Edited, memorised or added to reading queue
on 01-Mar-2021 (Mon)
Do you want BuboFlash to help you learning these things? Click here to log in or create user.
Flashcard 4965946494220
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itLet a discrete random variable \(X\) have \(k\) possible values \(\{ x_i \}_{i=1}^k\). The expectation of \(X\) denoted as \(\mathbb E[X]\) is given by, \(\mathbb E[X] \stackrel{\textrm{def}}{=} \sum_{i=1}^k \left[ x_i \cdot \textrm{Pr} \left( X = x_i \right) \right] \\ = x_1 \cdot \textrm{Pr} \left( X = x_1 \right) + x_2 \cdot \textrm{Pr} \left( X = x_2 \right) + \cdots + x_k \cdot \textrm{Pr} \left( X = x_k \right)\) where \(\textrm{Pr} \left( X = x_i \right)\) is the probability that \(X\) has the value \(x_i\) according to the pmf. The expectation of a random variable is also called the mean, average or expected value and is frequently denoted with the letter \(\mu\) . The expectation is one of the most important statistics of a random variable.
Original toplevel document (pdf)
cannot see any pdfs| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
opics are updated as new evidence becomes available and our peer review process is complete. Literature review current through: Jan 2021. | This topic last updated: Dec 02, 2019. INTRODUCTION — <span>Although hypokalemia can be transiently induced by the entry of potassium into the cells, most cases result from unreplenished gastrointestinal or urinary losses due, for example, to vomiting, diarrhea, or diuretic therapy [1-3]. (See "Causes of hypokalemia in adults".) Potassium replacement is primarily indicated when hypokalemia is due to potassium loss, and there is a significant deficit in body potass
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
in disorders such as hypokalemic or thyrotoxic periodic paralysis in which the hypokalemia is due to redistribution of potassium into the cells, often in association with significant symptoms. <span>Potassium is given cautiously in redistributive hypokalemia since the hypokalemia is transient and the administration of potassium can lead to rebound hyperkalemia when the underlying process is corrected and potassium moves back out of the cells. The recommended regimens for acute therapy in this disorder are presented elsewhere. (See "Hypokalemic periodic paralysis", section on 'Acute treatment' and "Thyrotoxic periodic paralys
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
apy [1-3]. (See "Causes of hypokalemia in adults".) Potassium replacement is primarily indicated when hypokalemia is due to potassium loss, and there is a significant deficit in body potassium. <span>It is also warranted for acute therapy in disorders such as hypokalemic or thyrotoxic periodic paralysis in which the hypokalemia is due to redistribution of potassium into the cells, often in association with significant symptoms. Potassium is given cautiously in redistributive hypokalemia since the hypokalemia is transient and the administration of potassium can lead to rebound hyperkalemia when the underlying
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
evaluation of patients with hypokalemia are discussed separately. (See "Causes of hypokalemia in adults" and "Evaluation of the adult patient with hypokalemia".) MANIFESTATIONS OF HYPOKALEMIA — <span>The severity of the manifestations of hypokalemia tends to be proportionate to the degree and duration of the reduction in serum potassium. Symptoms generally do not become manifest until the serum potassium is below 3.0 mEq/L, unless the serum potassium falls rapidly or the patient has a potentiating factor, such as a predisposition to arrhythmia due to the use of digitalis. Symptoms usually resolve with correction of the hypokalemia. Severe muscle weakness or rhabdomyolysis — Muscle weakness usually does not occur at serum potassium concentrations above 2.5 mEq/L if the hypokalemia develops slowly [2]. However, sign
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
potentiating factor, such as a predisposition to arrhythmia due to the use of digitalis. Symptoms usually resolve with correction of the hypokalemia. Severe muscle weakness or rhabdomyolysis — <span>Muscle weakness usually does not occur at serum potassium concentrations above 2.5 mEq/L if the hypokalemia develops slowly [2]. However, significant muscle weakness can occur at serum potassium concentrations below 2.5 mEq/L or at higher values with hypokalemia of acute onset, as occurs in hypokalemic or thyrotoxic periodic paralysis. In addition, the pathophysiology of weakness in these disorders is more complex. (See "Myopathies of systemic disease", section on 'Hypokalemic myopathy'.) The pattern of weakness in hypokalemia is similar to that associated with hyperkalemia. Weakness usually begin
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
mic or thyrotoxic periodic paralysis. In addition, the pathophysiology of weakness in these disorders is more complex. (See "Myopathies of systemic disease", section on 'Hypokalemic myopathy'.) <span>The pattern of weakness in hypokalemia is similar to that associated with hyperkalemia. Weakness usually begins in the lower extremities, progresses to the trunk and upper extremities, and can worsen to the point of paralysis. (See "Clinical manifestations of hyperkalemia in adults", section on 'Severe muscle weakness or paralysis'.) In addition to causing muscle weakness, severe potassium depletion (serum po
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
resses to the trunk and upper extremities, and can worsen to the point of paralysis. (See "Clinical manifestations of hyperkalemia in adults", section on 'Severe muscle weakness or paralysis'.) <span>In addition to causing muscle weakness, severe potassium depletion (serum potassium less than 2.5 mEq/L) can lead to muscle cramps, rhabdomyolysis, and myoglobinuria [4-7]. Potassium release from muscle cells during exercise normally mediates vasodilation and an appropriate increase in muscle blood flow [8]. Decreased potassium release due to profound hypokalemia can diminish blood flow to muscles during exertion, leading to ischemic rhabdomyolysis [8]. The clinical and pathologic abnormalities are reversible with potassium repletion [4]. A potential diagnostic problem is that the release of potassium from the cells with rhabdomyolysis can mask the severity of the underlying hypokalemia or even lead to normal or high values. (See "Causes of rhabdomyolysis", section on 'Electrolyte disorders'.) Other manifestations of muscle dysfunction due to hypokalemia include: ●Respiratory muscle weakness, which can be s
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
om the cells with rhabdomyolysis can mask the severity of the underlying hypokalemia or even lead to normal or high values. (See "Causes of rhabdomyolysis", section on 'Electrolyte disorders'.) <span>Other manifestations of muscle dysfunction due to hypokalemia include: ●Respiratory muscle weakness, which can be severe enough to result in respiratory failure and death. ●Involvement of gastrointestinal muscles, resulting in ileus and its associated symptoms of distension, anorexia, nausea, and vomiting. The hypokalemia in some of these patients is caused by concomitant diarrhea. As an example, several reports have noted an association between colonic pseudo-obstruction (Ogilvie's syndr
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
abnormally high fecal potassium content [9,10]. (See "Acute colonic pseudo-obstruction (Ogilvie's syndrome)", section on 'Clinical manifestations'.) Cardiac arrhythmias and ECG abnormalities — <span>A variety of arrhythmias may be seen in patients with hypokalemia. These include premature atrial complex (PAC; also referred to a premature atrial beat, premature supraventricular complex, or premature supraventricular beat) and premature ventricular beats, sinus bradycardia, paroxysmal atrial or junctional tachycardia, atrioventricular block, and ventricular tachycardia or fibrillation [2]. Hypokalemia produces characteristic changes on the ECG although they are not seen in all patients. There is depression of the ST segment, decrease in the amplitude of the T wave, and an increase in the amplitude of U waves which occur at the end of the T wave (waveform 1). U waves are often seen in the lateral precordial leads V4 to V6. Hypokalemia also prolongs the QT interval [11-13]. (See "ECG tutorial: Miscellaneous diagnoses", section on 'Hypokalemia'.) There is a large interpatient variability in the serum potassium concentration that is associated with progress
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
1). U waves are often seen in the lateral precordial leads V4 to V6. Hypokalemia also prolongs the QT interval [11-13]. (See "ECG tutorial: Miscellaneous diagnoses", section on 'Hypokalemia'.) <span>There is a large interpatient variability in the serum potassium concentration that is associated with progression of ECG changes or arrhythmias. In a carefully controlled trial of thiazide therapy (hydrochlorothiazide 50 mg/day), there was a two-fold increase in ventricular arrhythmias (as detected by Holter monitoring) in the small proportion of patients in whom the serum potassium concentration fell to or below 3.0 mEq/L [14]. In addition, the presence of concomitant factors, such as coronary ischemia, digitalis, increased beta-adrenergic activity, and magnesium depletion, can promote arrhythmias; the last two of these cofactors can also lower the serum potassium concentration: ●Epinephrine released during a stress response (as with coronary ischemia) drives potassium into the cells, possibly worsening preexisting hypokalemia. A similar effect can be seen wit
