dose: 1 – 2 mU/min • Increase Interval: every 30 min • Dosage Increment: 1 – 2 mU • Usual Dose for Good Labour: 8 – 12 mU/min but may vary
Flashcard 1411384741132
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
For augmentation of labour using oxytocin (different protocols may be used – this is one example): • Initial dose: 1 – 2 mU/min • Increase Interval: every 30 min • Dosage Increment: 1 – 2 mU • Usual Dose for Good Labour: 8 – 12 mU/min but may vary
Flashcard 1411386313996
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
For augmentation of labour using oxytocin (different protocols may be used – this is one example): • Initial dose: 1 – 2 mU/min • Increase Interval: every 30 min • Dosage Increment: 1 – 2 mU • Usual Dose for Good Labour: 8 – 12 mU/min but may vary
Flashcard 1411387886860
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
n>For augmentation of labour using oxytocin (different protocols may be used – this is one example): • Initial dose: 1 – 2 mU/min • Increase Interval: every 30 min • Dosage Increment: 1 – 2 mU • Usual Dose for Good Labour: <span>8 – 12 mU/min but may vary<span><body><html>
Flashcard 1411389459724
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1411391294732
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411394440460
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
maternal indications for assisted vag birth: • Failure to deliver spontaneously in the second stage • Conditions which require a shortened second stage • Conditions which contraindicate pushing • Inefficient maternal effort
Flashcard 1411396013324
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
maternal indications for assisted vag birth: • Failure to deliver spontaneously in the second stage • Conditions which require a shortened second stage • Conditions which contraindicate pushing • Inefficient maternal effort
Flashcard 1411397586188
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
maternal indications for assisted vag birth: • Failure to deliver spontaneously in the second stage • Conditions which require a shortened second stage • Conditions which contraindicate pushing • Inefficient maternal effort
Flashcard 1411399159052
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
d><head>maternal indications for assisted vag birth: • Failure to deliver spontaneously in the second stage • Conditions which require a shortened second stage • Conditions which contraindicate pushing • Inefficient maternal effort <html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411402042636
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Contra-indications for operative delivery (forceps or vacuum): • Non-cephalic presentation, face or brow • Unengaged head • Incompletely dilated cervix • Low probability of success
Flashcard 1411403615500
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Contra-indications for operative delivery (forceps or vacuum): • Non-cephalic presentation, face or brow • Unengaged head • Incompletely dilated cervix • Low probability of success
Flashcard 1411405188364
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Contra-indications for operative delivery (forceps or vacuum): • Non-cephalic presentation, face or brow • Unengaged head • Incompletely dilated cervix • Low probability of success
Flashcard 1411406761228
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Contra-indications for operative delivery (forceps or vacuum): • Non-cephalic presentation, face or brow • Unengaged head • Incompletely dilated cervix • Low probability of success
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411411217676
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Contra-indications Specific to Vacuum: • <34 weeks’ gestation • Deflexed attitude of fetal head • Need for rotation • Fetal conditions (bleeding disorder, demineralization disorder)
Flashcard 1411412790540
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Contra-indications Specific to Vacuum: • <34 weeks’ gestation • Deflexed attitude of fetal head • Need for rotation • Fetal conditions (bleeding disorder, demineralization disorder)
Flashcard 1411414363404
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Contra-indications Specific to Vacuum: • <34 weeks’ gestation • Deflexed attitude of fetal head • Need for rotation • Fetal conditions (bleeding disorder, demineralization disorder)
Flashcard 1411415936268
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Contra-indications Specific to Vacuum: • <34 weeks’ gestation • Deflexed attitude of fetal head • Need for rotation • Fetal conditions (bleeding disorder, demineralization disorder)
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411418819852
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Prerequisites for application of vacuum extractor or forceps: • Vertex presentation • Vertex engaged • Term or near term fetus • Cervix fully dilated • Membranes ruptured • Adequate anesthesia • Adequate maternal pelvis by cli
Flashcard 1411420392716
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Prerequisites for application of vacuum extractor or forceps: • Vertex presentation • Vertex engaged • Term or near term fetus • Cervix fully dilated • Membranes ruptured • Adequate anesthesia • Adequate maternal pelvis by clinical assessment • Mat
Flashcard 1411421965580
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Prerequisites for application of vacuum extractor or forceps: • Vertex presentation • Vertex engaged • Term or near term fetus • Cervix fully dilated • Membranes ruptured • Adequate anesthesia • Adequate maternal pelvis by clinical assessment • Maternal bladder empty • Backup plan
Flashcard 1411423538444
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Prerequisites for application of vacuum extractor or forceps: • Vertex presentation • Vertex engaged • Term or near term fetus • Cervix fully dilated • Membranes ruptured • Adequate anesthesia • Adequate maternal pelvis by clinical assessment • Maternal bladder empty • Backup plan (if forceps or vacuum not su
Flashcard 1411425111308
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Prerequisites for application of vacuum extractor or forceps: • Vertex presentation • Vertex engaged • Term or near term fetus • Cervix fully dilated • Membranes ruptured • Adequate anesthesia • Adequate maternal pelvis by clinical assessment • Maternal bladder empty • Backup plan (if forceps or vacuum not successful may need CS)</spa
Flashcard 1411426684172
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Prerequisites for application of vacuum extractor or forceps: • Vertex presentation • Vertex engaged • Term or near term fetus • Cervix fully dilated • Membranes ruptured • Adequate anesthesia • Adequate maternal pelvis by clinical assessment • Maternal bladder empty • Backup plan (if forceps or vacuum not successful may need CS)<html>
Flashcard 1411428257036
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
pan>Prerequisites for application of vacuum extractor or forceps: • Vertex presentation • Vertex engaged • Term or near term fetus • Cervix fully dilated • Membranes ruptured • Adequate anesthesia • Adequate <span>maternal pelvis by clinical assessment • Maternal bladder empty • Backup plan (if forceps or vacuum not successful may need CS)<span><body><html>
Flashcard 1411429829900
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
tractor or forceps: • Vertex presentation • Vertex engaged • Term or near term fetus • Cervix fully dilated • Membranes ruptured • Adequate anesthesia • Adequate maternal pelvis by clinical assessment • <span>Maternal bladder empty • Backup plan (if forceps or vacuum not successful may need CS)<span><body><html>
Flashcard 1411431402764
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
tex presentation • Vertex engaged • Term or near term fetus • Cervix fully dilated • Membranes ruptured • Adequate anesthesia • Adequate maternal pelvis by clinical assessment • Maternal bladder empty • <span>Backup plan (if forceps or vacuum not successful may need CS)<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411434286348
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Risks of Assisted Vaginal Birth: • Maternal soft tissue trauma • Fetal scalp trauma (hemorrhage, laceration) • Increased risk of intra-ventricular hemorrhage with multiple procedures • Fetal subgaleal or subaponeurotic hemorrhage wit
Flashcard 1411435859212
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Risks of Assisted Vaginal Birth: • Maternal soft tissue trauma • Fetal scalp trauma (hemorrhage, laceration) • Increased risk of intra-ventricular hemorrhage with multiple procedures • Fetal subgaleal or subaponeurotic hemorrhage with vacuum
Flashcard 1411437432076
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Risks of Assisted Vaginal Birth: • Maternal soft tissue trauma • Fetal scalp trauma (hemorrhage, laceration) • Increased risk of intra-ventricular hemorrhage with multiple procedures • Fetal subgaleal or subaponeurotic hemorrhage with vacuum
Flashcard 1411439004940
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Risks of Assisted Vaginal Birth: • Maternal soft tissue trauma • Fetal scalp trauma (hemorrhage, laceration) • Increased risk of intra-ventricular hemorrhage with multiple procedures • Fetal subgaleal or subaponeurotic hemorrhage with vacuum
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411441888524
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Most Common Indications for C/S: • Repeat C-Section • Dystocia • Breech presentation and other malpresentations • Non-reassuring fetal status
Flashcard 1411443461388
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Most Common Indications for C/S: • Repeat C-Section • Dystocia • Breech presentation and other malpresentations • Non-reassuring fetal status
Flashcard 1411445034252
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Most Common Indications for C/S: • Repeat C-Section • Dystocia • Breech presentation and other malpresentations • Non-reassuring fetal status
Flashcard 1411446607116
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Most Common Indications for C/S: • Repeat C-Section • Dystocia • Breech presentation and other malpresentations • Non-reassuring fetal status
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411449490700
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Absolute Indications for C/S: • Placenta Previa • Cord Prolapse • Previous Uterine Surgery • Previous Classical CS • Previous Uterine Rupture • Malpresentation (breech, transverse, brow) • Obstructed pel
Flashcard 1411451063564
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Absolute Indications for C/S: • Placenta Previa • Cord Prolapse • Previous Uterine Surgery • Previous Classical CS • Previous Uterine Rupture • Malpresentation (breech, transverse, brow) • Obstructed pelvis (mass, contracted
Flashcard 1411452636428
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Absolute Indications for C/S: • Placenta Previa • Cord Prolapse • Previous Uterine Surgery • Previous Classical CS • Previous Uterine Rupture • Malpresentation (breech, transverse, brow) • Obstructed pelvis (mass, contracted)
Flashcard 1411454209292
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Absolute Indications for C/S: • Placenta Previa • Cord Prolapse • Previous Uterine Surgery • Previous Classical CS • Previous Uterine Rupture • Malpresentation (breech, transverse, brow) • Obstructed pelvis (mass, contracted)
Flashcard 1411455782156
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Absolute Indications for C/S: • Placenta Previa • Cord Prolapse • Previous Uterine Surgery • Previous Classical CS • Previous Uterine Rupture • Malpresentation (breech, transverse, brow) • Obstructed pelvis (mass, contracted)
Flashcard 1411457355020
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Absolute Indications for C/S: • Placenta Previa • Cord Prolapse • Previous Uterine Surgery • Previous Classical CS • Previous Uterine Rupture • Malpresentation (breech, transverse, brow) • Obstructed pelvis (mass, contracted)
Flashcard 1411458927884
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
>Absolute Indications for C/S: • Placenta Previa • Cord Prolapse • Previous Uterine Surgery • Previous Classical CS • Previous Uterine Rupture • Malpresentation (breech, transverse, brow) • Obstructed pelvis (mass, contracted)<html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411461811468
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Relative Indications to C/S: • Failed Induction • Abnormal progression in labour • Pre-eclampsia/eclampsia • Diabetes • Cardiac disease • Placental abruption • Multiple Pregnancy</ht
Flashcard 1411463384332
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Relative Indications to C/S: • Failed Induction • Abnormal progression in labour • Pre-eclampsia/eclampsia • Diabetes • Cardiac disease • Placental abruption • Multiple Pregnancy
Flashcard 1411464957196
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Relative Indications to C/S: • Failed Induction • Abnormal progression in labour • Pre-eclampsia/eclampsia • Diabetes • Cardiac disease • Placental abruption • Multiple Pregnancy
Flashcard 1411466530060
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Relative Indications to C/S: • Failed Induction • Abnormal progression in labour • Pre-eclampsia/eclampsia • Diabetes • Cardiac disease • Placental abruption • Multiple Pregnancy
Flashcard 1411468102924
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Relative Indications to C/S: • Failed Induction • Abnormal progression in labour • Pre-eclampsia/eclampsia • Diabetes • Cardiac disease • Placental abruption • Multiple Pregnancy
Flashcard 1411469675788
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Relative Indications to C/S: • Failed Induction • Abnormal progression in labour • Pre-eclampsia/eclampsia • Diabetes • Cardiac disease • Placental abruption • Multiple Pregnancy
Flashcard 1411471248652
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Relative Indications to C/S: • Failed Induction • Abnormal progression in labour • Pre-eclampsia/eclampsia • Diabetes • Cardiac disease • Placental abruption • Multiple Pregnancy
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411474132236
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Risks of CS • Infection (wound, uterine, sepsis, urinary) • Hemorrhage • Atelectasis • Injury to bowel or bladder or ueter • Deep venous thrombosis • Pulmonary embolus • Longer recovery time</
Flashcard 1411475705100
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Risks of CS • Infection (wound, uterine, sepsis, urinary) • Hemorrhage • Atelectasis • Injury to bowel or bladder or ueter • Deep venous thrombosis • Pulmonary embolus • Longer recovery time
Flashcard 1411477277964
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Risks of CS • Infection (wound, uterine, sepsis, urinary) • Hemorrhage • Atelectasis • Injury to bowel or bladder or ueter • Deep venous thrombosis • Pulmonary embolus • Longer recovery time
Flashcard 1411478850828
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Risks of CS • Infection (wound, uterine, sepsis, urinary) • Hemorrhage • Atelectasis • Injury to bowel or bladder or ueter • Deep venous thrombosis • Pulmonary embolus • Longer recovery time
Flashcard 1411480423692
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Risks of CS • Infection (wound, uterine, sepsis, urinary) • Hemorrhage • Atelectasis • Injury to bowel or bladder or ueter • Deep venous thrombosis • Pulmonary embolus • Longer recovery time
Flashcard 1411481996556
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Risks of CS • Infection (wound, uterine, sepsis, urinary) • Hemorrhage • Atelectasis • Injury to bowel or bladder or ueter • Deep venous thrombosis • Pulmonary embolus • Longer recovery time
Flashcard 1411483569420
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Risks of CS • Infection (wound, uterine, sepsis, urinary) • Hemorrhage • Atelectasis • Injury to bowel or bladder or ueter • Deep venous thrombosis • Pulmonary embolus • Longer recovery time
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411486453004
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Non-pharmacologic Pain Relief Techniques in labour: 1. Reduction of painful stimuli 2. Activation of peripheral sensory receptors 3. Enhancement of descending inhibitory pathways
Flashcard 1411488025868
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Non-pharmacologic Pain Relief Techniques in labour: 1. Reduction of painful stimuli 2. Activation of peripheral sensory receptors 3. Enhancement of descending inhibitory pathways
Flashcard 1411489598732
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Non-pharmacologic Pain Relief Techniques in labour: 1. Reduction of painful stimuli 2. Activation of peripheral sensory receptors 3. Enhancement of descending inhibitory pathways
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411492482316
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Reduction of painful stimuli (non-pharm pain relief technique in labour): • Maternal movement and position change • Counter-pressure • Abdominal decompression
Flashcard 1411494055180
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Reduction of painful stimuli (non-pharm pain relief technique in labour): • Maternal movement and position change • Counter-pressure • Abdominal decompression
Flashcard 1411495628044
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Reduction of painful stimuli (non-pharm pain relief technique in labour): • Maternal movement and position change • Counter-pressure • Abdominal decompression
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411498511628
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Activation of peripheral sensory receptors (non-pharm pain relief technique for labour): • Superficial heat and cold • Immersion in water during labour • Touch and massage • Acupuncture and acupressure • Transcutaneous electrical nerve stimulation (TENS) • Intradermal injectio
Flashcard 1411500084492
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Activation of peripheral sensory receptors (non-pharm pain relief technique for labour): • Superficial heat and cold • Immersion in water during labour • Touch and massage • Acupuncture and acupressure • Transcutaneous electrical nerve stimulation (TENS) • Intradermal injection of sterile water • Aromatherapy</
Flashcard 1411501657356
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Activation of peripheral sensory receptors (non-pharm pain relief technique for labour): • Superficial heat and cold • Immersion in water during labour • Touch and massage • Acupuncture and acupressure • Transcutaneous electrical nerve stimulation (TENS) • Intradermal injection of sterile water • Aromatherapy
Flashcard 1411503230220
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Activation of peripheral sensory receptors (non-pharm pain relief technique for labour): • Superficial heat and cold • Immersion in water during labour • Touch and massage • Acupuncture and acupressure • Transcutaneous electrical nerve stimulation (TENS) • Intradermal injection of sterile water • Aromatherapy
Flashcard 1411504803084
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
y>Activation of peripheral sensory receptors (non-pharm pain relief technique for labour): • Superficial heat and cold • Immersion in water during labour • Touch and massage • Acupuncture and acupressure • Transcutaneous electrical nerve stimulation (TENS) • Intradermal injection of sterile water • Aromatherapy<body><html>
Flashcard 1411506375948
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
non-pharm pain relief technique for labour): • Superficial heat and cold • Immersion in water during labour • Touch and massage • Acupuncture and acupressure • Transcutaneous electrical nerve stimulation (TENS) • <span>Intradermal injection of sterile water • Aromatherapy<span><body><html>
Flashcard 1411507948812
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
13; • Superficial heat and cold • Immersion in water during labour • Touch and massage • Acupuncture and acupressure • Transcutaneous electrical nerve stimulation (TENS) • Intradermal injection of sterile water • <span>Aromatherapy<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411510832396