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ary ischemia, digitalis, increased beta-adrenergic activity, and magnesium depletion, can promote arrhythmias; the last two of these cofactors can also lower the serum potassium concentration: ●<span>Epinephrine released during a stress response (as with coronary ischemia) drives potassium into the cells, possibly worsening preexisting hypokalemia. A similar effect can be seen with bronchodilator therapy with a beta-adrenergic agonist. (See "Causes of hypokalemia in adults", section on 'Elevated beta-adrenergic activity'.) ●Hypokalemia may be associated with magnesium depletion (due, for example, to diuretics or diarr
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
g hypokalemia. A similar effect can be seen with bronchodilator therapy with a beta-adrenergic agonist. (See "Causes of hypokalemia in adults", section on 'Elevated beta-adrenergic activity'.) ●<span>Hypokalemia may be associated with magnesium depletion (due, for example, to diuretics or diarrhea), both of which promote the development of arrhythmias. Hypokalemia and hypomagnesemia are associated with an increased risk of torsades de pointes, particularly in patients treated with drugs that prolong the QT interval or those with a genetic predisposition to the long QT syndrome. In addition to its direct proarrhythmic effect, hypomagnesemia can increase urinary potassium losses and lower the serum potassium concentration. (See "Acquired long QT syndrome: Definitions, causes, and pathophysiology", section on 'Hypokalemia, hypomagnesemia, and hypocalcemia' and 'Hypomagnesemia and redistributive hypokalemia
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
c nephropathy ●Elevation in blood pressure These changes are discussed in detail elsewhere. (See "Hypokalemia-induced renal dysfunction" and "Potassium and hypertension".) Glucose intolerance — <span>Hypokalemia reduces insulin secretion, which may play an important role in thiazide-associated diabetes. However, worsening glucose tolerance is much less common in the era of low-dose thiazide therapy (eg, 12.5 to 25 mg of hydrochlorothiazide) (figure 1). (See "Pathogenesis of type 2 diabetes mellitus", section on 'Thiazide diuretics'.) PATHOGENESIS OF SYMPTOMS — The neuromuscular and cardiac symptoms induced by hypokalemia a
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
of low-dose thiazide therapy (eg, 12.5 to 25 mg of hydrochlorothiazide) (figure 1). (See "Pathogenesis of type 2 diabetes mellitus", section on 'Thiazide diuretics'.) PATHOGENESIS OF SYMPTOMS — <span>The neuromuscular and cardiac symptoms induced by hypokalemia are related to alterations in the generation of the action potential [2]. The ease of generating an action potential (called membrane excitability) is related both to the magnitude of the resting membrane potential and to the activation state of membrane sodium channels. Opening the sodium channels leads to the passive diffusion of extracellular sodium into the cells, which is the primary step in this process. According to the Nernst equation, the resting membrane potential is related to the ratio of the intracellular to the extracellular potassium concentration. In skeletal muscle, a reduction in the serum (extracellular) potassium concentration will increase this ratio and therefore hyperpolarize the cell membrane (that is, make the resting potential more electronegative); this impairs the ability of the muscle to depolarize and contract, leading to weakness. However, in some cardiac cells (such as Purkinje fibers in the conducting system), hypokalemia causes K2P1 channels, which are normally selective for potassium, to transport sodium into the cells, causing depolarization [16,17]. This leads to increased membrane excitability and arrhythmias. Hypokalemia also delays ventricular repolarization by inhibiting the activity of potassium channels responsible for this component of the cardiac electrical cycle [12]. (See "Reentry and the development of cardiac arrhythmias".) In addition, hypokalemia causes ventricular arrhythmias through downregulation of cardiac Na-K-ATPase activity [18,19]. This produces an increase in intracellular sodium, which impedes removal of intracellular calcium by the Na-Ca exchanger, leading to intracellular calcium overload. The ensuing activation of calmodulin kinase II activity reduces repolarization reserve by activating late sodium and calcium currents [20]. This, in turn, predisposes the heart to early afterdepolarization-associated arrhythmias, such as Torsades de pointes and polymorphic ventricular tachycardia [20]. DIAGNOSIS AND EVALUATION — Once the presence of hypokalemia has been documented, attempts should be made from the history and laboratory findings to identify the cause of the hypokalem
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
unctional manifestations of hypokalemia, and the potassium deficit should be estimated. (See "Evaluation of the adult patient with hypokalemia" and 'Estimation of the potassium deficit' below.) <span>The assessment of the hypokalemic patient begins with evaluation of muscle strength and obtaining an electrocardiogram to assess the cardiac consequences of the hypokalemia, with particular attention to the QT interval. At serum potassium concentrations below 2.5 mEq/L, severe muscle weakness and/or marked electrocardiographic changes may be present and require immediate treatment. (See 'Manifestations of hypokalemia' above and "ECG tutorial: Miscellaneous diagnoses", section on 'Hypokalemia'.) Telemetry or continuous ECG monitoring is indicated for hypokalemic p
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
d electrocardiographic changes may be present and require immediate treatment. (See 'Manifestations of hypokalemia' above and "ECG tutorial: Miscellaneous diagnoses", section on 'Hypokalemia'.) <span>Telemetry or continuous ECG monitoring is indicated for hypokalemic patients with a prolonged QT, other ECG changes associated with hypokalemia, and/or underlying cardiac issues that predispose to arrhythmia in the setting of hypokalemia (digoxin toxicity, myocardial infarction, underlying long QT syndrome, etc) [21,22]. TREATMENT General issues — The goals of therapy in hypokalemia are to prevent or treat life-threatening complications (arrhythmias, paralysis, rhabdomyolysis, and diaphragmatic
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
or treat life-threatening complications (arrhythmias, paralysis, rhabdomyolysis, and diaphragmatic weakness), to replace the potassium deficit, and to diagnose and correct the underlying cause. <span>The urgency of therapy depends upon the severity of hypokalemia, associated and/or comorbid conditions, and the rate of decline in serum potassium concentration. The risk of arrhythmia from hypokalemia is highest in older patients, patients with organic heart disease, and patients on digoxin or antiarrhythmic drugs [23]. Potassium replacement i
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
d correct the underlying cause. The urgency of therapy depends upon the severity of hypokalemia, associated and/or comorbid conditions, and the rate of decline in serum potassium concentration. <span>The risk of arrhythmia from hypokalemia is highest in older patients, patients with organic heart disease, and patients on digoxin or antiarrhythmic drugs [23]. Potassium replacement is the mainstay of therapy in hypokalemia. Such therapy is clearly warranted in patients with hypokalemia due to renal or gastrointestinal losses. It should also b
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
n serum potassium concentration. The risk of arrhythmia from hypokalemia is highest in older patients, patients with organic heart disease, and patients on digoxin or antiarrhythmic drugs [23]. <span>Potassium replacement is the mainstay of therapy in hypokalemia. Such therapy is clearly warranted in patients with hypokalemia due to renal or gastrointestinal losses. It should also be considered when hypokalemia is due to redistribution of potassium from the extracellular fluid into the cells (eg, hypokalemic periodic paralysis, insulin therapy) if serious complications such as paralysis, rhabdomyolysis, or arrhythmias are present or imminent. (See "Causes of hypokalemia in adults", section on 'Increased entry into cells'.) Hypomagnesemia and redistributive hypokalemia — The underlying cause of the hypokalemia should be ident
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
in therapy) if serious complications such as paralysis, rhabdomyolysis, or arrhythmias are present or imminent. (See "Causes of hypokalemia in adults", section on 'Increased entry into cells'.) <span>Hypomagnesemia and redistributive hypokalemia — The underlying cause of the hypokalemia should be identified as quickly as possible, particularly the presence of hypomagnesemia or redistributive hypokalemia: ●Patients with hypokalemia may also have hypomagnesemia due to concurrent loss with diarrhea or diuretic therapy or, in patients with hypomagnesemia as the primary abnormality, renal po
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
and redistributive hypokalemia — The underlying cause of the hypokalemia should be identified as quickly as possible, particularly the presence of hypomagnesemia or redistributive hypokalemia: ●<span>Patients with hypokalemia may also have hypomagnesemia due to concurrent loss with diarrhea or diuretic therapy or, in patients with hypomagnesemia as the primary abnormality, renal potassium wasting [24,25]. Such patients can be refractory to potassium replacement alone [26]. Thus, measurement of serum magnesium should be considered in patients with hypokalemia and, if present, hypomagnesemia should be treated. (See "Hypomagnesemia: Clinical manifestations of magnesium depletion", section on 'Hypokalemia' and "Hypomagnesemia: Evaluation and treatment".) ●A potential complication of potassium t
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
in redistributive hypokalemia is rebound hyperkalemia as the initial process causing redistribution resolves or is corrected. Such patients can develop fatal hyperkalemic arrhythmias [3,27-30]. <span>The risk of rebound hyperkalemia is particularly high in patients with hypokalemic or thyrotoxic periodic paralysis in whom rebound hyperkalemia has been described in 40 to 60 percent of treated attacks. (See "Thyrotoxic periodic paralysis", section on 'Acute treatment'.) ●When increased sympathetic tone is thought to play a major role, the administration of a nonspecific beta blocker,
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ic or thyrotoxic periodic paralysis in whom rebound hyperkalemia has been described in 40 to 60 percent of treated attacks. (See "Thyrotoxic periodic paralysis", section on 'Acute treatment'.) ●<span>When increased sympathetic tone is thought to play a major role, the administration of a nonspecific beta blocker, such as propranolol, should be considered. The greatest experience is with acute attacks of hypokalemic thyrotoxic periodic paralysis [31], although head injury and theophylline toxicity can also result in redistributive hypokalemia [32-35], presumably due to sympathetic activation and elevated epinephrine levels [36]. In such patients, high-dose oral propranolol or intravenous propranolol rapidly reverses the hypokalemia and paralysis seen in acute attacks, without rebound hyperkalemia. (See "Thyrotoxic periodic paralysis", section on 'Acute treatment'.) Estimation of the potassium deficit — Estimation of the potassium deficit assumes that there is a normal distributi
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ses the hypokalemia and paralysis seen in acute attacks, without rebound hyperkalemia. (See "Thyrotoxic periodic paralysis", section on 'Acute treatment'.) Estimation of the potassium deficit — <span>Estimation of the potassium deficit assumes that there is a normal distribution of potassium between the cells and the extracellular fluid. The most common settings in which this estimation does not apply is diabetic ketoacidosis or nonketotic hyperglycemia, and in redistributive causes of hypokalemia such as hypokalemic periodic paralysis. (See "Causes of hypokalemia in adults", section on 'Increased entry into cells'.) The goals of potassium replacement in patients with hypokalemia due to potassium losses are to rapidly
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ncentration to a safe level and then replace the remaining deficit at a slower rate over days to weeks to allow for equilibration of potassium between plasma and intracellular stores [3,23,37]. <span>Estimation of the potassium deficit and careful monitoring of the serum potassium helps to prevent hyperkalemia due to excessive supplementation. This is not an uncommon outcome in hospitalized patients since, in one report, one in six patients developed mild hyperkalemia following potassium administration for hypokalemia [38]. The risk of overcorrection is increased in patients with a reduced glomerular filtration rate. The potassium deficit varies directly with the severity of hypokalemia. In different studies, the serum potassium concentration fell by approximately 0.27 mEq/L for every 100 mEq reduct
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
tion for hypokalemia [38]. The risk of overcorrection is increased in patients with a reduced glomerular filtration rate. The potassium deficit varies directly with the severity of hypokalemia. <span>In different studies, the serum potassium concentration fell by approximately 0.27 mEq/L for every 100 mEq reduction in total body potassium stores [3,37,39] and, in chronic hypokalemia, a potassium deficit of 200 to 400 mEq is required to lower the serum potassium concentration by 1 mEq/L [39]. However, these estimates are only an approximation of the amount of potassium replacement required to normalize the serum potassium concentration and careful monitoring is required. Uncontrolled diabetes — In diabetic ketoacidosis or a hyperosmolar hyperglycemic state (nonketotic hyperglycemia), hyperosmolality and insulin deficiency favor the movement of potassiu
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
se estimates are only an approximation of the amount of potassium replacement required to normalize the serum potassium concentration and careful monitoring is required. Uncontrolled diabetes — <span>In diabetic ketoacidosis or a hyperosmolar hyperglycemic state (nonketotic hyperglycemia), hyperosmolality and insulin deficiency favor the movement of potassium out of cells. As a result, the serum potassium concentration at presentation may be normal or even elevated despite a marked potassium deficit due to urinary and, in some patients, gastrointestinal losses [40]. The initiation of insulin therapy and fluid replacement will lower the serum potassium toward the level appropriate for the potassium deficit. Potassium supplementation is usually begun once the serum potassium concentration is 4.5 mEq/L or lower. Occasional patients with uncontrolled diabetes (eg, 6 percent in one study) have more marked potassium loss and are hypokalemic at presentation [41]. Such patients require aggressive po
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
t will lower the serum potassium toward the level appropriate for the potassium deficit. Potassium supplementation is usually begun once the serum potassium concentration is 4.5 mEq/L or lower. <span>Occasional patients with uncontrolled diabetes (eg, 6 percent in one study) have more marked potassium loss and are hypokalemic at presentation [41]. Such patients require aggressive potassium replacement (20 to 30 mEq/hour), which can be achieved by the addition of 40 to 60 mEq of potassium chloride to each liter of one-half isotonic saline. Since insulin will worsen the hypokalemia, insulin therapy should be delayed until the serum potassium is above 3.3 mEq/L to avoid possible complications of hypokalemia such as cardiac arrhythmias and respiratory muscle weakness. (See 'Intravenous potassium repletion' below and 'Manifestations of hypokalemia' above.) These issues are discussed in detail elsewhere. (See "Diabetic ketoacidosis and hyperosmolar hyp
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
hosphate, potassium bicarbonate or its precursors (potassium citrate, potassium acetate) or potassium gluconate [3,23,37]. The choice among these preparations varies with the clinical setting: ●<span>Potassium bicarbonate or its precursors are preferred in patients with hypokalemia and metabolic acidosis (eg, renal tubular acidosis or diarrhea) [23,37]. Only potassium acetate is available for intravenous use. ●Potassium phosphate should be considered only in the rarely seen patients with hypokalemia and hypophosphatemia, as might occur with proximal (type 2) renal tubular acidosis associated
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
e or its precursors are preferred in patients with hypokalemia and metabolic acidosis (eg, renal tubular acidosis or diarrhea) [23,37]. Only potassium acetate is available for intravenous use. ●<span>Potassium phosphate should be considered only in the rarely seen patients with hypokalemia and hypophosphatemia, as might occur with proximal (type 2) renal tubular acidosis associated with Fanconi syndrome and phosphate wasting [37,42,43]. ●Potassium chloride is preferred in all other patients for two major reasons [1]: •Patients with hypokalemia and metabolic alkalosis are often chloride depleted due, for example, to di
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