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Enhancement of descending inhibitory pathways (non-pharm pain relief technique for labour): • Attention focusing and distraction • Hypnosis and self-hypnosis • Music and audio analgesia • Biofeedback
Flashcard 1411512405260
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Enhancement of descending inhibitory pathways (non-pharm pain relief technique for labour): • Attention focusing and distraction • Hypnosis and self-hypnosis • Music and audio analgesia • Biofeedback
Flashcard 1411513978124
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Enhancement of descending inhibitory pathways (non-pharm pain relief technique for labour): • Attention focusing and distraction • Hypnosis and self-hypnosis • Music and audio analgesia • Biofeedback
Flashcard 1411515550988
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
tml>Enhancement of descending inhibitory pathways (non-pharm pain relief technique for labour): • Attention focusing and distraction • Hypnosis and self-hypnosis • Music and audio analgesia • Biofeedback<html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411518434572
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Pharm methods of pain relief in labour & birth: 1. Nitrous Oxide 2. Narcotics 3 . Peripheral Nerve Blocks – Pudendal Nerve Block 4 . Perineal Infiltration 5 . Regional Anaesthesia
Flashcard 1411520007436
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Pharm methods of pain relief in labour & birth: 1. Nitrous Oxide 2. Narcotics 3 . Peripheral Nerve Blocks – Pudendal Nerve Block 4 . Perineal Infiltration 5 . Regional Anaesthesia
Flashcard 1411521580300
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Pharm methods of pain relief in labour & birth: 1. Nitrous Oxide 2. Narcotics 3 . Peripheral Nerve Blocks – Pudendal Nerve Block 4 . Perineal Infiltration 5 . Regional Anaesthesia
Flashcard 1411523153164
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Pharm methods of pain relief in labour & birth: 1. Nitrous Oxide 2. Narcotics 3 . Peripheral Nerve Blocks – Pudendal Nerve Block 4 . Perineal Infiltration 5 . Regional Anaesthesia
Flashcard 1411524726028
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Pharm methods of pain relief in labour & birth: 1. Nitrous Oxide 2. Narcotics 3 . Peripheral Nerve Blocks – Pudendal Nerve Block 4 . Perineal Infiltration 5 . Regional Anaesthesia
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411527609612
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Nitrous Oxide as pharm pain relief in labour: • Entonox is self-administered. Deep inhalation begins as the woman is aware of the onset of a contraction. Useful in latter part of first stage of labour.
Flashcard 1411529182476
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Nitrous Oxide as pharm pain relief in labour: • Entonox is self-administered. Deep inhalation begins as the woman is aware of the onset of a contraction. Useful in latter part of first stage of labour.
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411532066060
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Narcotics as pharm pain relief in labour/birth: • Can be given IV and with PCA pumps • Usually combined with anti-emetic • Decrease fetal heart rate variability • Cause neonatal respiratory depression (reverse with naloxone given to newborn)
Flashcard 1411533638924
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Narcotics as pharm pain relief in labour/birth: • Can be given IV and with PCA pumps • Usually combined with anti-emetic • Decrease fetal heart rate variability • Cause neonatal respiratory depression (reverse with naloxone given to newborn)
Flashcard 1411535211788
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Narcotics as pharm pain relief in labour/birth: • Can be given IV and with PCA pumps • Usually combined with anti-emetic • Decrease fetal heart rate variability • Cause neonatal respiratory depression (reverse with naloxone given to newborn)
Flashcard 1411536784652
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Narcotics as pharm pain relief in labour/birth: • Can be given IV and with PCA pumps • Usually combined with anti-emetic • Decrease fetal heart rate variability • Cause neonatal respiratory depression (reverse with naloxone given to newborn)
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411539668236
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Peripheral Nerve Blocks – Pudendal Nerve Block as pharm pain relief in labour/birth • Used for analgesia of perineum in second stage • Useful when other regional analgesia is not available or ineffective
Flashcard 1411541241100
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Peripheral Nerve Blocks – Pudendal Nerve Block as pharm pain relief in labour/birth • Used for analgesia of perineum in second stage • Useful when other regional analgesia is not available or ineffective
Flashcard 1411542813964
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Peripheral Nerve Blocks – Pudendal Nerve Block as pharm pain relief in labour/birth • Used for analgesia of perineum in second stage • Useful when other regional analgesia is not available or ineffective
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411545697548
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Epidural block can provide effective pain relief throughout all stages of labour and delivery
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411548581132
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Epidural analgesia can be beneficial to women with dystocia secondary to hypotonic contractions whose labour will require augmentation with oxytocin. Provision of more effective pain relief facilitates th
Flashcard 1411550153996
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Epidural analgesia can be beneficial to women with dystocia secondary to hypotonic contractions whose labour will require augmentation with oxytocin. Provision of more effective pain relief facilitates the use of the most appropriate oxytocin do
Flashcard 1411551726860
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Epidural analgesia can be beneficial to women with dystocia secondary to hypotonic contractions whose labour will require augmentation with oxytocin. Provision of more effective pain relief facilitates the use of the most appropriate oxytocin dosage to improve labour progress</spa
Flashcard 1411553299724
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Epidural analgesia can be beneficial to women with dystocia secondary to hypotonic contractions whose labour will require augmentation with oxytocin. Provision of more effective pain relief facilitates the use of the most appropriate oxytocin dosage to improve labour progress
Flashcard 1411554872588
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
an>Epidural analgesia can be beneficial to women with dystocia secondary to hypotonic contractions whose labour will require augmentation with oxytocin. Provision of more effective pain relief facilitates the use of the most appropriate oxytocin dosage to improve labour progress<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411557756172
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Absolute Contra-Indications to a VBAC • Previous classical, inverted-T, or unknown incision • Other uterine surgeries (myomectomy) • Previous history of uterine rupture • Opinion of previous surgeon (important to get CS operative note) • Mother desires a re
Flashcard 1411559329036
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Absolute Contra-Indications to a VBAC • Previous classical, inverted-T, or unknown incision • Other uterine surgeries (myomectomy) • Previous history of uterine rupture • Opinion of previous surgeon (important to get CS operative note) • Mother desires a repeat CS
Flashcard 1411560901900
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Absolute Contra-Indications to a VBAC • Previous classical, inverted-T, or unknown incision • Other uterine surgeries (myomectomy) • Previous history of uterine rupture • Opinion of previous surgeon (important to get CS operative note) • Mother desires a repeat CS
Flashcard 1411562474764
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Absolute Contra-Indications to a VBAC • Previous classical, inverted-T, or unknown incision • Other uterine surgeries (myomectomy) • Previous history of uterine rupture • Opinion of previous surgeon (important to get CS operative note) • Mother desires a repeat CS
Flashcard 1411564047628
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
cations to a VBAC • Previous classical, inverted-T, or unknown incision • Other uterine surgeries (myomectomy) • Previous history of uterine rupture • Opinion of previous surgeon (important to get CS operative note) • <span>Mother desires a repeat CS<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411566931212
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Relative Contra-indications to a trial of VBAC • If induction required • Two or more previous lower segment CS scars • Multiple pregnancy • Breech presentation • Previous poor obstetrical history • Patient desires a tubal
Flashcard 1411568504076
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Relative Contra-indications to a trial of VBAC • If induction required • Two or more previous lower segment CS scars • Multiple pregnancy • Breech presentation • Previous poor obstetrical history • Patient desires a tubal sterilization
Flashcard 1411570076940
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Relative Contra-indications to a trial of VBAC • If induction required • Two or more previous lower segment CS scars • Multiple pregnancy • Breech presentation • Previous poor obstetrical history • Patient desires a tubal sterilization
Flashcard 1411571649804
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Relative Contra-indications to a trial of VBAC • If induction required • Two or more previous lower segment CS scars • Multiple pregnancy • Breech presentation • Previous poor obstetrical history • Patient desires a tubal sterilization
Flashcard 1411573222668
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Relative Contra-indications to a trial of VBAC • If induction required • Two or more previous lower segment CS scars • Multiple pregnancy • Breech presentation • Previous poor obstetrical history • Patient desires a tubal sterilization
Flashcard 1411574795532
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
dy>Relative Contra-indications to a trial of VBAC • If induction required • Two or more previous lower segment CS scars • Multiple pregnancy • Breech presentation • Previous poor obstetrical history • Patient desires a tubal sterilization<body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411577679116
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Risks of Trial of VBAC • Prolonged labour • Maternal fever and infection • Failed trial necessitating a repeat CS: risks of a CS done after a failed trial of VBAC are all higher when compared with an elective CS inclu
Flashcard 1411579251980
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Risks of Trial of VBAC • Prolonged labour • Maternal fever and infection • Failed trial necessitating a repeat CS: risks of a CS done after a failed trial of VBAC are all higher when compared with an elective CS including infection, bleeding, trauma etc
Flashcard 1411580824844
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Risks of Trial of VBAC • Prolonged labour • Maternal fever and infection • Failed trial necessitating a repeat CS: risks of a CS done after a failed trial of VBAC are all higher when compared with an elective CS including infection, bleeding, trauma etc. • Uterine rupture: with increased risk of maternal haemorrhage, fetal morbidity and mortality, possible need for Cesarean hysterectomy and ultimate loss of fertility <span>
Flashcard 1411582397708
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
onged labour • Maternal fever and infection • Failed trial necessitating a repeat CS: risks of a CS done after a failed trial of VBAC are all higher when compared with an elective CS including infection, bleeding, trauma etc. • <span>Uterine rupture: with increased risk of maternal haemorrhage, fetal morbidity and mortality, possible need for Cesarean hysterectomy and ultimate loss of fertility <span><body><html>
Flashcard 1411583970572
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
nfection • Failed trial necessitating a repeat CS: risks of a CS done after a failed trial of VBAC are all higher when compared with an elective CS including infection, bleeding, trauma etc. • Uterine rupture: with increased risk of <span>maternal haemorrhage, fetal morbidity and mortality, possible need for Cesarean hysterectomy and ultimate loss of fertility <span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411586854156
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Uterine Rupture: The risk of uterine rupture during a trial of VBAC increases considerably when induction of labour is required and with high dose oxytocin. Usually one of the first signs of uterine rupture is a profound fetal bradycardia with no recovery and constant lower abdominal pain in the
Flashcard 1411588427020
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Uterine Rupture: The risk of uterine rupture during a trial of VBAC increases considerably when induction of labour is required and with high dose oxytocin. Usually one of the first signs of uterine rupture is a profound fetal bradycardia with no recovery and constant lower abdominal pain in the mother. If the woman has an epidur
Flashcard 1411589999884
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
ad>Uterine Rupture: The risk of uterine rupture during a trial of VBAC increases considerably when induction of labour is required and with high dose oxytocin. Usually one of the first signs of uterine rupture is a profound fetal bradycardia with no recovery and constant lower abdominal pain in the mother. If the woman has an epidural for pain relief, the pain may not be experienced. Other signs and symptoms include: cessation of
Flashcard 1411591572748
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
isk of uterine rupture during a trial of VBAC increases considerably when induction of labour is required and with high dose oxytocin. Usually one of the first signs of uterine rupture is a profound fetal bradycardia with no recovery and <span>constant lower abdominal pain in the mother. If the woman has an epidural for pain relief, the pain may not be experienced. Other signs and symptoms include: cessation of uterine contractions, vaginal bleeding, recessio
Flashcard 1411593145612
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
ns of uterine rupture is a profound fetal bradycardia with no recovery and constant lower abdominal pain in the mother. If the woman has an epidural for pain relief, the pain may not be experienced. Other signs and symptoms include: <span>cessation of uterine contractions, vaginal bleeding, recession of the presenting part on vaginal examination (fetus may be extruded into the peritoneal cavity through the uterine incision), intra-abdominal haemorrhage,
Flashcard 1411594718476
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
fetal bradycardia with no recovery and constant lower abdominal pain in the mother. If the woman has an epidural for pain relief, the pain may not be experienced. Other signs and symptoms include: cessation of uterine contractions, <span>vaginal bleeding, recession of the presenting part on vaginal examination (fetus may be extruded into the peritoneal cavity through the uterine incision), intra-abdominal haemorrhage, and hypovolemic sh
Flashcard 1411596291340
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
with no recovery and constant lower abdominal pain in the mother. If the woman has an epidural for pain relief, the pain may not be experienced. Other signs and symptoms include: cessation of uterine contractions, vaginal bleeding, <span>recession of the presenting part on vaginal examination (fetus may be extruded into the peritoneal cavity through the uterine incision), intra-abdominal haemorrhage, and hypovolemic shock. Although a previous uterine scar is the most common reason for uterine rupture in our society, there are other causes. <
Flashcard 1411597864204
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
experienced. Other signs and symptoms include: cessation of uterine contractions, vaginal bleeding, recession of the presenting part on vaginal examination (fetus may be extruded into the peritoneal cavity through the uterine incision), <span>intra-abdominal haemorrhage, and hypovolemic shock. Although a previous uterine scar is the most common reason for uterine rupture in our society, there are other causes. <span><body><html>
Flashcard 1411599437068
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
d symptoms include: cessation of uterine contractions, vaginal bleeding, recession of the presenting part on vaginal examination (fetus may be extruded into the peritoneal cavity through the uterine incision), intra-abdominal haemorrhage, and <span>hypovolemic shock. Although a previous uterine scar is the most common reason for uterine rupture in our society, there are other causes. <span><body><html>
Flashcard 1411601009932
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
erine contractions, vaginal bleeding, recession of the presenting part on vaginal examination (fetus may be extruded into the peritoneal cavity through the uterine incision), intra-abdominal haemorrhage, and hypovolemic shock. Although a <span>previous uterine scar is the most common reason for uterine rupture in our society, there are other causes. <span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411603893516
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Causes of Uterine Rupture in pregnancy: • Uterine Scar: CS, myomectomy, previous uterine perforation during D&C, salpingectomy with cornual resection • Excessive Uterine Action: Oxytocin, prostaglandins, neglected obstructed labour • Trauma: ECV, Forceps, manual removal of placenta, trauma (motor vehicle, assault) • Mi
Flashcard 1411605466380
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Causes of Uterine Rupture in pregnancy: • Uterine Scar: CS, myomectomy, previous uterine perforation during D&C, salpingectomy with cornual resection • Excessive Uterine Action: Oxytocin, prostaglandins, neglected obstructed labour • Trauma: ECV, Forceps, manual removal of placenta, trauma (motor vehicle, assault) • Miscellaneous: multiparity, uterine anomalies, placenta accreta</htm
Flashcard 1411607039244
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Uterine Rupture in pregnancy: • Uterine Scar: CS, myomectomy, previous uterine perforation during D&C, salpingectomy with cornual resection • Excessive Uterine Action: Oxytocin, prostaglandins, neglected obstructed labour • <span>Trauma: ECV, Forceps, manual removal of placenta, trauma (motor vehicle, assault) • Miscellaneous: multiparity, uterine anomalies, placenta accreta<span><body><html>
Flashcard 1411609136396
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
&C, salpingectomy with cornual resection • Excessive Uterine Action: Oxytocin, prostaglandins, neglected obstructed labour • Trauma: ECV, Forceps, manual removal of placenta, trauma (motor vehicle, assault) • Miscellaneous: <span>multiparity, uterine anomalies, placenta accreta<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411612019980
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Management of Uterine Rupture: • Stabilize mother and treat hypovolemia • Call for assistance – nursing, pediatrician, anesthesia, respiratory tech. • Emergency laparotomy to deliver fetus, placenta and repair uterus.
Flashcard 1411613592844
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Management of Uterine Rupture: • Stabilize mother and treat hypovolemia • Call for assistance – nursing, pediatrician, anesthesia, respiratory tech. • Emergency laparotomy to deliver fetus, placenta and repair uterus.
Flashcard 1411615165708
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Management of Uterine Rupture: • Stabilize mother and treat hypovolemia • Call for assistance – nursing, pediatrician, anesthesia, respiratory tech. • Emergency laparotomy to deliver fetus, placenta and repair uterus.
Flashcard 1411618835724


| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1411623030028

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1411627224332

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1411630107916

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1411634302220

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1411638496524

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1411644001548

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1411648195852

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1411649506572

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1411656060172

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1411657895180

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1411662613772

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1411666808076

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1411671002380
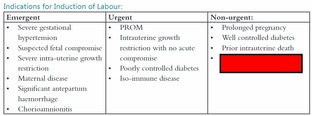
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411678866700
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Contra-indications to Induction • Placenta previa, vasa previa, cord presentation • Abnormal fetal lie • Prior classical CS scar or inverted T incision • Uterine surgery • Active genital herpes • Pelvic structu
Flashcard 1411680439564
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Contra-indications to Induction • Placenta previa, vasa previa, cord presentation • Abnormal fetal lie • Prior classical CS scar or inverted T incision • Uterine surgery • Active genital herpes • Pelvic structural deformiti
Flashcard 1411682012428
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Contra-indications to Induction • Placenta previa, vasa previa, cord presentation • Abnormal fetal lie • Prior classical CS scar or inverted T incision • Uterine surgery • Active genital herpes • Pelvic structural deformities • Invasive
Flashcard 1411683585292
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Contra-indications to Induction • Placenta previa, vasa previa, cord presentation • Abnormal fetal lie • Prior classical CS scar or inverted T incision • Uterine surgery • Active genital herpes • Pelvic structural deformities • Invasive cervical cancer</sp
Flashcard 1411685158156
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Contra-indications to Induction • Placenta previa, vasa previa, cord presentation • Abnormal fetal lie • Prior classical CS scar or inverted T incision • Uterine surgery • Active genital herpes • Pelvic structural deformities • Invasive cervical cancer
Flashcard 1411686731020
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Contra-indications to Induction • Placenta previa, vasa previa, cord presentation • Abnormal fetal lie • Prior classical CS scar or inverted T incision • Uterine surgery • Active genital herpes • Pelvic structural deformities • Invasive cervical cancer
Flashcard 1411688303884
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Contra-indications to Induction • Placenta previa, vasa previa, cord presentation • Abnormal fetal lie • Prior classical CS scar or inverted T incision • Uterine surgery • Active genital herpes • Pelvic structural deformities • Invasive cervical cancer
Flashcard 1411689876748
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
body>Contra-indications to Induction • Placenta previa, vasa previa, cord presentation • Abnormal fetal lie • Prior classical CS scar or inverted T incision • Uterine surgery • Active genital herpes • Pelvic structural deformities • Invasive cervical cancer<body><html>
Flashcard 1411691449612
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
o Induction • Placenta previa, vasa previa, cord presentation • Abnormal fetal lie • Prior classical CS scar or inverted T incision • Uterine surgery • Active genital herpes • Pelvic structural deformities • <span>Invasive cervical cancer<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411694333196
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Risks of Induction • Failure to achieve labour • Failure to achieve a vaginal birth • Uterine hyperstimulation with fetal compromise • Uterine hyperstimulation with uterine rupture • Maternal side-effects to medi
Flashcard 1411695906060
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Risks of Induction • Failure to achieve labour • Failure to achieve a vaginal birth • Uterine hyperstimulation with fetal compromise • Uterine hyperstimulation with uterine rupture • Maternal side-effects to medications
Flashcard 1411697478924
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Risks of Induction • Failure to achieve labour • Failure to achieve a vaginal birth • Uterine hyperstimulation with fetal compromise • Uterine hyperstimulation with uterine rupture • Maternal side-effects to medications
Flashcard 1411699051788
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Risks of Induction • Failure to achieve labour • Failure to achieve a vaginal birth • Uterine hyperstimulation with fetal compromise • Uterine hyperstimulation with uterine rupture • Maternal side-effects to medications
Flashcard 1411700624652
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
tml>Risks of Induction • Failure to achieve labour • Failure to achieve a vaginal birth • Uterine hyperstimulation with fetal compromise • Uterine hyperstimulation with uterine rupture • Maternal side-effects to medications<html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411705605388
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Options for induction of labour: 1 . If artificial rupture of membranes (ARM) is possible (cervix open, soft, membranes felt, head well applied to cervix) then do the ARM and consider starting oxytocin infusion. 2 . If ARM not possible (cervix long, closed,
Flashcard 1411707178252
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Options for induction of labour: 1 . If artificial rupture of membranes (ARM) is possible (cervix open, soft, membranes felt, head well applied to cervix) then do the ARM and consider starting oxytocin infusion. 2 . If ARM not possible (cervix long, closed, firm, posterior), then use a method of “cervical ripening” (medications or m
Flashcard 1411708751116
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Options for induction of labour: 1 . If artificial rupture of membranes (ARM) is possible (cervix open, soft, membranes felt, head well applied to cervix) then do the ARM and consider starting oxytocin infusion. 2 . If ARM not possible (cervix long, closed, firm, posterior), then use a method of “cervical ripening” (medications or methods to soften, efface, dilate cervix; will increase th
Flashcard 1411710323980
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
ns for induction of labour: 1 . If artificial rupture of membranes (ARM) is possible (cervix open, soft, membranes felt, head well applied to cervix) then do the ARM and consider starting oxytocin infusion. 2 . If ARM not possible (<span>cervix long, closed, firm, posterior), then use a method of “cervical ripening” (medications or methods to soften, efface, dilate cervix; will increase the success of the induction). Once cervix ripened then do ARM and sta
Flashcard 1411711896844
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
f membranes (ARM) is possible (cervix open, soft, membranes felt, head well applied to cervix) then do the ARM and consider starting oxytocin infusion. 2 . If ARM not possible (cervix long, closed, firm, posterior), then use a method of “<span>cervical ripening” (medications or methods to soften, efface, dilate cervix; will increase the success of the induction). Once cervix ripened then do ARM and start oxytocin infusion (same protocol as aug
Flashcard 1411713469708
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
ft, membranes felt, head well applied to cervix) then do the ARM and consider starting oxytocin infusion. 2 . If ARM not possible (cervix long, closed, firm, posterior), then use a method of “cervical ripening” (medications or methods to <span>soften, efface, dilate cervix; will increase the success of the induction). Once cervix ripened then do ARM and start oxytocin infusion (same protocol as augmentation of labour for dystocia). 3 . “Ripen
Flashcard 1411715042572
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
or methods to soften, efface, dilate cervix; will increase the success of the induction). Once cervix ripened then do ARM and start oxytocin infusion (same protocol as augmentation of labour for dystocia). 3 . “Ripen Cervix” with • <span>Prostaglandins (Prostin, Cervidil) • Foley catheter balloon in cervix • Oxytocin infusion (not as successful)<span><body><html>
Flashcard 1411716615436
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
ix; will increase the success of the induction). Once cervix ripened then do ARM and start oxytocin infusion (same protocol as augmentation of labour for dystocia). 3 . “Ripen Cervix” with • Prostaglandins (Prostin, Cervidil) • <span>Foley catheter balloon in cervix • Oxytocin infusion (not as successful)<span><body><html>
Flashcard 1411718188300
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
uction). Once cervix ripened then do ARM and start oxytocin infusion (same protocol as augmentation of labour for dystocia). 3 . “Ripen Cervix” with • Prostaglandins (Prostin, Cervidil) • Foley catheter balloon in cervix • <span>Oxytocin infusion (not as successful)<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411721071884
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Postterm pregnancies are at higher risk than term pregnancies of perinatal death (antepartum, intrapartum, and postpartum) due to anomalies (e.g. anencephaly), intra-uterine infection, and asphyxia with and without meconium
Flashcard 1411722644748
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Postterm pregnancies are at higher risk than term pregnancies of perinatal death (antepartum, intrapartum, and postpartum) due to anomalies (e.g. anencephaly), intra-uterine infection, and asphyxia with and without meconium
Flashcard 1411724217612
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Postterm pregnancies are at higher risk than term pregnancies of perinatal death (antepartum, intrapartum, and postpartum) due to anomalies (e.g. anencephaly), intra-uterine infection, and asphyxia with and without meconium
Flashcard 1411725790476
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Postterm pregnancies are at higher risk than term pregnancies of perinatal death (antepartum, intrapartum, and postpartum) due to anomalies (e.g. anencephaly), intra-uterine infection, and asphyxia with and without meconium
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411728674060
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Post term pregnancies are also at a higher risk of neonatal morbidity (e.g. macrosomia, shoulder dystocia, meconium aspiration syndrome, admission to NICU, need for oxygen, intubation, pneumonia, and seizures)
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411731557644
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Management of post-term pregnancy: 1 . Ensure that accurate gestational age is established (make sure to do early ultrasound) 2 . No evidence for inducing labour or initiating serial fetal monitoring prior to 41 weeks 3 . After 41 weeks’ gestation, offer women either induction of labour or serial fet
Flashcard 1411733130508
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Management of post-term pregnancy: 1 . Ensure that accurate gestational age is established (make sure to do early ultrasound) 2 . No evidence for inducing labour or initiating serial fetal monitoring prior to 41 weeks 3 . After 41 weeks’ gestation, offer women either induction of labour or serial fetal monitoring 4 . If induction selected, follow protocol above for inducti
Flashcard 1411734703372
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
e gestational age is established (make sure to do early ultrasound) 2 . No evidence for inducing labour or initiating serial fetal monitoring prior to 41 weeks 3 . After 41 weeks’ gestation, offer women either induction of labour or <span>serial fetal monitoring 4 . If induction selected, follow protocol above for induction of labour<span><body><html>
Flashcard 1411736538380
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itHyposmotic urine is produced when there are low circulating levels of ADH (e.g., water drinking, central diabetes insipidus) or when ADH is ineffective (e.g., nephrogenic diabetes insipidus)
Original toplevel document (pdf)
cannot see any pdfsFlashcard 1411738897676
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itHyposmotic urine is produced when there are low circulating levels of ADH (e.g., water drinking, central diabetes insipidus) or when ADH is ineffective (e.g., nephrogenic diabetes insipidus)
Original toplevel document (pdf)
cannot see any pdfsFlashcard 1411741256972
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itHyposmotic urine is produced when there are low circulating levels of ADH (e.g., water drinking, central diabetes insipidus) or when ADH is ineffective (e.g., nephrogenic diabetes insipidus)
Original toplevel document (pdf)
cannot see any pdfsFlashcard 1411743091980
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itNegative feedback is the most important and common mechanism for regu- lating hormone secretion
Original toplevel document (pdf)
cannot see any pdfsFlashcard 1411744664844
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itNegative feedback is the most important and common mechanism for regu- lating hormone secretion
Original toplevel document (pdf)
cannot see any pdfsFlashcard 1411746237708
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itNegative feedback is the most important and common mechanism for regu- lating hormone secretion
Original toplevel document (pdf)
cannot see any pdfsFlashcard 1411751218444
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itAll steroid hormones are derivatives of cholesterol
Original toplevel document (pdf)
cannot see any pdfsFlashcard 1411752791308
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itAll steroid hormones are derivatives of cholesterol
Original toplevel document (pdf)
cannot see any pdfs| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Żelazna dama ze srebrnymi ustami. Taka była Zyta Gilowska
[imagelink] REKLAMA Żelazna dama ze srebrnymi ustami. Taka była Zyta Gilowska Fot. PAP/Radek Pietruszka <span>Zwolenniczka wolnego rynku i zmniejszania obciążeń podatkowych, a do tego jedna z najbardziej wyrazistych kobiet w polskiej polityce. Zdaniem ekspertów, to w dużej mierze dzięki jej reformom nasz kraj suchą stopą przebrnął przez światowy kryzys gospodarczy. "Żelazna dama polskich finansów" podejmowała decyzje, przy których blednie nawet dzisiejszy program Rodzina 500+. Wspominamy Zytę Gilowską, byłą wicepremier i minister finansów, zmarłą w kwietniu tego roku. - Przydepnijcie w końcu gardło swej rewolucyjnej pieśni i zamiast na okrągło śpiewać: "dać, dać, dać", zacznijcie powtarzać: "szukać oszczędności, likwidować bałagan, og
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
ORP Kormoran – Wikipedia, wolna encyklopedia
ie armata Wróbel II kaliber 23 mm 3 karabiny maszynowe WKM-Bm 12,7 mm 2 wyrzutnie pocisków rakietowych Grom Wyposażenie System dowodzenia SCOT-M Pojazdy głębinowe Double Eagle Mk. III Kongsberg Hugin i Morświn Załoga 45 oficerów i marynarzy <span>ORP Kormoran (601) – zwodowany 4 września 2015 roku w stoczni Remontowa Shipbuilding w Gdańsku, polski niszczyciel min, okręt wiodący typu Kormoran II, przeznaczony do poszukiwania i zwalczania min morskich na wodach polskiej strefy ekonomicznej oraz w grupach taktycznych na Morzu Bałtyckim i Północnym. W celu zapewnienia amagnetyczności, kadłub jednostki o wyporności standardowej 830 ton i długości całkowitej 58,5 metra, zbudowany został z austenitycznej stali nierdzewnej. Wejście okrętu do służby w Marynarce Wojennej przewidziane jest na listopad 2016 roku. Spis treści [ukryj] 1 Budowa 2 Konstrukcja 2.1 Wyposażenie 2.2 Uzbrojenie 3 Służba 4 Przypisy Budowa[edytuj] Kontrakt między Inspektoratem Uzbrojenia a konsorcjum




| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |

| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |

{kind=link}
{kind=link}
{kind=link}
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Work breakdown structure - Wikipedia
clusive elements 3.2 Plan outcomes, not actions 3.3 Level of detail 3.4 Coding scheme 3.5 Terminal element 3.6 Consistent to norms 4 Example 5 Misconceptions 6 See also 7 References 8 Further reading 9 External links Overview[edit] <span>WBS is a hierarchical and incremental decomposition of the project into phases, deliverables and work packages. It is a tree structure, which shows a subdivision of effort required to achieve an objective; for example a program, project, and contract. [2] In a project or contract, the WBS is developed by starting with the end objective and successively subdividing it into manageable components in terms of size, duration, and responsibility (e.g., systems, subsystems, components, tasks, subtasks, and work packages) which include all steps necessary to achieve the objective. [imagelink] [emptylink] Example of work breakdown structure applied in a NASA reporting structure. [2] The work breakdown structure provides a common framework for the nat
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Work breakdown structure - Wikipedia
to the DoD handbook, but is intended for more general application. [12] Design principles[edit] 100% rule[edit] An important design principle for work breakdown structures is called the 100% rule. [13] It has been defined as follows: <span>The 100% rule states that the WBS includes 100% of the work defined by the project scope and captures all deliverables – internal, external, interim – in terms of the work to be completed, including project management. The 100% rule is one of the most important principles guiding the development, decomposition and evaluation of the WBS. The rule applies at all levels within the hierarchy: the sum of the work at the "child" level must equal 100% of the work represented by the "parent" and the WBS should not include any work that falls outside the actual scope of the project, that is, it cannot include more than 100% of the work… It is important to remember that the 100% rule also applies to the activity level. The work represented by the activities in each
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Work breakdown structure - Wikipedia
deliverable defined by the WBS. There are several heuristics or "rules of thumb" used when determining the appropriate duration of an activity or group of activities necessary to produce a specific deliverable defined by the WBS. <span>The first is the "80 hour rule" which means that no single activity or group of activities at the lowest level of detail of the WBS to produce a single deliverable should be more than 80 hours of effort. The second rule of thumb is that no activity or group of activities at the lowest level of detail of the WBS should be longer than a single reporting period. Thus if the project team is reporting progress monthly, then no single activity or series of activities should be longer than one month long. The last heuristic is the "if it makes sense" rule. Applying this rule of thumb, one can apply "common sense" when creating the duration of a single activity or group of activities necessary to produce a deliverable defined by the WBS. A work package at the activity level is a task that: can be realistically and confidently estimated; makes no sense practically to break down any further; can be completed in accord
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1412281011468
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itLong-loop feedback means that the hormone feeds back all the way to the hypothalamic-pituitary axis
Original toplevel document (pdf)
cannot see any pdfsFlashcard 1412284681484
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Work breakdown structure - Wikipedia
sense practically to break down any further; can be completed in accordance with one of the heuristics defined above; produces a deliverable which is measurable; and forms a unique package of work which can be outsourced or contracted out. <span>Coding scheme[edit] It is common for work breakdown structure elements to be numbered sequentially to reveal the hierarchical structure. The purpose for the numbering is to provide a consistent approach to identifying and managing the WBS across like systems regardless of vendor or service. [16] For example, 1.1.2 Propulsion (in the example below) identifies this item as a Level 3 WBS element, since there are three numbers separated by a decimal point. A coding scheme also helps WBS elements to be recognized in any written context and allows for mapping to the WBS Dictionary. [17] A practical example of the WBS coding scheme is [18] 1.0 Aircraft System 1.1 Air Vehicle 1.1.1 Airframe 1.1.1.1 Airframe Integration, Assembly, Test and Checkout 1.1.1.2 Fuselage 1.1.1.3 Wing 1.1.1.4 Empennage 1.1.1.5 Nacelle 1.1.1.6 Other Airframe Components 1..n (Specify) 1.1.2 Propulsion 1.1.3 Vehicle Subsystems 1.1.4 Avionics 1.2 System Engineering 1.3 Program Management 1.4 System Test and Evaluation 1.5 Training 1.6 Data 1.7 Peculiar Support Equipment 1.8 Common Support Equipment 1.9 Operational/Site Activation 1.10 Industrial Facilities 1.11 Initial Spares and Repair Parts An example in the software industry would be as follows: [19] 1267.1 Systems Integration 1267.1.1 Requirements Definition 1267.1.2 Regulations 1267.1.3 Scheduling 1267.1.4 Monitoring & Control 1267.1.5 Procurement Management 1267.1.6 Closeout 1267.2 Design 1267.2.1 Conceptual Design 1267.2.2 Preliminary Design 1267.2.3 Final Design Terminal element[edit] The lowest element in a tree structure, a ter
Flashcard 1414088232204
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1414091377932
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Uterine “After Pains” • The uterus contracts tonically causing “after pains” • Worse during breast feeding • Tends to subside by the third post-partum day
Flashcard 1414092950796
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Uterine “After Pains” • The uterus contracts tonically causing “after pains” • Worse during breast feeding • Tends to subside by the third post-partum day
Flashcard 1414094523660
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Uterine “After Pains” • The uterus contracts tonically causing “after pains” • Worse during breast feeding • Tends to subside by the third post-partum day
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1414097407244
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Lochia • The lochia refers to the sloughing of the uterine decidual tissue • Occurs in the early post-partum period • Quantity and color progressively changes as the puerperium progresses • Red in the first few days and called lochia rubra. Afte
Flashcard 1414098980108
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Lochia • The lochia refers to the sloughing of the uterine decidual tissue • Occurs in the early post-partum period • Quantity and color progressively changes as the puerperium progresses • Red in the first few days and called lochia rubra. After 3 to 4 days, it becomes pale – lochia
Flashcard 1414100552972
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Lochia • The lochia refers to the sloughing of the uterine decidual tissue • Occurs in the early post-partum period • Quantity and color progressively changes as the puerperium progresses • Red in the first few days and called lochia rubra. After 3 to 4 days, it becomes pale – lochia serosa – and by the 10th day, it becomes whitish or yellow – lochia alba
Flashcard 1414102125836
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
ead>Lochia • The lochia refers to the sloughing of the uterine decidual tissue • Occurs in the early post-partum period • Quantity and color progressively changes as the puerperium progresses • Red in the first few days and called lochia rubra. After 3 to 4 days, it becomes pale – lochia serosa – and by the 10th day, it becomes whitish or yellow – lochia alba. The lochia may persist for up to 4 we
Flashcard 1414103698700
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
• The lochia refers to the sloughing of the uterine decidual tissue • Occurs in the early post-partum period • Quantity and color progressively changes as the puerperium progresses • Red in the first few days and called lochia <span>rubra. After 3 to 4 days, it becomes pale – lochia serosa – and by the 10th day, it becomes whitish or yellow – lochia alba. The lochia may persist for up to 4 weeks and in some cases beyond.
Flashcard 1414105271564
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
refers to the sloughing of the uterine decidual tissue • Occurs in the early post-partum period • Quantity and color progressively changes as the puerperium progresses • Red in the first few days and called lochia rubra. After <span>3 to 4 days, it becomes pale – lochia serosa – and by the 10th day, it becomes whitish or yellow – lochia alba. The lochia may persist for up to 4 weeks and in some cases beyond. • The su
Flashcard 1414106844428
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
of the uterine decidual tissue • Occurs in the early post-partum period • Quantity and color progressively changes as the puerperium progresses • Red in the first few days and called lochia rubra. After 3 to 4 days, it becomes <span>pale – lochia serosa – and by the 10th day, it becomes whitish or yellow – lochia alba. The lochia may persist for up to 4 weeks and in some cases beyond. • The superficial layer of the endometrium bec
Flashcard 1414108417292
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
3; • Occurs in the early post-partum period • Quantity and color progressively changes as the puerperium progresses • Red in the first few days and called lochia rubra. After 3 to 4 days, it becomes pale – lochia serosa – and by the <span>10th day, it becomes whitish or yellow – lochia alba. The lochia may persist for up to 4 weeks and in some cases beyond. • The superficial layer of the endometrium becomes necrotic and
Flashcard 1414109990156
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
rly post-partum period • Quantity and color progressively changes as the puerperium progresses • Red in the first few days and called lochia rubra. After 3 to 4 days, it becomes pale – lochia serosa – and by the 10th day, it becomes <span>whitish or yellow – lochia alba. The lochia may persist for up to 4 weeks and in some cases beyond. • The superficial layer of the endometrium becomes necrotic and replaced by the newly regenerated layer from the
Flashcard 1414111563020
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
nges as the puerperium progresses • Red in the first few days and called lochia rubra. After 3 to 4 days, it becomes pale – lochia serosa – and by the 10th day, it becomes whitish or yellow – lochia alba. The lochia may persist for up to <span>4 weeks and in some cases beyond. • The superficial layer of the endometrium becomes necrotic and replaced by the newly regenerated layer from the basal layer. • The basal layer
Flashcard 1414113135884
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
the 10th day, it becomes whitish or yellow – lochia alba. The lochia may persist for up to 4 weeks and in some cases beyond. • The superficial layer of the endometrium becomes necrotic and replaced by the newly regenerated layer from the <span>basal layer. • The basal layer is never shed and remains intact<span><body><html>
Flashcard 1414114708748
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
whitish or yellow – lochia alba. The lochia may persist for up to 4 weeks and in some cases beyond. • The superficial layer of the endometrium becomes necrotic and replaced by the newly regenerated layer from the basal layer. • The <span>basal layer is never shed and remains intact<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1414117592332
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Involution of the Uterus • The process where the pregnant uterus returns to its pre-pregnancy size. • The uterus contracts after the expulsion of the placenta. • The previously hypertrophied muscle cells shrink, rather than reduce in number. • The fundus remains below
Flashcard 1414119165196
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Involution of the Uterus • The process where the pregnant uterus returns to its pre-pregnancy size. • The uterus contracts after the expulsion of the placenta. • The previously hypertrophied muscle cells shrink, rather than reduce in number. • The fundus remains below the umbilicus within 24 hours of delivery, midway between the pubi
Flashcard 1414120738060
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
/head>Involution of the Uterus • The process where the pregnant uterus returns to its pre-pregnancy size. • The uterus contracts after the expulsion of the placenta. • The previously hypertrophied muscle cells shrink, rather than reduce in number. • The fundus remains below the umbilicus within 24 hours of delivery, midway between the pubic symphysis and the umbilicus within 1 week postpartum, impalpable per abdomen by 2 wee
Flashcard 1414122310924
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
us returns to its pre-pregnancy size. • The uterus contracts after the expulsion of the placenta. • The previously hypertrophied muscle cells shrink, rather than reduce in number. • The fundus remains below the umbilicus within <span>24 hours of delivery, midway between the pubic symphysis and the umbilicus within 1 week postpartum, impalpable per abdomen by 2 weeks and returns to normal size by 6 weeks post-partum.
Flashcard 1414123883788
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
ion of the placenta. • The previously hypertrophied muscle cells shrink, rather than reduce in number. • The fundus remains below the umbilicus within 24 hours of delivery, midway between the pubic symphysis and the umbilicus within <span>1 week postpartum, impalpable per abdomen by 2 weeks and returns to normal size by 6 weeks post-partum. • The myometrium contracts the uterine vasculature (ischemic appearance).</spa
Flashcard 1414125456652
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
pertrophied muscle cells shrink, rather than reduce in number. • The fundus remains below the umbilicus within 24 hours of delivery, midway between the pubic symphysis and the umbilicus within 1 week postpartum, impalpable per abdomen by <span>2 weeks and returns to normal size by 6 weeks post-partum. • The myometrium contracts the uterine vasculature (ischemic appearance).<span><body><html>
Flashcard 1414127029516
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
r than reduce in number. • The fundus remains below the umbilicus within 24 hours of delivery, midway between the pubic symphysis and the umbilicus within 1 week postpartum, impalpable per abdomen by 2 weeks and returns to normal size by <span>6 weeks post-partum. • The myometrium contracts the uterine vasculature (ischemic appearance).<span><body><html>
Flashcard 1414128602380
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
24 hours of delivery, midway between the pubic symphysis and the umbilicus within 1 week postpartum, impalpable per abdomen by 2 weeks and returns to normal size by 6 weeks post-partum. • The myometrium contracts the uterine vasculature (<span>ischemic appearance).<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1414131485964