the rarely seen patients with hypokalemia and hypophosphatemia, as might occur with proximal (type 2) renal tubular acidosis associated with Fanconi syndrome and phosphate wasting [37,42,43]. ●<span>Potassium chloride is preferred in all other patients for two major reasons [1]: •Patients with hypokalemia and metabolic alkalosis are often chloride depleted due, for example, to diuretic therapy or vomiting. In such patients, chloride depletion contributes to maintenance of the metabolic alkalosis by enhancing renal bicarbonate reabsorption and may contribute to potassium wasting as sodium is reabsorbed in exchange for secreted potassium rather than with chloride [3,44,45]. It has been estimated that administration of non-chloride-containing potassium salts in the presence of metabolic alkalosis results in the retention of only 40 percent as much potassium as the administration of potassium chloride [45]. (See "Pathogenesis of metabolic alkalosis", section on 'Chloride depletion' and "Treatment of metabolic alkalosis", section on 'Treatment'.) •Potassium chloride raises the serum potassium concentration at a faster rate than potassium bicarbonate. Chloride is primarily an extracellular anion that does not enter cells to the same extent as bicarbonate, thereby promoting maintenance of the administered potassium in the extracellular fluid [46] In addition, potassium bicarbonate may partially offset the benefits of potassium administration by aggravating metabolic alkalosis, if present. Oral potassium chloride can be given in crystalline form (salt substitutes), as a liquid, or in a slow-release tablet or capsule. Salt substitutes contain 50 to 65 mEq per level teaspo
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
stered potassium in the extracellular fluid [46] In addition, potassium bicarbonate may partially offset the benefits of potassium administration by aggravating metabolic alkalosis, if present. <span>Oral potassium chloride can be given in crystalline form (salt substitutes), as a liquid, or in a slow-release tablet or capsule. Salt substitutes contain 50 to 65 mEq per level teaspoon; they are safe, well tolerated, and much less expensive than the other preparations [47]. Liquid forms of potassium chloride are also inexpensive, but are often unpalatable. Nevertheless, they may be preferred in patients with an enteral feeding tube or who are unable to swallow tablets. Slow-release tablets are better tolerated, but they have been associated with gastrointestinal ulceration and bleeding, which have been ascribed to local accumulation of high concentrations of potassium [48]. The risk is relatively low, and even lower with microencapsulated preparations (eg, microK or Klor-Con) compared to wax matrix tablets [3]. Increasing the intake of potassium-rich foods, such as oranges and bananas (table 1), is less effective, in part because dietary potassium is predominantly in the form of potassium pho
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ccumulation of high concentrations of potassium [48]. The risk is relatively low, and even lower with microencapsulated preparations (eg, microK or Klor-Con) compared to wax matrix tablets [3]. <span>Increasing the intake of potassium-rich foods, such as oranges and bananas (table 1), is less effective, in part because dietary potassium is predominantly in the form of potassium phosphate or potassium citrate which, as mentioned earlier in this section, results in the retention of only 40 percent as much potassium as potassium chloride [45]. In addition, the potassium concentration is relatively low in fruit (eg, approximately 2.2 mEq/inch [0.9 mEq/cm] in bananas) [49]. As a result, it would take two to three bananas to provide 40 mEq. Intravenous therapy — Potassium chloride can be given intravenously to patients who are unable to take oral therapy or as an adjunct to oral replacement in patients who have severe sym
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
●Among patients with ongoing losses, the rate of potassium administration recommended below must be increased by the rate of potassium loss to produce the desired rate of potassium repletion. ●<span>Stable patients with chronic diuretic therapy (at a fixed dose), primary aldosteronism (unless aldosterone secretion increases), or Gitelman or Bartter syndrome typically do not develop progressive hypokalemia because the increased urinary potassium losses are balanced by hypokalemia-induced potassium retention. The net effect is a new steady state in which potassium intake and output are in balance, with a lower-than-normal serum potassium concentration. A potassium-sparing diuretic is usually required in such patients who do not respond adequately to potassium supplementation. (See "General principles of disorders of water balance (hyponatremia and hypernatremia) and sodium balance (hypovolemia and edema)", section on 'The steady state'.) Potassium-sparing di
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
See "General principles of disorders of water balance (hyponatremia and hypernatremia) and sodium balance (hypovolemia and edema)", section on 'The steady state'.) Potassium-sparing diuretics — <span>There are two classes of potassium-sparing diuretics: blockers of the cortical collecting tubule sodium channels (amiloride and triamterene); and the aldosterone (mineralocorticoid receptor) antagonists (spironolactone and eplerenone). With respect to treating hypokalemia, these drugs are used in patients with renal potassium wasting in whom, as noted in the preceding section, potassium supplements may not be sufficiently effective. Amiloride is usually preferred to a mineralocorticoid receptor antagonist because it is better tolerated (see "Triamterene nephrotoxicity"). Primary aldosteronism is an important excep
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
spect to treating hypokalemia, these drugs are used in patients with renal potassium wasting in whom, as noted in the preceding section, potassium supplements may not be sufficiently effective. <span>Amiloride is usually preferred to a mineralocorticoid receptor antagonist because it is better tolerated (see "Triamterene nephrotoxicity"). Primary aldosteronism is an important exception since spironolactone or eplerenone is preferred to block apparent adverse effects of excess aldosterone on the heart and vascular system in patients diagnosed with this disorder. (See "Treatment of primary aldosteronism", section on 'First line: Mineralocorticoid receptor antagonists' and "Pathophysiology and clinical features of primary aldosteronism", section
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
markedly reduce urinary potassium excretion (decreased renal perfusion due to the fall in cardiac output, therapy with an angiotensin inhibitor, and therapy with spironolactone or eplerenone). <span>Among patients with heart failure, mineralocorticoid receptor antagonists should be given only if the serum creatinine is less than or equal to 2.5 mg/dL (221 micromol/L) in men and 2.0 mg/dL (177 micromol/L) in women and the serum potassium is less than 5.0 mEq/L. (See "Secondary pharmacologic therapy in heart failure with reduced ejection fraction (HFrEF) in adults", section on 'Dosing and cautions' and "Secondary pharmacologic therapy in heart
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ection on 'Dosing and cautions' and "Secondary pharmacologic therapy in heart failure with reduced ejection fraction (HFrEF) in adults", section on 'Monitoring'.) Mild to moderate hypokalemia — <span>Most hypokalemic patients have a serum potassium concentration of 3.0 to 3.4 mEq/L. This degree of potassium depletion usually produces no symptoms. Exceptions include patients with heart disease (particularly if they are taking digitalis or certain other antiarrhythmic drugs or are undergoing cardiac surgery [50,51]) and patients with cirrhosis, in whom hypokalemia can increase ammonia generation and promote the development of hepatic encephalopathy. Treatment of mild to moderate hypokalemia depends upon the cause of the hypokalemia and acid-base status: ●Patients with gastrointestinal losses are treated with potassium chloride if
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
can increase ammonia generation and promote the development of hepatic encephalopathy. Treatment of mild to moderate hypokalemia depends upon the cause of the hypokalemia and acid-base status: ●<span>Patients with gastrointestinal losses are treated with potassium chloride if they have metabolic alkalosis (as usually seen with vomiting) or a normal serum bicarbonate concentration, and with potassium bicarbonate (or potassium citrate or acetate) in the presence of metabolic acidosis (as seen with diarrhea or renal tubular acidosis). Treatment is usually started with 10 to 20 mEq of potassium given two to four times per day (20 to 80 mEq/day), depending upon the severity of the hypokalemia. (See 'Potassium preparations' above.) ●By contrast, potassium supplements at usual doses produce only modest elevations in serum potassium in patients with hypokalemia due to renal pota
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ment is usually started with 10 to 20 mEq of potassium given two to four times per day (20 to 80 mEq/day), depending upon the severity of the hypokalemia. (See 'Potassium preparations' above.) ●<span>By contrast, potassium supplements at usual doses produce only modest elevations in serum potassium in patients with hypokalemia due to renal potassium wasting (eg, chronic diuretic therapy, primary aldosteronism). As soon as the serum potassium rises, there is less hypokalemia-induced potassium retention and most of the administered potassium is excreted in the urine. Thus, a potassium-sparing diuretic is likely to be more effective. Amiloride is usually preferred to a mineralocorticoid receptor antagonist because it is better tolerated. Primary aldosteronism is an important exception since spironolactone or eplerenone is preferred to block apparent adverse effects of excess aldosterone on the heart and vascular system. (See 'Ongoing losses and the steady state' above and 'Potassium-sparing diuretics' above.) Patients with mild to moderate hypokalemia who are treated with potassium supplements are typ
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
py. Patients who cannot take oral therapy require intravenous repletion. Sequential monitoring of the serum potassium is essential to determine the response. Severe or symptomatic hypokalemia — <span>Potassium must be given more rapidly to patients with hypokalemia that is severe (serum potassium less than 2.5 to 3.0 mEq/L) or symptomatic (arrhythmias, marked muscle weakness, or rhabdomyolysis). A potential diagnostic and therapeutic problem in patients with hypokalemia-induced rhabdomyolysis is that the release of potassium from the muscle cells can mask the severity of the u
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
sium must be given more rapidly to patients with hypokalemia that is severe (serum potassium less than 2.5 to 3.0 mEq/L) or symptomatic (arrhythmias, marked muscle weakness, or rhabdomyolysis). <span>A potential diagnostic and therapeutic problem in patients with hypokalemia-induced rhabdomyolysis is that the release of potassium from the muscle cells can mask the severity of the underlying hypokalemia or even lead to normal or elevated values at presentation or after potassium supplementation. If the serum potassium is normal or elevated at baseline, it will not be possible to be certain that underlying hypokalemia was responsible for the rhabdomyolysis and initial potassium therapy in such patients is not warranted and may be dangerous. In patients who present with hypokalemia, potassium therapy can be initiated with repeated monitoring of the serum potassium (eg, every four to six hours initially). Particular caution
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
anted and may be dangerous. In patients who present with hypokalemia, potassium therapy can be initiated with repeated monitoring of the serum potassium (eg, every four to six hours initially). <span>Particular caution must be exercised when repleting potassium in patients with a concurrent disorder that, when treated, will tend to drive potassium into the cells and worsen the hypokalemia. The two main examples are insulin therapy in diabetic ketoacidosis or nonketotic hyperglycemia, and bicarbonate therapy in metabolic acidosis with a normal anion gap. Potassium repletion is most easily accomplished orally but can be given intravenously. The serum potassium concentration can transiently rise by as much as 1 to 1.5 mEq/L after an oral
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
nd worsen the hypokalemia. The two main examples are insulin therapy in diabetic ketoacidosis or nonketotic hyperglycemia, and bicarbonate therapy in metabolic acidosis with a normal anion gap. <span>Potassium repletion is most easily accomplished orally but can be given intravenously. The serum potassium concentration can transiently rise by as much as 1 to 1.5 mEq/L after an oral dose of 40 to 60 mEq, and by as much as 2.5 to 3.5 mEq/L after 135 to 160 mEq [52,53]. The serum potassium concentration will then fall back toward baseline over a few hours, as most of the exogenous potassium is taken up by the cells [54]. A patient with a serum potassium concentration of 2.0 mEq/L, for example, may have a 400 to 800 mEq potassium deficit [39]. In patients with severe hypokalemia, potassium chloride can be given orally in doses of 40 mEq, three to four times per day or, particularly in patients also treated with intravenous potassium, 20 mEq every two to three hours. As noted in the preceding section, potassium supplements at usual doses produce only modest elevations in serum potassium in patients with hypokalemia due to renal potassium wasting (eg
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
m potassium in patients with hypokalemia due to renal potassium wasting (eg, chronic diuretic therapy, primary aldosteronism). Thus, a potassium-sparing diuretic is likely to be more effective. <span>Careful monitoring is essential in patients treated with potassium. We suggest that the serum potassium should initially be measured every two to four hours to ascertain the response to therapy. If tolerated, this regimen should be continued until the serum potassium concentration is persistently above 3.0 to 3.5 mEq/L and symptoms or signs attributable to hypokalemia have resolved. Thereafter, the dose and frequency of administration can be reduced to that used in mild to moderate hypokalemia since aggressive repletion is no longer required and gastric irritation can be avoided. (See 'Mild to moderate hypokalemia' above.) Intravenous potassium repletion — Potassium chloride can be given intravenously as an adjunct to oral replacement in patients who have severe
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
take oral medications. Potential constraints to intravenous therapy for severe hypokalemia include a risk of volume overload in susceptible subjects and hyperkalemia due to excessive repletion. <span>A saline rather than a dextrose solution should be used for initial therapy since the administration of dextrose stimulates the release of insulin which drives extracellular potassium into the cells. This can lead to a transient 0.2 to 1.4 mEq/L reduction in the serum potassium concentration, particularly if the solution contains only 20 mEq/L of potassium [3,55]. The transient reduction in serum potassium can induce arrhythmias in susceptible patients, such as those taking digitalis [55]. The necessity for aggressive intravenous potassium replacement most commonly occurs in patients with diabetic ketoacidosis or hyperosmolar hyperglycemic state (nonketotic hyperglycemia)
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ses, but usually present with normal or even high serum potassium levels due to transcellular potassium shifts. Patients who present with hypokalemia have an even larger potassium deficit [56]. <span>Furthermore, treatment with insulin and intravenous fluids will exacerbate the hypokalemia and minimize the efficacy of potassium repletion. Thus, insulin therapy should be delayed until the serum potassium is above 3.3 mEq/L to avoid possible complications of hypokalemia such as cardiac arrhythmias, cardiac arrest, and respiratory muscle weakness. (See "Diabetic ketoacidosis and hyperosmolar hyperglycemic state in adults: Clinical features, evaluation, and diagnosis", section on 'Serum potassium' and 'Manifestations of hypokalemi
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ection on 'Serum potassium' and 'Manifestations of hypokalemia' above and "Diabetic ketoacidosis and hyperosmolar hyperglycemic state in adults: Treatment", section on 'Potassium replacement'.) <span>Although isotonic saline is often the initial replacement fluid used in treating diabetic ketoacidosis or nonketotic hyperglycemia, the addition of potassium will make this a hypertonic fluid (since potassium is as osmotically active as sodium), thereby delaying reversal of the hyperosmolality. Thus, 40 to 60 mEq of potassium per liter in one-half isotonic saline is preferred. (See "Diabetic ketoacidosis and hyperosmolar hyperglycemic state in adults: Treatment", section on 'Potassium replacement'.) In contrast to patients with marked potassium depletion, pat
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
mEq of potassium per liter in one-half isotonic saline is preferred. (See "Diabetic ketoacidosis and hyperosmolar hyperglycemic state in adults: Treatment", section on 'Potassium replacement'.) <span>In contrast to patients with marked potassium depletion, patients with hypokalemia due to potassium redistribution (eg, hypokalemic periodic paralysis) have no potassium deficit and even low rates of potassium administration can result in hyperkalemia once the redistributed potassium returns to the extracellular fluid. In a report of patients with hypokalemic thyrotoxic periodic paralysis (baseline serum potassium concentration 2.0 mEq/L), administration of potassium at a rate of 10 mEq/hour (80 mEq/L) resulted in hyperkalemia (>5.5 mEq/L) in 40 percent of patients, one-half of whom had ECG changes [30]. Appropriate therapy in these patients is discussed separately. (See "Hypokalemic periodic paralysis", section on 'Acute treatment' and "Thyrotoxic periodic paralysis", section on 'Acute treatment'.) Adverse effects of intravenous potassium — Pain
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ed separately. (See "Hypokalemic periodic paralysis", section on 'Acute treatment' and "Thyrotoxic periodic paralysis", section on 'Acute treatment'.) Adverse effects of intravenous potassium — <span>Pain and phlebitis can occur during parenteral infusion of potassium into a peripheral vein. This primarily occurs at rates above 10 mEq/hour, but can be seen at lower rates. If pain occurs, either the infusion rate or, preferably, the potassium concentration should be reduced. Another potential problem with administering high potassium concentrations in a single infusion container is inadvertent administration of a large amount of potassium in a short period