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Sub-involution • The delay in the normal postpartum changes in the uterus results in delayed involution where the uterus fails to go back to its normal size. • The two most common causes are retained products of conception and pelvic infection. • Presents as persistent vaginal discharge, mild or profuse bleeding. • Treatment d
Flashcard 1414133058828
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Sub-involution • The delay in the normal postpartum changes in the uterus results in delayed involution where the uterus fails to go back to its normal size. • The two most common causes are retained products of conception and pelvic infection. • Presents as persistent vaginal discharge, mild or profuse bleeding. • Treatment depends on the etiology. • Retained products of conception may res
Flashcard 1414134631692
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Sub-involution • The delay in the normal postpartum changes in the uterus results in delayed involution where the uterus fails to go back to its normal size. • The two most common causes are retained products of conception and pelvic infection. • Presents as persistent vaginal discharge, mild or profuse bleeding. • Treatment depends on the etiology. • Retained products of conception may respond to Misoprostol (
Flashcard 1414136204556
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
in the normal postpartum changes in the uterus results in delayed involution where the uterus fails to go back to its normal size. • The two most common causes are retained products of conception and pelvic infection. • Presents as <span>persistent vaginal discharge, mild or profuse bleeding. • Treatment depends on the etiology. • Retained products of conception may respond to Misoprostol (to aid uterine contraction) or surgical intervention (evacuation of the ute
Flashcard 1414137777420
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
common causes are retained products of conception and pelvic infection. • Presents as persistent vaginal discharge, mild or profuse bleeding. • Treatment depends on the etiology. • Retained products of conception may respond to <span>Misoprostol (to aid uterine contraction) or surgical intervention (evacuation of the uterus). • Pelvic infection (endometritis) responds to antibiotic therapy.<span><body><html>
Flashcard 1414139350284
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
ption and pelvic infection. • Presents as persistent vaginal discharge, mild or profuse bleeding. • Treatment depends on the etiology. • Retained products of conception may respond to Misoprostol (to aid uterine contraction) or <span>surgical intervention (evacuation of the uterus). • Pelvic infection (endometritis) responds to antibiotic therapy.<span><body><html>
Flashcard 1414140923148
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
. • Treatment depends on the etiology. • Retained products of conception may respond to Misoprostol (to aid uterine contraction) or surgical intervention (evacuation of the uterus). • Pelvic infection (endometritis) responds to <span>antibiotic therapy.<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1414143806732
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Delayed post-partum hemorrhage • Bleeding occurring 1 to 2 weeks into the puerperium. • May result from retained products of conception or abnormal placental site involution. • The retained piece of the placenta may become calcified f
Flashcard 1414145379596
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Delayed post-partum hemorrhage • Bleeding occurring 1 to 2 weeks into the puerperium. • May result from retained products of conception or abnormal placental site involution. • The retained piece of the placenta may become calcified forming a placental polyp. • Treatment with ergometrine, misoprostol and Prost
Flashcard 1414146952460
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Delayed post-partum hemorrhage • Bleeding occurring 1 to 2 weeks into the puerperium. • May result from retained products of conception or abnormal placental site involution. • The retained piece of the placenta may become calcified forming a placental polyp. • Treatment with ergometrine, misoprostol and Prostaglandin is conservative and preserves
Flashcard 1414148525324
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
span>Delayed post-partum hemorrhage • Bleeding occurring 1 to 2 weeks into the puerperium. • May result from retained products of conception or abnormal placental site involution. • The retained piece of the placenta may become <span>calcified forming a placental polyp. • Treatment with ergometrine, misoprostol and Prostaglandin is conservative and preserves the uterus. • Surgical treatment with gentle dilatation an
Flashcard 1414150098188
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
rtum hemorrhage • Bleeding occurring 1 to 2 weeks into the puerperium. • May result from retained products of conception or abnormal placental site involution. • The retained piece of the placenta may become calcified forming a <span>placental polyp. • Treatment with ergometrine, misoprostol and Prostaglandin is conservative and preserves the uterus. • Surgical treatment with gentle dilatation and curettage is reserved fo
Flashcard 1414151671052
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
ng 1 to 2 weeks into the puerperium. • May result from retained products of conception or abnormal placental site involution. • The retained piece of the placenta may become calcified forming a placental polyp. • Treatment with <span>ergometrine, misoprostol and Prostaglandin is conservative and preserves the uterus. • Surgical treatment with gentle dilatation and curettage is reserved for severe bleeding or if medical treatment fails. Beware of overzea
Flashcard 1414153243916
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
te involution. • The retained piece of the placenta may become calcified forming a placental polyp. • Treatment with ergometrine, misoprostol and Prostaglandin is conservative and preserves the uterus. • Surgical treatment with <span>gentle dilatation and curettage is reserved for severe bleeding or if medical treatment fails. Beware of overzealous curettage as this may lead uterine synechiae (Asherman’s syndrome).<span><body><html>
Flashcard 1414154816780
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
placenta may become calcified forming a placental polyp. • Treatment with ergometrine, misoprostol and Prostaglandin is conservative and preserves the uterus. • Surgical treatment with gentle dilatation and curettage is reserved for <span>severe bleeding or if medical treatment fails. Beware of overzealous curettage as this may lead uterine synechiae (Asherman’s syndrome).<span><body><html>
Flashcard 1414156389644
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
prostol and Prostaglandin is conservative and preserves the uterus. • Surgical treatment with gentle dilatation and curettage is reserved for severe bleeding or if medical treatment fails. Beware of overzealous curettage as this may lead <span>uterine synechiae (Asherman’s syndrome).<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1414159273228
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Urinary tract changes • During pregnancy, there is physiological retention of water. • Water diuresis occurs after delivery due to the loss of the elevated venous pressure and the loss of the hyperestrogenemia of pregnancy. • Bladder distension can o
Flashcard 1414160846092
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Urinary tract changes • During pregnancy, there is physiological retention of water. • Water diuresis occurs after delivery due to the loss of the elevated venous pressure and the loss of the hyperestrogenemia of pregnancy. • Bladder distension can occur from regional anaesthesia.&
Flashcard 1414162418956
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Urinary tract changes • During pregnancy, there is physiological retention of water. • Water diuresis occurs after delivery due to the loss of the elevated venous pressure and the loss of the hyperestrogenemia of pregnancy. • Bladder distension can occur from regional anaesthesia. • Disposition to urinary tract infection due to bladder distensio
Flashcard 1414163991820
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Urinary tract changes • During pregnancy, there is physiological retention of water. • Water diuresis occurs after delivery due to the loss of the elevated venous pressure and the loss of the hyperestrogenemia of pregnancy. • Bladder distension can occur from regional anaesthesia. • Disposition to urinary tract infection due to bladder distension from regional anesthesia, dilated re
Flashcard 1414165564684
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
n>Urinary tract changes • During pregnancy, there is physiological retention of water. • Water diuresis occurs after delivery due to the loss of the elevated venous pressure and the loss of the hyperestrogenemia of pregnancy. • <span>Bladder distension can occur from regional anaesthesia. • Disposition to urinary tract infection due to bladder distension from regional anesthesia, dilated renal pelvis. • Stress or urge urinar
Flashcard 1414167137548
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
esis occurs after delivery due to the loss of the elevated venous pressure and the loss of the hyperestrogenemia of pregnancy. • Bladder distension can occur from regional anaesthesia. • Disposition to urinary tract infection due to <span>bladder distension from regional anesthesia, dilated renal pelvis. • Stress or urge urinary incontinence is common; more so if there was an instrumental delivery or a prolonged second stage.<span><body><html>
Flashcard 1414168710412
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
the elevated venous pressure and the loss of the hyperestrogenemia of pregnancy. • Bladder distension can occur from regional anaesthesia. • Disposition to urinary tract infection due to bladder distension from regional anesthesia, <span>dilated renal pelvis. • Stress or urge urinary incontinence is common; more so if there was an instrumental delivery or a prolonged second stage.<span><body><html>
Flashcard 1414170283276
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
and the loss of the hyperestrogenemia of pregnancy. • Bladder distension can occur from regional anaesthesia. • Disposition to urinary tract infection due to bladder distension from regional anesthesia, dilated renal pelvis. • <span>Stress or urge urinary incontinence is common; more so if there was an instrumental delivery or a prolonged second stage.<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1414173166860
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Blood and fluid changes • In the puerperium, there is leukocytosis, thrombocytosis, lymphopenia and eosinopenia. • Cardiac volume elevated for the first 48 hrs. • Elevation of plasma fibrinogen. • ESR remains elevated.</bod
Flashcard 1414174739724
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Blood and fluid changes • In the puerperium, there is leukocytosis, thrombocytosis, lymphopenia and eosinopenia. • Cardiac volume elevated for the first 48 hrs. • Elevation of plasma fibrinogen. • ESR remains elevated.
Flashcard 1414176312588
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Blood and fluid changes • In the puerperium, there is leukocytosis, thrombocytosis, lymphopenia and eosinopenia. • Cardiac volume elevated for the first 48 hrs. • Elevation of plasma fibrinogen. • ESR remains elevated.
Flashcard 1414177885452
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Blood and fluid changes • In the puerperium, there is leukocytosis, thrombocytosis, lymphopenia and eosinopenia. • Cardiac volume elevated for the first 48 hrs. • Elevation of plasma fibrinogen. • ESR remains elevated.
Flashcard 1414179458316
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Blood and fluid changes • In the puerperium, there is leukocytosis, thrombocytosis, lymphopenia and eosinopenia. • Cardiac volume elevated for the first 48 hrs. • Elevation of plasma fibrinogen. • ESR remains elevated.
Flashcard 1414181031180
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Blood and fluid changes • In the puerperium, there is leukocytosis, thrombocytosis, lymphopenia and eosinopenia. • Cardiac volume elevated for the first 48 hrs. • Elevation of plasma fibrinogen. • ESR remains elevated.
Flashcard 1414182604044
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
><head>Blood and fluid changes • In the puerperium, there is leukocytosis, thrombocytosis, lymphopenia and eosinopenia. • Cardiac volume elevated for the first 48 hrs. • Elevation of plasma fibrinogen. • ESR remains elevated.<html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1414186011916
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Need to monitor volume of blood loss objectively during delivery because body will suddenly decompensate later
Flashcard 1414187584780
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Need to monitor volume of blood loss objectively during delivery because body will suddenly decompensate later
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1414190730508
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
NORMAL POSTPARTUM CARE Following Spontaneous Vaginal Delivery (SVD) and Caesarean Section: • Commence regular diet as soon as possible, as long as there is no contraindication to doing so. • Resume activity. • Regular perineal cleansing 2 to 3 times daily or following bowel movements and urination. • Ice
Flashcard 1414192303372
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
ad><head>NORMAL POSTPARTUM CARE Following Spontaneous Vaginal Delivery (SVD) and Caesarean Section: • Commence regular diet as soon as possible, as long as there is no contraindication to doing so. • Resume activity. • Regular perineal cleansing 2 to 3 times daily or following bowel movements and urination. • Ice packs to perineum if painful. • Sitz bath with warm water if perineal l
Flashcard 1414193876236
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
M CARE Following Spontaneous Vaginal Delivery (SVD) and Caesarean Section: • Commence regular diet as soon as possible, as long as there is no contraindication to doing so. • Resume activity. • Regular perineal cleansing <span>2 to 3 times daily or following bowel movements and urination. • Ice packs to perineum if painful. • Sitz bath with warm water if perineal laceration or episiotomy. • Regular an
Flashcard 1414195449100
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
us Vaginal Delivery (SVD) and Caesarean Section: • Commence regular diet as soon as possible, as long as there is no contraindication to doing so. • Resume activity. • Regular perineal cleansing 2 to 3 times daily or following <span>bowel movements and urination. • Ice packs to perineum if painful. • Sitz bath with warm water if perineal laceration or episiotomy. • Regular analgesia, stool softener (may wish to give self-medicati
Flashcard 1414197021964
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
n Section: • Commence regular diet as soon as possible, as long as there is no contraindication to doing so. • Resume activity. • Regular perineal cleansing 2 to 3 times daily or following bowel movements and urination. • <span>Ice packs to perineum if painful. • Sitz bath with warm water if perineal laceration or episiotomy. • Regular analgesia, stool softener (may wish to give self-medication package so that