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ommended maximum rate of potassium administration is 10 to 20 mEq/hour in most patients. However, initial rates as high as 40 mEq/hour have been used for life-threatening hypokalemia [2,56-58]. <span>Rates above 20 mEq/hour are highly irritating to peripheral veins. Such high rates should be infused into a large central vein or into multiple peripheral veins. Potassium can be given intravenously via a peripheral or a large central vein. To decrease the risk of inadvertent administration of a large absolute amount of potassium, we suggest the
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
n result in severe hyperkalemia. The following recommended approach should minimize this risk, but careful monitoring is still required. (See 'Careful monitoring' below.) Recommended approach — <span>For patients with severe hypokalemia due to gastrointestinal or renal losses, the recommended maximum rate of potassium administration is 10 to 20 mEq/hour in most patients. However, initial rates as high as 40 mEq/hour have been used for life-threatening hypokalemia [2,56-58]. Rates above 20 mEq/hour are highly irritating to peripheral veins. Such high rat
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
advertent administration of a large absolute amount of potassium, we suggest the following maximum amounts of potassium that should be added to each particular sized infusion container [57,59]: <span>●In any 1000 mL-sized container of appropriate non-dextrose fluid, we suggest a maximum of 60 mEq of potassium. ●In a small-volume mini-bag of 100 to 200 mL of water that is to be infused into a peripheral vein, we suggest 10 mEq of potassium. ●In a small-volume mini-bag of 100 mL of water that is to be infused into a large central vein, we suggest a maximum of 40 mEq of potassium. Intravenous potassium is most often infused in a peripheral vein at concentrations of 20 to 60 mEq/L in a non-dextrose-containing saline solution. Use of an infusion pump is preferred t
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
o a peripheral vein, we suggest 10 mEq of potassium. ●In a small-volume mini-bag of 100 mL of water that is to be infused into a large central vein, we suggest a maximum of 40 mEq of potassium. <span>Intravenous potassium is most often infused in a peripheral vein at concentrations of 20 to 60 mEq/L in a non-dextrose-containing saline solution. Use of an infusion pump is preferred to prevent overly rapid potassium administration in any intravenous container with more than 40 mEq of potassium or if the desired rate of potassium administration is more than 10 mEq/hour. For patients with severe hypokalemia, administration in a large central vein is preferred if this access is available. Careful monitoring — Careful monitoring of the physiologic effects of severe hypokalemia (ECG abnormalities, muscle weakness, paralysis) is essential. Continuous ECG monitoring or telem
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Hypokaliémie : diagnostic et prise en charge - Revue Médicale Suisse
iologique n'est pas établi, la chimie urinaire ainsi que l'état acido-basique peuvent orienter vers un diagnostic précis. Dans chaque cas, un traitement étiologique est nécessaire. Introduction <span>L'hypokaliémie est définie comme une concentration plasmatique inférieure à 3,5 mmol/l. Il s'agit du trouble électrolytique le plus fréquent en pratique clinique. Il est présent chez 20% des patients hospitalisés et chez 10-40% des patients sous traitement de diurétiques thiazidiques.1,2 En général, une hypokaliémie discrète à modérée (3,0-3,5 mmol/l) est bien tolérée chez les personnes en bonne santé, toutefois elle peut être vitale surtout chez les patients avec un
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Hypokaliémie : diagnostic et prise en charge - Revue Médicale Suisse
it du trouble électrolytique le plus fréquent en pratique clinique. Il est présent chez 20% des patients hospitalisés et chez 10-40% des patients sous traitement de diurétiques thiazidiques.1,2 <span>En général, une hypokaliémie discrète à modérée (3,0-3,5 mmol/l) est bien tolérée chez les personnes en bonne santé, toutefois elle peut être vitale surtout chez les patients avec une pathologie cardiaque sous-jacente. Pour ces raisons, une approche étiologique et thérapeutique de l'hypokaliémie est importante. Concernant la régulation de la balance potassique, voir l'article sur l'hyperkaliémie dans
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Hypokaliémie : diagnostic et prise en charge - Revue Médicale Suisse
ulation de la balance potassique, voir l'article sur l'hyperkaliémie dans ce même numéro. Manifestations cliniques L'hypokaliémie est souvent découverte fortuitement lors d'un bilan biologique. <span>Lorsque l'hypokaliémie est modérée à sévère (3 à 2,5 mmol/l), elle peut s'accompagner de symptômes non spécifiques (faiblesse musculaire, myalgies, sensation de fatigue). Quand la kaliémie est inférieure à 2,0 mmol/l, on peut observer une atteinte musculaire avec rhabdomyolyse, tétraparésie, atteinte des fibres musculaires lisses avec iléus paralytique, rétention urinaire et finalement arrêt respiratoire. Les manifestations cardiaques sont les plus importantes car elles influencent le pronostic vital.3 En cas de pathologie cardiaque sous-jacente, une hypokaliémie discrète à modérée (3,0
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Hypokaliémie : diagnostic et prise en charge - Revue Médicale Suisse
usculaires lisses avec iléus paralytique, rétention urinaire et finalement arrêt respiratoire. Les manifestations cardiaques sont les plus importantes car elles influencent le pronostic vital.3 <span>En cas de pathologie cardiaque sous-jacente, une hypokaliémie discrète à modérée (3,0-3,5 mmol/l) peut quand même induire des arythmies cardiaques en relation avec la rapidité de son installation. L'augmentation du gradient transcellulaire de potassium entraîne une augmentation du potentiel de repos membranaire avec comme conséquences une augmentation de la durée du potentiel d'a
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Hypokaliémie : diagnostic et prise en charge - Revue Médicale Suisse
cas de pathologie cardiaque sous-jacente, une hypokaliémie discrète à modérée (3,0-3,5 mmol/l) peut quand même induire des arythmies cardiaques en relation avec la rapidité de son installation. <span>L'augmentation du gradient transcellulaire de potassium entraîne une augmentation du potentiel de repos membranaire avec comme conséquences une augmentation de la durée du potentiel d'action et de l'excitabilité myocardique (apparition d'une onde U). Les anomalies à l'ECG peuvent aller de l'onde U à des arythmies plus importantes (fibrillation auriculaire, extrasystoles, torsades de pointes et fibrillation ventriculaire).4 Certains auteurs préconisent de maintenir une kaliémie supérieure à 4,5 mmol/l chez les patients présentant une insuffisance cardiaque ou une cardiopathie ischémique.3 Causes d'hypoka
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Hypokaliémie : diagnostic et prise en charge - Revue Médicale Suisse
on d'une onde U). Les anomalies à l'ECG peuvent aller de l'onde U à des arythmies plus importantes (fibrillation auriculaire, extrasystoles, torsades de pointes et fibrillation ventriculaire).4 <span>Certains auteurs préconisent de maintenir une kaliémie supérieure à 4,5 mmol/l chez les patients présentant une insuffisance cardiaque ou une cardiopathie ischémique.3 Causes d'hypokaliémies L'hypokaliémie peut survenir soit par shift cellulaire, soit par des apports insuffisants ou finalement une augmentation des pertes (figure 1).5 Hypokaliémie sur
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Hypokaliémie : diagnostic et prise en charge - Revue Médicale Suisse
pertes (figure 1).5 Hypokaliémie sur shift cellulaire On connaît trois grandes causes de shift : les médicaments sont responsables d'une hypokaliémie sans modification du pool potassique total. <span>Les b2 mimétiques, la théophylline et la caféine entraînent une hypokaliémie par stimulation de la pompe Na+,K+,-ATPase. L'insuline augmente l'activité de la Na+,K+,-ATPase, provoquant une hypokaliémie transitoire lors de son administration chez les patients diabétiques, néanmoins cette hypokaliémie n'a pas de conséquences cliniques, sauf en cas d'intoxication à l'insuline et lors du traitement de l'acidocétose diabétique. Le vérapamil est le seul des anticalciques qui peut parfois être responsable d'une hypokaliémie modérée. Lors de l'hypokaliémie dans le contexte de l'alcalose métabolique et respiratoire, le shift cellulaire permet de garder l'électroneutralité intracellulaire. La paralysie périodique hyp
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Hypokaliémie : diagnostic et prise en charge - Revue Médicale Suisse
uf en cas d'intoxication à l'insuline et lors du traitement de l'acidocétose diabétique. Le vérapamil est le seul des anticalciques qui peut parfois être responsable d'une hypokaliémie modérée. <span>Lors de l'hypokaliémie dans le contexte de l'alcalose métabolique et respiratoire, le shift cellulaire permet de garder l'électroneutralité intracellulaire. La paralysie périodique hypokaliémique familiale est une affection génétique rare qui modifie la sensibilité au canal calcique, et est responsable d'hypokaliémies à la fin d'un effort
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Hypokaliémie : diagnostic et prise en charge - Revue Médicale Suisse
ponsable d'une hypokaliémie modérée. Lors de l'hypokaliémie dans le contexte de l'alcalose métabolique et respiratoire, le shift cellulaire permet de garder l'électroneutralité intracellulaire. <span>La paralysie périodique hypokaliémique familiale est une affection génétique rare qui modifie la sensibilité au canal calcique, et est responsable d'hypokaliémies à la fin d'un effort intense ou d'un repas riche en glucides. Le mécanisme n'est pas clairement établi.6 Lors de phénomènes d'anabolisme cellulaire comme lors de la correction d'une anémie mégaloblastique, on peut observer une hypokaliémie liée à l'utilisation du potassium dans la synthès
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Hypokaliémie : diagnostic et prise en charge - Revue Médicale Suisse
ue rare qui modifie la sensibilité au canal calcique, et est responsable d'hypokaliémies à la fin d'un effort intense ou d'un repas riche en glucides. Le mécanisme n'est pas clairement établi.6 <span>Lors de phénomènes d'anabolisme cellulaire comme lors de la correction d'une anémie mégaloblastique, on peut observer une hypokaliémie liée à l'utilisation du potassium dans la synthèse cellulaire. Diminution des apports en potassium Une diminution des apports potassiques à moins de 1g par jour, soit 25 mmol par jour, peut induire une hypokaliémie transitoire car l'adaptation rén
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Hypokaliémie : diagnostic et prise en charge - Revue Médicale Suisse
re comme lors de la correction d'une anémie mégaloblastique, on peut observer une hypokaliémie liée à l'utilisation du potassium dans la synthèse cellulaire. Diminution des apports en potassium <span>Une diminution des apports potassiques à moins de 1g par jour, soit 25 mmol par jour, peut induire une hypokaliémie transitoire car l'adaptation rénale n'est pas immédiate. C'est une cause inhabituelle d'hypokaliémie, mais elle peut être un facteur aggravant lors des pertes potassiques rénales ou digestives. L'anorexie ou une alimentation riche en hydrates
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Hypokaliémie : diagnostic et prise en charge - Revue Médicale Suisse
transitoire car l'adaptation rénale n'est pas immédiate. C'est une cause inhabituelle d'hypokaliémie, mais elle peut être un facteur aggravant lors des pertes potassiques rénales ou digestives. <span>L'anorexie ou une alimentation riche en hydrates de carbone associée à une consommation chronique d'alcool sont les causes principales d'hypokaliémie d'origine alimentaire. Pertes digestives de potassium La concentration de potassium dans les selles normales est environ 80 à 100 mmol/l et la perte quotidienne normale est de 10 mmol/l. Le potassium est sécr
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Hypokaliémie : diagnostic et prise en charge - Revue Médicale Suisse
ou une alimentation riche en hydrates de carbone associée à une consommation chronique d'alcool sont les causes principales d'hypokaliémie d'origine alimentaire. Pertes digestives de potassium <span>La concentration de potassium dans les selles normales est environ 80 à 100 mmol/l et la perte quotidienne normale est de 10 mmol/l. Le potassium est sécrété par l'épithélium colique. En cas de diarrhées, ou lors d'abus de laxatifs, l'augmentation du volume des selles peut provoquer une hypokaliémie parfois sévère. L
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Hypokaliémie : diagnostic et prise en charge - Revue Médicale Suisse
0 mmol/l. Le potassium est sécrété par l'épithélium colique. En cas de diarrhées, ou lors d'abus de laxatifs, l'augmentation du volume des selles peut provoquer une hypokaliémie parfois sévère. <span>Les vomissements peuvent également être responsables d'une hypokaliémie mais dont le mécanisme est d'origine rénale par alcalose métabolique de contraction et stimulation de la sécrétion d'aldostérone. Pertes rénales de potassium Les diurétiques sont la cause la plus fréquente d'hypokaliémie. L'incidence de l'hypokaliémie chez les patients âgés de plus de 70 ans sous traitement diuré
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Hypokaliémie : diagnostic et prise en charge - Revue Médicale Suisse
s sont la cause la plus fréquente d'hypokaliémie. L'incidence de l'hypokaliémie chez les patients âgés de plus de 70 ans sous traitement diurétique de l'anse ou thiazidique est de 20% à 40%.1,2 <span>Les diurétiques de l'anse agissent au niveau de la branche ascendante de Henle par inhibition du cotransporteur Na+-K+-2Cl- (NKCC2) et les diurétiques thiazidiques au niveau du tubule contourné distal par inhibition du cotransporteur Na+-Cl- (NCC1). La sécrétion de potassium dépend de la charge sodée au niveau distal, de l'aldostérone et du flux dans la lumière tubulaire. La kaliurie dans cette situation est donc élevée. Les diurétiques thiazidiques sont plus souvent associés à une hypokaliémie plus sévère que les diurétiques de l'anse.7 La pénicilline et ses dérivés, lorsqu'ils sont administrés par vo
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Hypokaliémie : diagnostic et prise en charge - Revue Médicale Suisse
ur Na+-Cl- (NCC1). La sécrétion de potassium dépend de la charge sodée au niveau distal, de l'aldostérone et du flux dans la lumière tubulaire. La kaliurie dans cette situation est donc élevée. <span>Les diurétiques thiazidiques sont plus souvent associés à une hypokaliémie plus sévère que les diurétiques de l'anse.7 La pénicilline et ses dérivés, lorsqu'ils sont administrés par voie intraveineuse à hautes doses, peuvent entraîner une perte rénale de potassium par augmentation du flux tubulaire dist
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Hypokaliémie : diagnostic et prise en charge - Revue Médicale Suisse
ns la lumière tubulaire. La kaliurie dans cette situation est donc élevée. Les diurétiques thiazidiques sont plus souvent associés à une hypokaliémie plus sévère que les diurétiques de l'anse.7 <span>La pénicilline et ses dérivés, lorsqu'ils sont administrés par voie intraveineuse à hautes doses, peuvent entraîner une perte rénale de potassium par augmentation du flux tubulaire distal. L'amphotéricine B augmente la perméabilité de la membrane apicale au potassium entraînant une hypokaliémie et une hypomagnésémie. Les troubles acido-basiques constituent également une cause d'hypokaliémie. En cas d'alcalose métabolique, on distingue celle à volume extracellulaire diminué (diurétiques, vomissements
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Hypokaliémie : diagnostic et prise en charge - Revue Médicale Suisse
ine B augmente la perméabilité de la membrane apicale au potassium entraînant une hypokaliémie et une hypomagnésémie. Les troubles acido-basiques constituent également une cause d'hypokaliémie. <span>En cas d'alcalose métabolique, on distingue celle à volume extracellulaire diminué (diurétiques, vomissements importants, sonde naso-gastrique, dérivations digestives hautes). La perte de chlore et la déplétion volémique sont à l'origine de l'hypokaliémie par stimulation du système rénine-angiotensine-aldostérone (hyperaldostéronisme secondaire). L'administration de chlore suffit en général à corriger la kaliémie : alcalose métabolique répondant au chlore.8 En cas de volume extracellulaire normal ou augmenté, on doit suspecter un hyperaldostéronisme primaire (syndrome de Conn) ou une sténose des artères rénales. Cette hypokaliémie ne répon
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Hypokaliémie : diagnostic et prise en charge - Revue Médicale Suisse
ion du système rénine-angiotensine-aldostérone (hyperaldostéronisme secondaire). L'administration de chlore suffit en général à corriger la kaliémie : alcalose métabolique répondant au chlore.8 <span>En cas de volume extracellulaire normal ou augmenté, on doit suspecter un hyperaldostéronisme primaire (syndrome de Conn) ou une sténose des artères rénales. Cette hypokaliémie ne répond pas au chlore mais au traitement de la pathologie de base.9,10 Certaines anomalies génétiques rares touchant le rein comme le syndrome de Liddle s'accompagnant d'une hypervolémie avec hypertension (mutation avec gain de fonction canal ENaC), ou le
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Hypokaliémie : diagnostic et prise en charge - Revue Médicale Suisse
doit suspecter un hyperaldostéronisme primaire (syndrome de Conn) ou une sténose des artères rénales. Cette hypokaliémie ne répond pas au chlore mais au traitement de la pathologie de base.9,10 <span>Certaines anomalies génétiques rares touchant le rein comme le syndrome de Liddle s'accompagnant d'une hypervolémie avec hypertension (mutation avec gain de fonction canal ENaC), ou le syndrome de Bartter (mutation du cotransporteur Na+-K+-2Cl- apical, canal K+ apical et canal Cl- basolatéral au niveau de l'anse de Henle) et le syndrome de Gittelman (mutation du cotransporteur Na+-Cl+ du contourné distal) s'accompagnant d'une contraction volémique sont également des causes d'hypokaliémie. L'acidose tubulaire distale (type I), proximale (type II) ou mixte (type III) figurent parmi les rares causes d'hypokaliémie associée à une acidose métabolique. Déplétion en magnésium L