Flashcard 1414198594828
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
as soon as possible, as long as there is no contraindication to doing so. • Resume activity. • Regular perineal cleansing 2 to 3 times daily or following bowel movements and urination. • Ice packs to perineum if painful. • <span>Sitz bath with warm water if perineal laceration or episiotomy. • Regular analgesia, stool softener (may wish to give self-medication package so that the patient can administer the drug when necessary).
Flashcard 1414200167692
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
o. • Resume activity. • Regular perineal cleansing 2 to 3 times daily or following bowel movements and urination. • Ice packs to perineum if painful. • Sitz bath with warm water if perineal laceration or episiotomy. • <span>Regular analgesia, stool softener (may wish to give self-medication package so that the patient can administer the drug when necessary). • Give Rhogam if Rhesus negative and unsensitized. • Support exclusive b
Flashcard 1414204099852
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
nful. • Sitz bath with warm water if perineal laceration or episiotomy. • Regular analgesia, stool softener (may wish to give self-medication package so that the patient can administer the drug when necessary). • Give Rhogam if <span>Rhesus negative and unsensitized. • Support exclusive breastfeeding or the use of a breast binder for women who decide against breastfeeding. • Provide breastfeeding support at home if difficulty with breastfe
Flashcard 1414205672716
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
on or episiotomy. • Regular analgesia, stool softener (may wish to give self-medication package so that the patient can administer the drug when necessary). • Give Rhogam if Rhesus negative and unsensitized. • Support exclusive <span>breastfeeding or the use of a breast binder for women who decide against breastfeeding. • Provide breastfeeding support at home if difficulty with breastfeeding. • Give MMR to women who are
Flashcard 1414207245580
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
m if Rhesus negative and unsensitized. • Support exclusive breastfeeding or the use of a breast binder for women who decide against breastfeeding. • Provide breastfeeding support at home if difficulty with breastfeeding. • Give <span>MMR to women who are not immune to rubella (instruct patient to avoid getting pregnant for 3 months). • Discuss contraception ideally upon discharge home and be prepared to discuss it
Flashcard 1414208818444
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
ed. • Support exclusive breastfeeding or the use of a breast binder for women who decide against breastfeeding. • Provide breastfeeding support at home if difficulty with breastfeeding. • Give MMR to women who are not immune to <span>rubella (instruct patient to avoid getting pregnant for 3 months). • Discuss contraception ideally upon discharge home and be prepared to discuss it again at the six week post-partum check
Flashcard 1414210391308
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
a breast binder for women who decide against breastfeeding. • Provide breastfeeding support at home if difficulty with breastfeeding. • Give MMR to women who are not immune to rubella (instruct patient to avoid getting pregnant for <span>3 months). • Discuss contraception ideally upon discharge home and be prepared to discuss it again at the six week post-partum check. • Emotional and social support: Encourage p
Flashcard 1414211964172
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
eeding. • Provide breastfeeding support at home if difficulty with breastfeeding. • Give MMR to women who are not immune to rubella (instruct patient to avoid getting pregnant for 3 months). • Discuss contraception ideally upon <span>discharge home and be prepared to discuss it again at the six week post-partum check. • Emotional and social support: Encourage patients to have adequate rest, spousal time off/paternal leave; di
Flashcard 1414213537036
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
fficulty with breastfeeding. • Give MMR to women who are not immune to rubella (instruct patient to avoid getting pregnant for 3 months). • Discuss contraception ideally upon discharge home and be prepared to discuss it again at the <span>six week post-partum check. • Emotional and social support: Encourage patients to have adequate rest, spousal time off/paternal leave; discuss signs and symptoms of postpartum mood changes.<span></bod
Flashcard 1414215109900
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
n ideally upon discharge home and be prepared to discuss it again at the six week post-partum check. • Emotional and social support: Encourage patients to have adequate rest, spousal time off/paternal leave; discuss signs and symptoms of <span>postpartum mood changes.<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1414217993484
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1414220090636
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1414222712076
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Causes of postpartum fever: • “After pains” ---• Common the first 3 days, due to uterine contractions. Common during breastfeeding. ---• Encourage simple analgesia.
Flashcard 1414224284940
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Causes of postpartum fever: • “After pains” ---• Common the first 3 days, due to uterine contractions. Common during breastfeeding. ---• Encourage simple analgesia.
Flashcard 1414225857804
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Causes of postpartum fever: • “After pains” ---• Common the first 3 days, due to uterine contractions. Common during breastfeeding. ---• Encourage simple analgesia.
Flashcard 1414227430668
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Causes of postpartum fever: • “After pains” ---• Common the first 3 days, due to uterine contractions. Common during breastfeeding. ---• Encourage simple analgesia.
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1414230576396
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Etiology of postpartum fever (B-5W): • Wind (atelectasis) • Water (UTI) • Wound (Gram positive/negative aerobes or anaerobes) check CS site and episiotomy site • Walking (DVT, Pelvic Thrombophlebitis) • Womb (GAS, endometri
Flashcard 1414232149260
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Etiology of postpartum fever (B-5W): • Wind (atelectasis) • Water (UTI) • Wound (Gram positive/negative aerobes or anaerobes) check CS site and episiotomy site • Walking (DVT, Pelvic Thrombophlebitis) • Womb (GAS, endometritis) • Breast
Flashcard 1414233722124
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Etiology of postpartum fever (B-5W): • Wind (atelectasis) • Water (UTI) • Wound (Gram positive/negative aerobes or anaerobes) check CS site and episiotomy site • Walking (DVT, Pelvic Thrombophlebitis) • Womb (GAS, endometritis) • Breast (engorgement, mastitis)
Flashcard 1414235294988
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Etiology of postpartum fever (B-5W): • Wind (atelectasis) • Water (UTI) • Wound (Gram positive/negative aerobes or anaerobes) check CS site and episiotomy site • Walking (DVT, Pelvic Thrombophlebitis) • Womb (GAS, endometritis) • Breast (engorgement, mastitis)
Flashcard 1414236867852
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
dy>Etiology of postpartum fever (B-5W): • Wind (atelectasis) • Water (UTI) • Wound (Gram positive/negative aerobes or anaerobes) check CS site and episiotomy site • Walking (DVT, Pelvic Thrombophlebitis) • Womb (GAS, endometritis) • Breast (engorgement, mastitis)<body><html>
Flashcard 1414238440716
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
artum fever (B-5W): • Wind (atelectasis) • Water (UTI) • Wound (Gram positive/negative aerobes or anaerobes) check CS site and episiotomy site • Walking (DVT, Pelvic Thrombophlebitis) • Womb (GAS, endometritis) • <span>Breast (engorgement, mastitis)<span><body><html>
Flashcard 1414240013580
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1414241848588
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1414244994316
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Infected Episiotomy -keep open, frequent sitz bath, keep dry, consider oral antibiotics if indurated, painful with purulent discharge. -Avoid re-suturing, as healing is by secondary intention.</bod
Flashcard 1414246567180
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Infected Episiotomy -keep open, frequent sitz bath, keep dry, consider oral antibiotics if indurated, painful with purulent discharge. -Avoid re-suturing, as healing is by secondary intention.
Flashcard 1414248140044
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Infected Episiotomy -keep open, frequent sitz bath, keep dry, consider oral antibiotics if indurated, painful with purulent discharge. -Avoid re-suturing, as healing is by secondary intention.
Flashcard 1414249712908
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Infected Episiotomy -keep open, frequent sitz bath, keep dry, consider oral antibiotics if indurated, painful with purulent discharge. -Avoid re-suturing, as healing is by secondary intention.
Flashcard 1414251285772
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Infected Episiotomy -keep open, frequent sitz bath, keep dry, consider oral antibiotics if indurated, painful with purulent discharge. -Avoid re-suturing, as healing is by secondary intention.
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1414254169356
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Abdominal wound infection postpartum: -if superficial, treat with oral antibiotics -if deep, may need to admit, open the incision and treat as appropriate
Flashcard 1414255742220
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Abdominal wound infection postpartum: -if superficial, treat with oral antibiotics -if deep, may need to admit, open the incision and treat as appropriate
Flashcard 1414257315084
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1414259150092
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1414260985100
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1414262820108
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1414265965836
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
SEXUAL ACTIVITY • Can be resumed within 4-6 weeks of childbirth. • Dyspareunia can be treated with lubricants or topical estrogens.
Flashcard 1414267538700
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
SEXUAL ACTIVITY • Can be resumed within 4-6 weeks of childbirth. • Dyspareunia can be treated with lubricants or topical estrogens.
Flashcard 1414269111564
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
SEXUAL ACTIVITY • Can be resumed within 4-6 weeks of childbirth. • Dyspareunia can be treated with lubricants or topical estrogens.
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1414271995148
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
CONTRACEPTION • Ovulation can occur within 4 to 6 weeks of delivery in women who are not breastfeeding. • Hormonal preparation are safe in women breastfeeding (secretion in breast milk is minimal). • Milk production can be af
Flashcard 1414273568012
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
CONTRACEPTION • Ovulation can occur within 4 to 6 weeks of delivery in women who are not breastfeeding. • Hormonal preparation are safe in women breastfeeding (secretion in breast milk is minimal). • Milk production can be affected in the early postpartum period with the use of combined contraceptive pill. • Progesterone only pill (POP)/Progesterone only IUD are safe a
Flashcard 1414275140876
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
o 6 weeks of delivery in women who are not breastfeeding. • Hormonal preparation are safe in women breastfeeding (secretion in breast milk is minimal). • Milk production can be affected in the early postpartum period with the use of <span>combined contraceptive pill. • Progesterone only pill (POP)/Progesterone only IUD are safe and can be started within 2 weeks of delivery. • The combined oral contraceptive pill or POP can be commenced wi
Flashcard 1414276713740
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
re not breastfeeding. • Hormonal preparation are safe in women breastfeeding (secretion in breast milk is minimal). • Milk production can be affected in the early postpartum period with the use of combined contraceptive pill. • <span>Progesterone only pill (POP)/Progesterone only IUD are safe and can be started within 2 weeks of delivery. • The combined oral contraceptive pill or POP can be commenced within 1-2 weeks in women who are not breastfeeding. • D
Flashcard 1414278286604
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
retion in breast milk is minimal). • Milk production can be affected in the early postpartum period with the use of combined contraceptive pill. • Progesterone only pill (POP)/Progesterone only IUD are safe and can be started within <span>2 weeks of delivery. • The combined oral contraceptive pill or POP can be commenced within 1-2 weeks in women who are not breastfeeding. • Depo-Provera 150mg IM can be started a
Flashcard 1414279859468
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
). • Milk production can be affected in the early postpartum period with the use of combined contraceptive pill. • Progesterone only pill (POP)/Progesterone only IUD are safe and can be started within 2 weeks of delivery. • The <span>combined oral contraceptive pill or POP can be commenced within 1-2 weeks in women who are not breastfeeding. • Depo-Provera 150mg IM can be started after delivery. • The intrauterine device can be inserted immediat
Flashcard 1414281432332
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
m period with the use of combined contraceptive pill. • Progesterone only pill (POP)/Progesterone only IUD are safe and can be started within 2 weeks of delivery. • The combined oral contraceptive pill or POP can be commenced within <span>1-2 weeks in women who are not breastfeeding. • Depo-Provera 150mg IM can be started after delivery. • The intrauterine device can be inserted immediately (within 10 minutes) afte
Flashcard 1414283005196
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
• Progesterone only pill (POP)/Progesterone only IUD are safe and can be started within 2 weeks of delivery. • The combined oral contraceptive pill or POP can be commenced within 1-2 weeks in women who are not breastfeeding. • <span>Depo-Provera 150mg IM can be started after delivery. • The intrauterine device can be inserted immediately (within 10 minutes) after the delivery of the placenta, because of the high risk of expulsion,
Flashcard 1414284578060
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
s of delivery. • The combined oral contraceptive pill or POP can be commenced within 1-2 weeks in women who are not breastfeeding. • Depo-Provera 150mg IM can be started after delivery. • The intrauterine device can be inserted <span>immediately (within 10 minutes) after the delivery of the placenta, because of the high risk of expulsion, it is typically inserted after 6 weeks. • Tubal sterilization can be performed during Caesarean section,
Flashcard 1414286150924
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
3; • Depo-Provera 150mg IM can be started after delivery. • The intrauterine device can be inserted immediately (within 10 minutes) after the delivery of the placenta, because of the high risk of expulsion, it is typically inserted after <span>6 weeks. • Tubal sterilization can be performed during Caesarean section, immediately postpartum after a vaginal delivery or as an interval procedure.<span><body><html>
Flashcard 1414287723788
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
3; • The intrauterine device can be inserted immediately (within 10 minutes) after the delivery of the placenta, because of the high risk of expulsion, it is typically inserted after 6 weeks. • Tubal sterilization can be performed during <span>Caesarean section, immediately postpartum after a vaginal delivery or as an interval procedure.<span><body><html>
Flashcard 1414289296652
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
ne device can be inserted immediately (within 10 minutes) after the delivery of the placenta, because of the high risk of expulsion, it is typically inserted after 6 weeks. • Tubal sterilization can be performed during Caesarean section, <span>immediately postpartum after a vaginal delivery or as an interval procedure.<span><body><html>
Flashcard 1414290869516
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
es) after the delivery of the placenta, because of the high risk of expulsion, it is typically inserted after 6 weeks. • Tubal sterilization can be performed during Caesarean section, immediately postpartum after a vaginal delivery or as <span>an interval procedure.<span><body><html>
Flashcard 1414293753100
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Endometritis - postpartum complication: • Infection of the uterine myometrium and parametrium. • A common cause of postpartum febrile morbidity. • Uncommon in uncomplicated vaginal deliveries. • Signs and symptoms: fever +/- chills, abdominal pain, abnormal bleedin
Flashcard 1414295325964
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Endometritis - postpartum complication: • Infection of the uterine myometrium and parametrium. • A common cause of postpartum febrile morbidity. • Uncommon in uncomplicated vaginal deliveries. • Signs and symptoms: fever +/- chills, abdominal pain, abnormal bleeding or foul smelling lochia. • Examination revealed
Flashcard 1414296898828
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Endometritis - postpartum complication: • Infection of the uterine myometrium and parametrium. • A common cause of postpartum febrile morbidity. • Uncommon in uncomplicated vaginal deliveries. • Signs and symptoms: fever +/- chills, abdominal pain, abnormal bleeding or foul smelling lochia. • Examination revealed a tender abdomen and uterus, offensive discharge.
Flashcard 1414298471692
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
n>Endometritis - postpartum complication: • Infection of the uterine myometrium and parametrium. • A common cause of postpartum febrile morbidity. • Uncommon in uncomplicated vaginal deliveries. • Signs and symptoms: fever +/- chills, abdominal pain, abnormal bleeding or foul smelling lochia. • Examination revealed a tender abdomen and uterus, offensive discharge. • Predisposing factors: prolonged rupture of membranes and labour, multiple vaginal examinations, use
Flashcard 1414300044556
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
• A common cause of postpartum febrile morbidity. • Uncommon in uncomplicated vaginal deliveries. • Signs and symptoms: fever +/- chills, abdominal pain, abnormal bleeding or foul smelling lochia. • Examination revealed a <span>tender abdomen and uterus, offensive discharge. • Predisposing factors: prolonged rupture of membranes and labour, multiple vaginal examinations, use of internal fetal monitoring, intrapartum chorioamnionitis, caesarean section
Flashcard 1414301617420
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
complicated vaginal deliveries. • Signs and symptoms: fever +/- chills, abdominal pain, abnormal bleeding or foul smelling lochia. • Examination revealed a tender abdomen and uterus, offensive discharge. • Predisposing factors: <span>prolonged rupture of membranes and labour, multiple vaginal examinations, use of internal fetal monitoring, intrapartum chorioamnionitis, caesarean section.<span><body><html>
Flashcard 1414303190284
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
s and symptoms: fever +/- chills, abdominal pain, abnormal bleeding or foul smelling lochia. • Examination revealed a tender abdomen and uterus, offensive discharge. • Predisposing factors: prolonged rupture of membranes and labour, <span>multiple vaginal examinations, use of internal fetal monitoring, intrapartum chorioamnionitis, caesarean section.<span><body><html>
Flashcard 1414304763148
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
s, abdominal pain, abnormal bleeding or foul smelling lochia. • Examination revealed a tender abdomen and uterus, offensive discharge. • Predisposing factors: prolonged rupture of membranes and labour, multiple vaginal examinations, <span>use of internal fetal monitoring, intrapartum chorioamnionitis, caesarean section.<span><body><html>
Flashcard 1414306336012
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
ng or foul smelling lochia. • Examination revealed a tender abdomen and uterus, offensive discharge. • Predisposing factors: prolonged rupture of membranes and labour, multiple vaginal examinations, use of internal fetal monitoring, <span>intrapartum chorioamnionitis, caesarean section.<span><body><html>
Flashcard 1414307908876
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
3; • Examination revealed a tender abdomen and uterus, offensive discharge. • Predisposing factors: prolonged rupture of membranes and labour, multiple vaginal examinations, use of internal fetal monitoring, intrapartum chorioamnionitis, <span>caesarean section.<span><body><html>
Flashcard 1414310792460
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
postpartum endometritis investigations: - complete blood count (may show neutrophilia), vaginal, blood and urine cultures.
Flashcard 1414312365324
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
postpartum endometritis investigations: - complete blood count (may show neutrophilia), vaginal, blood and urine cultures.
Flashcard 1414313938188
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1414317083916
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Severe postpartum endometritis tx: Sick patients, post abdominal deliveries, treat with Intravenous therapy- Clindamycin IV 900mg every 8 hours + Gentamicin IV 1.5mg/kg every 8 hours or Extended interval dosing of Gentamicin 5mg/kg every 24 hours. The extended
Flashcard 1414318656780
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Severe postpartum endometritis tx: Sick patients, post abdominal deliveries, treat with Intravenous therapy- Clindamycin IV 900mg every 8 hours + Gentamicin IV 1.5mg/kg every 8 hours or Extended interval dosing of Gentamicin 5mg/kg every 24 hours. The extended dosing is convenient and does not require Gen
Flashcard 1414321802508
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Severe postpartum endometritis tx: Sick patients, post abdominal deliveries, treat with Intravenous therapy- Clindamycin IV 900mg every 8 hours + Gentamicin IV 1.5mg/kg every 8 hours or Extended interval dosing of Gentamicin 5mg/kg every 24 hours. The extended dosing is convenient and does not require Gentamicin levels. <
Flashcard 1414323375372
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Severe postpartum endometritis tx: Sick patients, post abdominal deliveries, treat with Intravenous therapy- Clindamycin IV 900mg every 8 hours + Gentamicin IV 1.5mg/kg every 8 hours or Extended interval dosing of Gentamicin 5mg/kg every 24 hours. The extended dosing is convenient and does not require Gentamicin levels.
Flashcard 1414327569676
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Severe postpartum endometritis tx: Sick patients, post abdominal deliveries, treat with Intravenous therapy- Clindamycin IV 900mg every 8 hours + Gentamicin IV 1.5mg/kg every 8 hours or Extended interval dosing of Gentamicin 5mg/kg every 24 hours. The extended dosing is convenient and does not require Gentamicin levels.
Flashcard 1414329142540
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Severe postpartum endometritis tx: Sick patients, post abdominal deliveries, treat with Intravenous therapy- Clindamycin IV 900mg every 8 hours + Gentamicin IV 1.5mg/kg every 8 hours or Extended interval dosing of Gentamicin 5mg/kg every 24 hours. The extended dosing is convenient and does not require Gentamicin levels.
Flashcard 1414330715404
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Severe postpartum endometritis tx: Sick patients, post abdominal deliveries, treat with Intravenous therapy- Clindamycin IV 900mg every 8 hours + Gentamicin IV 1.5mg/kg every 8 hours or Extended interval dosing of Gentamicin 5mg/kg every <span>24 hours. The extended dosing is convenient and does not require Gentamicin levels. <span><body><html>
Flashcard 1414332288268
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1414335433996
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Persistent postpartum fever: Refers to a lack of improvement or deterioration in clinical status after 48 hours of treatment. Re-evaluate the patient, perform a full physical exam and consider imaging like Ultrasound to exclude retained products of conception (RPOC), Consultation to Infectious disease te
Flashcard 1414337006860
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
span>Persistent postpartum fever: Refers to a lack of improvement or deterioration in clinical status after 48 hours of treatment. Re-evaluate the patient, perform a full physical exam and consider imaging like Ultrasound to exclude <span>retained products of conception (RPOC), Consultation to Infectious disease team (ID team). Consider other causes like Infected hematoma, Pelvic abscess, Pelvic cellulitis, Wound infection, Septic pelvic thrombophlebitis
Flashcard 1414338579724
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
f treatment. Re-evaluate the patient, perform a full physical exam and consider imaging like Ultrasound to exclude retained products of conception (RPOC), Consultation to Infectious disease team (ID team). Consider other causes like <span>Infected hematoma, Pelvic abscess, Pelvic cellulitis, Wound infection, Septic pelvic thrombophlebitis, ovarian vein thrombosis. Treatment: consider antibiotics changes (consult ID team); consider gentle curettage if there is RPOC to remove necrotic tissue. “Gentle” to prevent uterine scarring/ Asherman’s
Flashcard 1414340152588
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
c cellulitis, Wound infection, Septic pelvic thrombophlebitis, ovarian vein thrombosis. Treatment: consider antibiotics changes (consult ID team); consider gentle curettage if there is RPOC to remove necrotic tissue. “Gentle” to prevent <span>uterine scarring/ Asherman’s syndrome. <span><body><html>
Flashcard 1414341725452
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
POC), Consultation to Infectious disease team (ID team). Consider other causes like Infected hematoma, Pelvic abscess, Pelvic cellulitis, Wound infection, Septic pelvic thrombophlebitis, ovarian vein thrombosis. Treatment: consider <span>antibiotics changes (consult ID team); consider gentle curettage if there is RPOC to remove necrotic tissue. “Gentle” to prevent uterine scarring/ Asherman’s syndrome. <span><body><html>
Flashcard 1414343298316
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
ected hematoma, Pelvic abscess, Pelvic cellulitis, Wound infection, Septic pelvic thrombophlebitis, ovarian vein thrombosis. Treatment: consider antibiotics changes (consult ID team); consider gentle curettage if there is RPOC to remove <span>necrotic tissue. “Gentle” to prevent uterine scarring/ Asherman’s syndrome. <span><body><html>
Flashcard 1414344871180
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1414351162636
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
postpartum hemorrhage: Can be classified as early (within 24 hours of delivery) and late (after 24 hours but before 6 weeks)
Flashcard 1414353259788
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
postpartum hemorrhage: Can be classified as early (within 24 hours of delivery) and late (after 24 hours but before 6 weeks)
Flashcard 1414354832652
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1414356667660
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1414359026956
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1414362172684
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Prevention of PPH 1 . Administer oxytocin routinely after delivery 2 . Clamp and cut cord when baby delivered (delay clamping by 60 sec if <37wks GA) 3 . Palpate uterine fundus and confirm that uterus is contracting 4 . Keep tension o
Flashcard 1414363745548
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Prevention of PPH 1 . Administer oxytocin routinely after delivery 2 . Clamp and cut cord when baby delivered (delay clamping by 60 sec if <37wks GA) 3 . Palpate uterine fundus and confirm that uterus is contracting 4 . Keep tension on cord pulling gently while applying suprapubic counter-traction on uterus with other hand.
Flashcard 1414365318412
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Prevention of PPH 1 . Administer oxytocin routinely after delivery 2 . Clamp and cut cord when baby delivered (delay clamping by 60 sec if <37wks GA) 3 . Palpate uterine fundus and confirm that uterus is contracting 4 . Keep tension on cord pulling gently while applying suprapubic counter-traction on uterus with other hand. Digital exam along the cord to determine whether the placenta is at th
Flashcard 1414366891276
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
revention of PPH 1 . Administer oxytocin routinely after delivery 2 . Clamp and cut cord when baby delivered (delay clamping by 60 sec if <37wks GA) 3 . Palpate uterine fundus and confirm that uterus is contracting 4 . <span>Keep tension on cord pulling gently while applying suprapubic counter-traction on uterus with other hand. Digital exam along the cord to determine whether the placenta is at the cervix. Pulling hard on cord may cause cord to avulse. Gentle traction with a relaxed uterus can cause uter
Flashcard 1414368464140
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
hand. Digital exam along the cord to determine whether the placenta is at the cervix. Pulling hard on cord may cause cord to avulse. Gentle traction with a relaxed uterus can cause uterine inversion. 5 . If placenta not delivered in <span>15 minutes, use oxytocin infusion 6 . Once placenta delivered, assess fundus to ensure it is well contracted 7 . Inspect placenta and membranes for completeness 8 . Examine
Flashcard 1414370037004
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
am along the cord to determine whether the placenta is at the cervix. Pulling hard on cord may cause cord to avulse. Gentle traction with a relaxed uterus can cause uterine inversion. 5 . If placenta not delivered in 15 minutes, use <span>oxytocin infusion 6 . Once placenta delivered, assess fundus to ensure it is well contracted 7 . Inspect placenta and membranes for completeness 8 . Examine external genitalia and internal
Flashcard 1414371609868
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
he cervix. Pulling hard on cord may cause cord to avulse. Gentle traction with a relaxed uterus can cause uterine inversion. 5 . If placenta not delivered in 15 minutes, use oxytocin infusion 6 . Once placenta delivered, assess <span>fundus to ensure it is well contracted 7 . Inspect placenta and membranes for completeness 8 . Examine external genitalia and internal genital tract for lacerations, hematomas.<span><body><html>
Flashcard 1414373182732
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
a relaxed uterus can cause uterine inversion. 5 . If placenta not delivered in 15 minutes, use oxytocin infusion 6 . Once placenta delivered, assess fundus to ensure it is well contracted 7 . Inspect placenta and membranes for <span>completeness 8 . Examine external genitalia and internal genital tract for lacerations, hematomas.<span><body><html>
Flashcard 1414374755596
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
d in 15 minutes, use oxytocin infusion 6 . Once placenta delivered, assess fundus to ensure it is well contracted 7 . Inspect placenta and membranes for completeness 8 . Examine external genitalia and internal genital tract for <span>lacerations, hematomas.<span><body><html>
Flashcard 1414377639180
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
8 Steps to PPH management: 1. ABCs 2. get help 3. assess fundus 4. exam genital tract & placenta, + uterine exploration 5. empty bladder 6. drug therapy 7. consider alternative procedure
Flashcard 1414379212044
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
8 Steps to PPH management: 1. ABCs 2. get help 3. assess fundus 4. exam genital tract & placenta, + uterine exploration 5. empty bladder 6. drug therapy 7. consider alternative procedures 8. if coag
Flashcard 1414380784908
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
8 Steps to PPH management: 1. ABCs 2. get help 3. assess fundus 4. exam genital tract & placenta, + uterine exploration 5. empty bladder 6. drug therapy 7. consider alternative procedures 8. if coagulopathy
Flashcard 1414382357772
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
8 Steps to PPH management: 1. ABCs 2. get help 3. assess fundus 4. exam genital tract & placenta, + uterine exploration 5. empty bladder 6. drug therapy 7. consider alternative procedures 8. if coagulopathy
Flashcard 1414383930636
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
8 Steps to PPH management: 1. ABCs 2. get help 3. assess fundus 4. exam genital tract & placenta, + uterine exploration 5. empty bladder 6. drug therapy 7. consider alternative procedures 8. if coagulopathy
Flashcard 1414385503500
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
8 Steps to PPH management: 1. ABCs 2. get help 3. assess fundus 4. exam genital tract & placenta, + uterine exploration 5. empty bladder 6. drug therapy 7. consider alternative procedures 8. if coagulopathy
Flashcard 1414387076364
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
8 Steps to PPH management: 1. ABCs 2. get help 3. assess fundus 4. exam genital tract & placenta, + uterine exploration 5. empty bladder 6. drug therapy 7. consider alternative procedures 8. if coagulopathy
Flashcard 1414388649228
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
n>8 Steps to PPH management: 1. ABCs 2. get help 3. assess fundus 4. exam genital tract & placenta, + uterine exploration 5. empty bladder 6. drug therapy 7. consider alternative procedures 8. if coagulopathy<span><body><html>
Flashcard 1414392057100
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Management of PPH - ABCs: • Talk to and observe your patient • Monitor vital signs • Commence at least one large bore IV (16 gauge or larger) • Run IV crystalloid solution wide open • Obtain a CBC, cross-match and do coagulati
Flashcard 1414393629964
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Management of PPH - ABCs: • Talk to and observe your patient • Monitor vital signs • Commence at least one large bore IV (16 gauge or larger) • Run IV crystalloid solution wide open • Obtain a CBC, cross-match and do coagulation studies</b
Flashcard 1414395202828
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Management of PPH - ABCs: • Talk to and observe your patient • Monitor vital signs • Commence at least one large bore IV (16 gauge or larger) • Run IV crystalloid solution wide open • Obtain a CBC, cross-match and do coagulation studies
Flashcard 1414396775692
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Management of PPH - ABCs: • Talk to and observe your patient • Monitor vital signs • Commence at least one large bore IV (16 gauge or larger) • Run IV crystalloid solution wide open • Obtain a CBC, cross-match and do coagulation studies
Flashcard 1414398348556
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
ml>Management of PPH - ABCs: • Talk to and observe your patient • Monitor vital signs • Commence at least one large bore IV (16 gauge or larger) • Run IV crystalloid solution wide open • Obtain a CBC, cross-match and do coagulation studies<html>
Flashcard 1414400707852
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
PPH management - get help: • Get additional personnel to manage resuscitation • Notify lab of potential need for massive transfusion
Flashcard 1414402280716
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
PPH management - get help: • Get additional personnel to manage resuscitation • Notify lab of potential need for massive transfusion
Flashcard 1414405164300
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
PPH management - assess fundus : if boggy, do bimanual massage: uterus massaged between a hand in vagina against the cervix and a hand on the fundus. Explore uterine cavity at this time to rule out retained products, uterine inversion or uterine ru
Flashcard 1414406737164
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
PPH management - assess fundus : if boggy, do bimanual massage: uterus massaged between a hand in vagina against the cervix and a hand on the fundus. Explore uterine cavity at this time to rule out retained products, uterine inversion or uterine rupture if analgesia allows.
Flashcard 1414408310028
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
PPH management - assess fundus : if boggy, do bimanual massage: uterus massaged between a hand in vagina against the cervix and a hand on the fundus. Explore uterine cavity at this time to rule out retained products, uterine inversion or uterine rupture if analgesia allows.
Flashcard 1414411193612
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Management of PPH - step 4: Examine the genital tract for injury, placenta for completeness, and do manual uterine exploration to rule out retained products
Flashcard 1414412766476
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Management of PPH - step 4: Examine the genital tract for injury, placenta for completeness, and do manual uterine exploration to rule out retained products
Flashcard 1414414339340
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Management of PPH - step 4: Examine the genital tract for injury, placenta for completeness, and do manual uterine exploration to rule out retained products
Flashcard 1414417222924
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
PPH management - empty bladder: may insert Foley catheter to keep bladder empty (which helps keep uterus contracted) and monitor urine output
Flashcard 1414418795788
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
PPH management - empty bladder: may insert Foley catheter to keep bladder empty (which helps keep uterus contracted) and monitor urine output
Flashcard 1414422990092
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
PPH management - alternative procedures: • Intra-uterine balloon (Bakri balloon) • Uterine vessel ligation • Internal iliac artery ligation • Uterine suturing techniques • Hysterectomy • Bilateral uterine/internal iliac artery ligation
Flashcard 1414424562956
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
PPH management - alternative procedures: • Intra-uterine balloon (Bakri balloon) • Uterine vessel ligation • Internal iliac artery ligation • Uterine suturing techniques • Hysterectomy • Bilateral uterine/internal iliac artery ligation
Flashcard 1414426135820
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
PPH management - alternative procedures: • Intra-uterine balloon (Bakri balloon) • Uterine vessel ligation • Internal iliac artery ligation • Uterine suturing techniques • Hysterectomy • Bilateral uterine/internal iliac artery ligation
Flashcard 1414427708684
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
PPH management - alternative procedures: • Intra-uterine balloon (Bakri balloon) • Uterine vessel ligation • Internal iliac artery ligation • Uterine suturing techniques • Hysterectomy • Bilateral uterine/internal iliac artery ligation
Flashcard 1414429281548
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
PPH management - alternative procedures: • Intra-uterine balloon (Bakri balloon) • Uterine vessel ligation • Internal iliac artery ligation • Uterine suturing techniques • Hysterectomy • Bilateral uterine/internal iliac artery ligation
Flashcard 1414430854412
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
><head>PPH management - alternative procedures: • Intra-uterine balloon (Bakri balloon) • Uterine vessel ligation • Internal iliac artery ligation • Uterine suturing techniques • Hysterectomy • Bilateral uterine/internal iliac artery ligation<html>
Flashcard 1414434524428
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
PPH management - coagulopathy: • FFP (fresh frozen plasma) • Cryoprecipitate • Platelets • Packed red blood cells
Flashcard 1414436097292
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
PPH management - coagulopathy: • FFP (fresh frozen plasma) • Cryoprecipitate • Platelets • Packed red blood cells
Flashcard 1414437670156
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
PPH management - coagulopathy: • FFP (fresh frozen plasma) • Cryoprecipitate • Platelets • Packed red blood cells
Flashcard 1414439243020
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
PPH management - coagulopathy: • FFP (fresh frozen plasma) • Cryoprecipitate • Platelets • Packed red blood cells
Flashcard 1414440815884
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
PPH management - drug therapy: • Oxytocin ---• 5 units IV bolus ---• 20-40 units/250mL in crystalloid ---• 10 units IM if CV collapse or no IV access • Carbetocin (long-acting oxytocin) ---• 100ug IV/IM • Hema
Flashcard 1414442388748
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
PPH management - drug therapy: • Oxytocin ---• 5 units IV bolus ---• 20-40 units/250mL in crystalloid ---• 10 units IM if CV collapse or no IV access • Carbetocin (long-acting oxytocin) ---• 100ug IV/IM • Hemabate (Carboprost/15-Methyl Pros
Flashcard 1414443961612
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
PPH management - drug therapy: • Oxytocin ---• 5 units IV bolus ---• 20-40 units/250mL in crystalloid ---• 10 units IM if CV collapse or no IV access • Carbetocin (long-acting oxytocin) ---• 100ug IV/IM • Hemabate (Carboprost/15-Methyl Prostaglandin F2a) ---• 250 ug IM or in
Flashcard 1414445534476
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
gonovine maleate ---• 0.25 mg IM/0.125 mg IV ---• Repeat every 5 mins as needed ---• Maximum 5 doses ---• Hypertension and some medications (eg proteases) are a contraindication • Misoprostol (off-label use) ---• <span>600-800 ug po/sl (faster onset) or pr/pv ---• Side effect: Pyrexia if >600ug given • Tranexamic Acid (cyklokapron)—antifibrinolytic ---• 1g IV<span><body><html>
Flashcard 1414447107340
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
mins as needed ---• Maximum 5 doses ---• Hypertension and some medications (eg proteases) are a contraindication • Misoprostol (off-label use) ---• 600-800 ug po/sl (faster onset) or pr/pv ---• Side effect: Pyrexia if <span>>600ug given • Tranexamic Acid (cyklokapron)—antifibrinolytic ---• 1g IV<span><body><html>
Flashcard 1414448680204
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
boprost/15-Methyl Prostaglandin F2a) ---• 250 ug IM or intramyometrial; repeat every 15 min as needed ---• Maximum cumulative dose 2 mg (8 doses) ---• Asthma a relative contraindication • Methylergonovine maleate ---• <span>0.25 mg IM/0.125 mg IV ---• Repeat every 5 mins as needed ---• Maximum 5 doses ---• Hypertension and some medications (eg proteases) are a contraindication • Misoprostol
Flashcard 1414450253068
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Methyl Prostaglandin F2a) ---• 250 ug IM or intramyometrial; repeat every 15 min as needed ---• Maximum cumulative dose 2 mg (8 doses) ---• Asthma a relative contraindication • Methylergonovine maleate ---• 0.25 mg IM/<span>0.125 mg IV ---• Repeat every 5 mins as needed ---• Maximum 5 doses ---• Hypertension and some medications (eg proteases) are a contraindication • Misoprostol (off-label u
Flashcard 1414451825932
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
250 ug IM or intramyometrial; repeat every 15 min as needed ---• Maximum cumulative dose 2 mg (8 doses) ---• Asthma a relative contraindication • Methylergonovine maleate ---• 0.25 mg IM/0.125 mg IV ---• Repeat every <span>5 mins as needed ---• Maximum 5 doses ---• Hypertension and some medications (eg proteases) are a contraindication • Misoprostol (off-label use) ---• 600-800 ug po/sl
Flashcard 1414453398796
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
at every 15 min as needed ---• Maximum cumulative dose 2 mg (8 doses) ---• Asthma a relative contraindication • Methylergonovine maleate ---• 0.25 mg IM/0.125 mg IV ---• Repeat every 5 mins as needed ---• Maximum <span>5 doses ---• Hypertension and some medications (eg proteases) are a contraindication • Misoprostol (off-label use) ---• 600-800 ug po/sl (faster onset) or pr/pv ---• S
Flashcard 1414454971660
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
needed ---• Maximum cumulative dose 2 mg (8 doses) ---• Asthma a relative contraindication • Methylergonovine maleate ---• 0.25 mg IM/0.125 mg IV ---• Repeat every 5 mins as needed ---• Maximum 5 doses ---• <span>Hypertension and some medications (eg proteases) are a contraindication • Misoprostol (off-label use) ---• 600-800 ug po/sl (faster onset) or pr/pv ---• Side effect: Pyrexia if >600ug given • Tranexamic Acid (cy
Flashcard 1414457855244
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
postpartum endometritis can be cause of late PPH -presents with fever, increased WBC, Hg can be normal -delivery usually no issues
Flashcard 1414459428108
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
postpartum endometritis can be cause of late PPH -presents with fever, increased WBC, Hg can be normal -delivery usually no issues
Flashcard 1414462311692
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
late PPH management: - admit vs outpatient ---admit if fever, Hg 50 -oral abx, oral miso -if admitted, IV Pit -observe carefully over 24h
Flashcard 1414463884556
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
late PPH management: - admit vs outpatient ---admit if fever, Hg 50 -oral abx, oral miso -if admitted, IV Pit -observe carefully over 24h
Flashcard 1414465457420
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
late PPH management: - admit vs outpatient ---admit if fever, Hg 50 -oral abx, oral miso -if admitted, IV Pit -observe carefully over 24h