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Hypokaliémie : diagnostic et prise en charge - Revue Médicale Suisse
eau de l'anse de Henle) et le syndrome de Gittelman (mutation du cotransporteur Na+-Cl+ du contourné distal) s'accompagnant d'une contraction volémique sont également des causes d'hypokaliémie. <span>L'acidose tubulaire distale (type I), proximale (type II) ou mixte (type III) figurent parmi les rares causes d'hypokaliémie associée à une acidose métabolique. Déplétion en magnésium La concentration de potassium intracellulaire est maintenue par la pompe Na+,K+,-ATPase. En cas d'hypomagnésémie, l'activité de la pompe est altérée et la concent
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Hypokaliémie : diagnostic et prise en charge - Revue Médicale Suisse
kaliémie. L'acidose tubulaire distale (type I), proximale (type II) ou mixte (type III) figurent parmi les rares causes d'hypokaliémie associée à une acidose métabolique. Déplétion en magnésium <span>La concentration de potassium intracellulaire est maintenue par la pompe Na+,K+,-ATPase. En cas d'hypomagnésémie, l'activité de la pompe est altérée et la concentration extracellulaire de potassium augmente avec comme conséquence une adaptation rénale sous la forme d'une kaliurèse accrue et une hypokaliémie secondaire. De plus, l'hypomagnésémie stimule le système rénine-angiotensine-aldostérone. Les aminoglycosides, le foscarnet et le cisplatine peuvent provoquer une déplétion en magnésium, et entraîner une hypokaliémie. Démarche diagnostique d'une hypokaliémie L'anamnèse, la prise de médicaments et l'évaluation du volume extracellulaire par un examen clinique minutieux sont essentielles dans la démarch
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Hypokaliémie : diagnostic et prise en charge - Revue Médicale Suisse
ngiotensine-aldostérone. Les aminoglycosides, le foscarnet et le cisplatine peuvent provoquer une déplétion en magnésium, et entraîner une hypokaliémie. Démarche diagnostique d'une hypokaliémie <span>L'anamnèse, la prise de médicaments et l'évaluation du volume extracellulaire par un examen clinique minutieux sont essentielles dans la démarche diagnostique d'une hypokaliémie. Si à ce stade, le diagnostic étiologique n'est pas établi, la chimie urinaire ainsi que l'état acido-basique vont nous orienter vers un diagnostic précis. La mesure du potassium urinair
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Hypokaliémie : diagnostic et prise en charge - Revue Médicale Suisse
arche diagnostique d'une hypokaliémie. Si à ce stade, le diagnostic étiologique n'est pas établi, la chimie urinaire ainsi que l'état acido-basique vont nous orienter vers un diagnostic précis. <span>La mesure du potassium urinaire sur un spot est alors utile. Lorsqu'il est inférieur à 20 mmol/l, ceci est compatible avec des pertes extrarénales de potassium, un shift cellulaire ou une diminution des apports alimentaires. Si l'excrétion urinaire de potassium est supérieure à 25 mmol/l, deux situations sont possibles. La première est représentée par le cas d'un hyperaldostéronisme secondaire sur hypovolé
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Hypokaliémie : diagnostic et prise en charge - Revue Médicale Suisse
ertes extrarénales de potassium, un shift cellulaire ou une diminution des apports alimentaires. Si l'excrétion urinaire de potassium est supérieure à 25 mmol/l, deux situations sont possibles. <span>La première est représentée par le cas d'un hyperaldostéronisme secondaire sur hypovolémie (diarrhées profuses). L'hypokaliémie est d'origine digestive mais la kaliurèse est haute en raison de la stimulation du système rénine-angiotensine-aldostérone. Dans la seconde, la kaliurèse haute signe l'origine rénale de l'hypokaliémie (syndrome de Conn, tubulopathies). La mesure du chlore urinaire permet de différencier ces deux possibilités. En cas d'hypovolémie, le chlore urinaire est bas. Traitement de l'hypokaliémie Le traitement de l'hypokaliémie comprend la prise en charge de la cause sous-jacente et la substitution en potassium. A l'exception des shifts où l'hypokali
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Hypokaliémie : diagnostic et prise en charge - Revue Médicale Suisse
ente et la substitution en potassium. A l'exception des shifts où l'hypokaliémie est transitoire, le traitement consiste en l'apport de potassium pour corriger les pertes rénales ou digestives. <span>La décision de corriger rapidement une hypokaliémie dépend du status clinique, des comorbidités et de la sévérité de l'hypokaliémie. Chez les patients asymptomatiques, avec une hypokaliémie modérée sans antécédent cardiaque, un régime riche en potassium suffit en général. En cas de persistance de l'hypokaliémie, une
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Hypokaliémie : diagnostic et prise en charge - Revue Médicale Suisse
avec une hypokaliémie modérée sans antécédent cardiaque, un régime riche en potassium suffit en général. En cas de persistance de l'hypokaliémie, une substitution médicamenteuse est nécessaire. <span>On estime que pour chaque augmentation de 0,3 mmol/l de la kaliémie, il est nécessaire d'administrer 100 mmol de potassium sous forme de chlorure de potassium.11,12 En cas d'hypokaliémie sévère, ou symptomatique, l'administration de potassium par voie intraveineuse est nécessaire. Elle ne doit pas dépasser les 20 mmol/h et sous surveillance rythmiq
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Hypokaliémie : diagnostic et prise en charge - Revue Médicale Suisse
dicamenteuse est nécessaire. On estime que pour chaque augmentation de 0,3 mmol/l de la kaliémie, il est nécessaire d'administrer 100 mmol de potassium sous forme de chlorure de potassium.11,12 <span>En cas d'hypokaliémie sévère, ou symptomatique, l'administration de potassium par voie intraveineuse est nécessaire. Elle ne doit pas dépasser les 20 mmol/h et sous surveillance rythmique.12 En cas de perfusion par voie périphérique, l'administration maximale est de 40 mmol par litre de solution. La kaliémie doit être régulièrement contrôlée pour éviter un phénomène de rebond. Une substitution en magnésium est souhaitée en cas d'hypokaliémie sévère. Conclusion En résumé, l'hypo
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Hypokaliémie : diagnostic et prise en charge - Revue Médicale Suisse
e.12 En cas de perfusion par voie périphérique, l'administration maximale est de 40 mmol par litre de solution. La kaliémie doit être régulièrement contrôlée pour éviter un phénomène de rebond. <span>Une substitution en magnésium est souhaitée en cas d'hypokaliémie sévère. Conclusion En résumé, l'hypokaliémie reste un trouble électrolytique fréquent en pratique clinique souvent découvert fortuitement lors du bilan biologique. Malgré le fait qu'elle soit
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 6262064811276
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262068481292
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262071889164
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262175960332
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262177008908
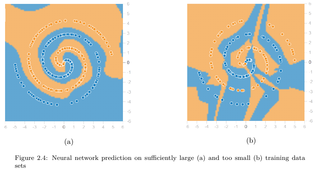
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262178319628
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262183562508
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262186970380
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262189067532
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262190902540
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262192737548
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262194572556
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262196407564
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262198242572
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262201650444
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262202174732
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262206893324
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262207417612
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262211349772
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262215544076
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262216068364
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262222359820
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262223408396

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262226029836
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262230224140
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262232845580
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262234680588
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262236515596
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262238350604
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262240185612
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262242020620
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262245428492
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262253817100
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262257224972
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6262260632844
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |