Edited, memorised or added to reading queue
on 11-Apr-2021 (Sun)
Do you want BuboFlash to help you learning these things? Click here to log in or create user.
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
English to Hindi Transliterate
ree legal aid, by suitable legislation or schemes or in any other way, to ensure that opportunities for securing justice are not denied to any citizen by reason of economic or other disability. <span>Articles 14 and 22(1) also make it obligatory for the State to ensure equality before law and a legal system which promotes justice on a basis of equal opportunity to all. Legal aid strives to ensure that constitutional pledge is fulfilled in its letter and spirit and equal justice is made available to the poor, downtrodden and weaker sections of the society. National Legal Services Authority The National Legal Services Authority (NALSA) has been constituted under the Legal Services Authorities Act, 1987 to provide free Legal Services to the
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
English to Hindi Transliterate
ok Adalats in the State. The State Legal Services Authority is headed by Hon’ble the Chief Justice of the respective High Court who is the Patron-in-Chief of the State Legal Services Authority. <span>In every District, District Legal Services Authority has been constituted to implement Legal Services Programmes in the District. The District Legal Services Authority is situated in the District Courts Complex in every District and chaired by the District Judge of the respective district. Free Legal Services offe
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
English to Hindi Transliterate
at constitutional pledge is fulfilled in its letter and spirit and equal justice is made available to the poor, downtrodden and weaker sections of the society. National Legal Services Authority <span>The National Legal Services Authority (NALSA) has been constituted under the Legal Services Authorities Act, 1987 to provide free Legal Services to the weaker sections of the society and to organize Lok Adalats for amicable settlement of disputes. NALSA is located at New Delhi. In every State, State Legal Services Authority has been constituted to give effect to the policies and directions of the NALSA and to give free legal serv
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
English to Hindi Transliterate
constituted under the Legal Services Authorities Act, 1987 to provide free Legal Services to the weaker sections of the society and to organize Lok Adalats for amicable settlement of disputes. <span>NALSA is located at New Delhi. In every State, State Legal Services Authority has been constituted to give effect to the policies and directions of the NALSA and to give free legal services to the people and conduct Lok Adalats in the State. The State Legal Services Authority is headed by Hon’ble the Chief Justice of the respective High Court who is the Patron-in-Chief of the State Legal Services Authority. In every District, District Legal Services Authority has been constituted to implement Legal Services Programmes in the District. The District Legal Services Authority is situated in th
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
English to Hindi Transliterate
criminal matters for those poor and marginalized people who cannot afford the services of a lawyer for the conduct of a case or a legal proceeding in any court, tribunal or before an authority. <span>Provision of free legal aid may include: Payment of court fee, process fees and all other charges payable or incurred in connection with any legal proceedings; Providing Advocate in a legal proceedings; Obtaining and supply of certified copies of orders and other documents in legal proceedings. Preparation of appeal, paper book including printing and translation of documents in legal proceedings. Rendering of any service in the conduct of any case or other legal proceeding before any court or other Authority or tribunal. Giving of advice on any legal matter. Eligible persons for getting free legal services The sections of the society as enlisted under Section 12 of the Legal Services Authorities Act are entitled for free legal services, the
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
English to Hindi Transliterate
rm available online at NALSA’s website. To access the online application, click here . Various SLSAs/DLSAs/SCLSC/HCLSCs/TLSCs also have application forms available on their websites. Lok Adalat <span>Lok Adalat is a forum where the disputes/cases pending in the court of law or at pre-litigation stage are settled/compromised amicably. The Lok Adalat has been given statutory status under the Legal Services Authorities Act, 1987. Under the said Act, the award made by the Lok Adalats is deemed to be the decree of a civil court and is final and binding on all parties and no appeal lies before any court against its
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Lok Adalat - National Legal Services Authority!
he weaker sections and interested in the implementation of legal services schemes or programmes or a person engaged in para-legal activities of the area, preferably a woman. National Lok Adalat <span>National Level Lok Adalats are held for at regular intervals where on a single day Lok Adalats are held throughout the country, in all the courts right from the Supreme Court till the Taluk Levels wherein cases are disposed off in huge numbers. From February 2015, National Lok Adalats are being held on a specific subject matter every month. Permanent Lok Adalat The other type of Lok Adalat is the Permanent Lok Adalat, organize
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Lok Adalat - National Legal Services Authority!
intervals where on a single day Lok Adalats are held throughout the country, in all the courts right from the Supreme Court till the Taluk Levels wherein cases are disposed off in huge numbers. <span>From February 2015, National Lok Adalats are being held on a specific subject matter every month. Permanent Lok Adalat The other type of Lok Adalat is the Permanent Lok Adalat, organized under Section 22-B of The Legal Services Authorities Act, 1987. Permanent Lok Adalats have been
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Lok Adalat - National Legal Services Authority!
s in such a manner as it considers appropriate, taking into account the circumstances of the case, wishes of the parties like requests to hear oral statements, speedy settlement of dispute etc. <span>Mobile Lok Adalats are also organized in various parts of the country which travel from one location to another to resolve disputes in order to facilitate the resolution of disputes through this mechanism. As on 30.09.2015, more than 15.14 lakhs Lok Adalats have been organized in the country since its inception. More than 8.25 crore cases have been settled by this mechanism so far. RTI Br
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Lok Adalat - National Legal Services Authority!
ph etc. Here, even if the parties fail to reach to a settlement, the Permanent Lok Adalat gets jurisdiction to decide the dispute, provided, the dispute does not relate to any offence. Further, <span>the Award of the Permanent Lok Adalat is final and binding on all the parties. The jurisdiction of the Permanent Lok Adalats is upto Rs. Ten Lakhs. Here if the parties fail to reach to a settlement, the Permanent Lok Adalat has the jurisdiction to decide the case. The award of the Permanent Lok Adalat is final and binding upon the parties. The Lok Adalat may conduct the proceedings in such a manner as it considers appropriate, taking into account
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Lok Adalat - National Legal Services Authority!
arties. The jurisdiction of the Permanent Lok Adalats is upto Rs. Ten Lakhs. Here if the parties fail to reach to a settlement, the Permanent Lok Adalat has the jurisdiction to decide the case. <span>The award of the Permanent Lok Adalat is final and binding upon the parties. The Lok Adalat may conduct the proceedings in such a manner as it considers appropriate, taking into account the circumstances of the case, wishes of the parties like requests to hear o
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Lok Adalat - National Legal Services Authority!
h matter to the Lok Adalat for amicable settlement of the dispute for which notice would then be issued to the other party. Levels and Composition of Lok Adalats: At the State Authority Level - <span>The Member Secretary of the State Legal Services Authority organizing the Lok Adalat would constitute benches of the Lok Adalat, each bench comprising of a sitting or retired judge of the High Court or a sitting or retired judicial officer and any one or both of- a member from the legal profession; a social worker engaged in the upliftment of the weaker sections and interested in the implementation of legal services schemes or programmes. At High Court Level - The Secretary of the High Court Legal Services Committee would constitute benches of the Lok Adalat, each bench comprising of a sitting or retired judge of the Hig
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Decriminalisation Of Compoundable Offences - Coronavirus (COVID-19) - India
fender is given an option to pay money in lieu of his prosecution to avoid prolonged litigation. Section 441 of the Act, provides for the provisions pertaining to the compounding of an offence. <span>There is no specific definition of the word “compounding” provided in the Act, however legal meaning of compounding can be referred to as doing good the default or non-compliance. Generally, compoundable offences are those which can be settled by paying a certain amount of money. THE REVIEW COMMITTEE The roots of necessity to decriminalize certain compoundable offences are elevated from the Ministry of Corporate Affairs (MCA) vide order dated 13.07.2018, wherein
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Decriminalisation Of Compoundable Offences - Coronavirus (COVID-19) - India
(the Act). The Government of India is initiating various relief packages, to provide aid to the companies to ease their working during the current pandemic, which the world is facing at large. <span>When a company contravenes specific provisions of the said Act, by doing something which is barred, restricted or prohibited under the Act, then such a behaviour performed by the company is treated as an offence under the Act. Such offences can be treated as Compoundable and Non-Compoundable Offences. The Government of India has announced to decriminalize certain offences which are compoundable in nature, to reduce the burden of compliance on the companies under various provisions of
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
English to Hindi Transliterate
before the court Provided that any matter relating to an offence not compoundable under the law shall not be settled in Lok Adalat. How to get the case referred to the Lok Adalat for settlement <span>A) Case pending before the court: If the parties agree to settle the dispute in Lok Adalat or One of the parties makes an application to the court or The court is satisfied that that the matter is an appropriate one for settlement in Lok Adalat B. Any dispute at pre-litigative stage The State Legal Services Authority or District Legal Services Authority as the case may be on receipt of an application from any one of the parties to any pre-litigation stage matter refer such matter to the Lok Adalat for amicable settlement. Websites of State Legal Services Authority ANDAMAN AND NICOBAR ANDHRA PRADESH ARUNACHAL PRADESH ASSAM BIHAR CHANDIGARH CHHATTISGARH DADRA AND NAGAR HAVELI DAMAN AND DIU DELHI GOA GUJARA
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
re no symptom-specific data about the prevalence of this problem in ambulatory patients, the epidemiology of cardiac and pulmonary diseases indicates that the magnitude of the problem is large. <span>Cardiac disease is the leading cause of death in the United States, and individuals with angina or myocardial infarction often experience breathlessness as the major (and sometimes sole) indicator that they are ill [1]. In addition, asthma and chronic obstructive pulmonary disease (COPD) afflict approximately 34 million people in the United States, most of whom seek help from clinicians for relief of
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
asthma and chronic obstructive pulmonary disease (COPD) afflict approximately 34 million people in the United States, most of whom seek help from clinicians for relief of breathlessness [2,3]. <span>Data from patients admitted to the hospital suggest that 16 percent of patients suffer from dyspnea within 24 hours of admission [4]. The pathophysiology of dyspnea will be reviewed here. Factors affecting the control of ventilation and disorders of ventilation, and an approach to a patient with dyspnea, are presented
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
qualitatively distinct sensations, and that the words utilized by patients to describe their breathing discomfort may provide insights into the underlying pathophysiology of the disease [5-8]. <span>Furthermore, there is a growing recognition that one must distinguish between a "sensation" (the neural activation resulting from the stimulation of a receptor) and a "perception" (the reaction of the individual to that sensation) [9-11] and that healthcare providers are relatively poor at estimating the intensity of dyspnea by observing patients [12,13]. In addition, for a given intensity of a breathing sensation, the unpleasantness of the sensation may vary with the stimulus [14]. A consensus statement of the American Thoracic Society
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
inadequate delivery of oxygen to, or utilization by, peripheral muscles are less well understood, but are felt to be related to stimulation of metaboreceptors and deserve consideration as well. <span>INCREASED OUTPUT FROM THE RESPIRATORY CENTERS — Most conditions that are associated with respiratory discomfort are characterized by increases in ventilation in response to derangements in ventilation-perfusion matching, increases in dead space, the presence of metabolic acidosis, or stimulation of pulmonary or chest wall receptors. For many years it was believed that this increase in stimulation of the respiratory centers and the resultant augmentation of activity of the ventilatory muscles was responsible for dyspnea. However, subsequent data suggest that the intensity of respiratory discomfort for a given level of ventilation may vary considerably depending upon the nature of the stimulus giving rise to the hyperpnea, and that stimulation of chemoreceptors can produce dyspnea even in the absence of activation of the respiratory muscles (figure 1). Chemoreceptors — The peripheral chemoreceptors, located in the carotid bodies and aortic arch, sense changes in the partial pressure of oxygen in arterial blood and are also stimulated
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
upon the nature of the stimulus giving rise to the hyperpnea, and that stimulation of chemoreceptors can produce dyspnea even in the absence of activation of the respiratory muscles (figure 1). <span>Chemoreceptors — The peripheral chemoreceptors, located in the carotid bodies and aortic arch, sense changes in the partial pressure of oxygen in arterial blood and are also stimulated by acidosis and hypercapnia. The central chemoreceptors, located in the medulla, respond to changes in pH and arterial tension of carbon dioxide (PaCO2). Acute hypercapnia is generally a much stronger stimulus for respiratory discomfort than is acute hypoxemia. (See "Control of ventilation".) Acute hypercapnia — While acute hypercapnia typically leads to brisk increases in ventilation, dyspnea can result from hypercapnia among ventilator-depen
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
a can result from hypercapnia among ventilator-dependent C1-2 quadriplegics who lack functioning respiratory muscles and in normal subjects paralyzed with neuromuscular blocking agents [15,16]. <span>In a different experimental model, normal subjects maintaining a targeted ventilation experienced greater dyspnea when made hypercapnic than when eucapnic conditions were maintained [17]. These results are consistent with the notion that there are direct projections from the brainstem chemoreceptors to the sensory cortex, ie, there is a "corollary discharge" or neural discharge to the sensory cortex that is generated simultaneously with and in proportion to the brainstem neural output to the respiratory muscles [18]. Evidence that one can experience some form of dyspnea in the absence of functioning central chemoreceptors is provided by studies of individuals with congenital central hypoventilation
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
here is a "corollary discharge" or neural discharge to the sensory cortex that is generated simultaneously with and in proportion to the brainstem neural output to the respiratory muscles [18]. <span>Evidence that one can experience some form of dyspnea in the absence of functioning central chemoreceptors is provided by studies of individuals with congenital central hypoventilation syndrome [19]. Many of these individuals breathe relatively normally when awake but have cessation of breathing and respiratory arrest when they are asleep and must be maintained on mechanical ventilation while sleeping. Although they do not increase ventilation or become dyspneic with acute hypercapnia, exercise hyperpnea and breathing discomfort with exercise persist. (See 'Impaired oxygen delivery or utilization' below.) Acute hypoxemia — Acute hypoxemia is also associated with increases in ventilation and respiratory discomfort. While the data supp
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
do not increase ventilation or become dyspneic with acute hypercapnia, exercise hyperpnea and breathing discomfort with exercise persist. (See 'Impaired oxygen delivery or utilization' below.) <span>Acute hypoxemia — Acute hypoxemia is also associated with increases in ventilation and respiratory discomfort. While the data supporting a direct role for hypoxic stimulation of chemoreceptors in the production of dyspnea are less clear than with hypercapnia, it seems likely that hypoxemia can produce breathing discomfort independently of changes in ventilation. As examples: ●Subjects exercising under hypoxic conditions experience more dyspnea than when performing the same activity while breathing room air, and less dyspnea when breathing 100 p
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
with greater breathing discomfort than comparable degrees of ventilation resulting from exercise [22], demonstrating an effect of hypoxemia on dyspnea that is independent of minute ventilation. <span>Nonetheless, hypoxemia alone or in the setting of minimal underlying cardiopulmonary abnormalities is a relatively weak stimulus for dyspnea; misunderstanding of this phenomenon may explain the notion of the "happy hypoxemic" patient with mild coronavirus disease 2019 (COVID-19) [23]. In addition, it is common that patients with hypoxemia and severe lung disease may experience little improvement of dyspnea despite administration of supplemental oxygen. STIMULATION OF MECHANORECEPTORS — Throughout the airways, lungs, and chest wall are a variety of receptors that assist the body in monitoring changes in pressure, flow, and volume in th
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
2019 (COVID-19) [23]. In addition, it is common that patients with hypoxemia and severe lung disease may experience little improvement of dyspnea despite administration of supplemental oxygen. <span>STIMULATION OF MECHANORECEPTORS — Throughout the airways, lungs, and chest wall are a variety of receptors that assist the body in monitoring changes in pressure, flow, and volume in the respiratory system. Information from these receptors is integrated by the central nervous system in a manner that modulates the intensity of dyspnea. However, in some cases, most notably the "chest tightness" associated with bronchoconstriction, the receptors may be the primary source of the sensation [24,25]. Upper airway receptors — Stimulation of receptors in the face and upper airway, which are largely innervated by the trigeminal nerve, can reduce the intensity of dyspnea. As examples, c
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
lates the intensity of dyspnea. However, in some cases, most notably the "chest tightness" associated with bronchoconstriction, the receptors may be the primary source of the sensation [24,25]. <span>Upper airway receptors — Stimulation of receptors in the face and upper airway, which are largely innervated by the trigeminal nerve, can reduce the intensity of dyspnea. As examples, cold air directed against the face increases breathholding time and reduces the respiratory discomfort associated with breathing against an inspiratory load [26,27]. Presumed stimulation of flow or temperature receptors by the inhalation of cold air reduces exertional dyspnea and ventilation in patients with chronic obstructive pulmonary disease (COPD), while reductions in upper airway receptor stimulation achieved with topical lidocaine or by the inhalation of warm, humidified air worsen respiratory discomfort in normal subjects [28,29]. High-flow nasal oxygen has been shown to reduce dyspnea to a greater degree than standard supplemental oxygen therapy [30], presumably because of greater stimulation of nasal receptors. Pulmonary receptors — The lung is populated by three major categories of receptors that transmit information relevant to respiratory sensation to the central nervous system via the vagu
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
28,29]. High-flow nasal oxygen has been shown to reduce dyspnea to a greater degree than standard supplemental oxygen therapy [30], presumably because of greater stimulation of nasal receptors. <span>Pulmonary receptors — The lung is populated by three major categories of receptors that transmit information relevant to respiratory sensation to the central nervous system via the vagus nerve: ●Slowly adapting receptors, also known as pulmonary stretch receptors, are activated by an increase in tension in the walls of airways, thereby providing information about increases in lung volume. ●Rapidly adapting receptors or irritant receptors are stimulated by rapid changes in lung volume, direct mechanical stimuli, or inhalation of irritant particulate matter or chemicals such as histamine. ●C-fibers are unmyelinated afferent nerve fibers that originate in J-receptors located in small airways and near alveolar capillaries; they are stimulated by mechanical and chemical factors. The configuration of these receptors is such that limitations of the movement of the respiratory system exacerbate dyspnea in a variety of experimental conditions, including breathholdi
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
e. ●C-fibers are unmyelinated afferent nerve fibers that originate in J-receptors located in small airways and near alveolar capillaries; they are stimulated by mechanical and chemical factors. <span>The configuration of these receptors is such that limitations of the movement of the respiratory system exacerbate dyspnea in a variety of experimental conditions, including breathholding and acute hypercapnia [31-33]. Restriction of tidal volume associated with hyperinflation may also contribute to the discomfort experienced by patients with emphysema [34]. Inhaled furosemide is hypothesized to stimulate pulmonary stretch receptors. It has been shown to reduce dyspnea in healthy subjects in whom dyspnea was induced using a large resistive
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
luding breathholding and acute hypercapnia [31-33]. Restriction of tidal volume associated with hyperinflation may also contribute to the discomfort experienced by patients with emphysema [34]. <span>Inhaled furosemide is hypothesized to stimulate pulmonary stretch receptors. It has been shown to reduce dyspnea in healthy subjects in whom dyspnea was induced using a large resistive load plus hypercapnia [35]. Similarly, dyspnea associated with acute hypercapnia and a restricted tidal volume, as well as the breathlessness associated with exercise, is ameliorated by inhaled furosemide [36,37]. More controlled administration of inhaled furosemide with a similar model of producing dyspnea with hypercapnia and restricted tidal volume, however, resulted in a highly variable response among individuals and group differences compared with placebo are not significant [38,39]. Stimulation of pulmonary receptors may provoke the dyspnea of asthma. While the work of breathing is increased in patients with acute bronchoconstriction due to changes in airways resis
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
a is greater with acute bronchoconstriction than with external resistive loads at comparable degrees of airway resistance [24,25], and the quality of the discomfort is different [5,6,24,25,40]. <span>Breathing against an external load leads to a sensation of increased "effort" or "work" of breathing, while acute bronchospasm is associated with a sensation of "chest tightness or constriction." Furthermore, the inhalation of lidocaine appears to blunt the dyspnea of bronchoconstriction, consistent with the hypothesis that stimulation of pulmonary receptors is contributing to the breathing discomfort [24]. Activation of pulmonary receptors may also play a role in the dyspnea of acute pulmonary embolism [41]. Chest wall receptors — Information from muscle spindles and tendon organs within the chest wall is also important to the perception of dyspnea. Muscle spindles function as length or str
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
inspiratory muscles during expiration, heightens the intensity of dyspnea [45]. It is important to note that the vibration used in these studies might also have stimulated pulmonary receptors. <span>While stimulation of chest wall receptors likely plays a role in the detection of changes in thoracic expansion, pulmonary receptors are sufficient to monitor lung volume. Patients with cervical spinal cord injury, for example, in whom information from chest wall receptors is interrupted before reaching the brain, can detect small changes in tidal volume and experience respiratory discomfort when tidal volumes are reduced [46,47]. MECHANICAL LOADING OF THE RESPIRATORY SYSTEM — A wide variety of cardiopulmonary diseases are associated with an increased mechanical load due to changes in airways resistance (eg, asth
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
nce (eg, idiopathic pulmonary fibrosis, kyphoscoliosis). To achieve a given tidal volume under these conditions, the brain must generate a greater neural output to the ventilatory muscles [48]. <span>Outgoing motor commands to the ventilatory muscles probably are associated with a corollary discharge to the sensory cortex, which is perceived as a "sense of effort" [49]. The sense of effort appears to be a function of the ratio of the pressure generated by the ventilatory muscles on a given breath to the maximal pressure achievable by the muscles [50]. Thus, the sense of effort may increase because there is an obstruction to flow and the intrathoracic pressure generated on each breath is high, or because the pressure-generating capacity of the muscles is reduced, as is seen in the presence of muscle fatigue, myopathy, or hyperinflation. Normal subjects maintaining a constant ventilatory target experience less effort but more dyspnea when hypercapnic than eucapnic [17], suggesting that ventilation arising from "automati
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
will not shorten appropriately for the tension being generated, intrathoracic pressures will be less negative than normal, inspiratory flow will be reduced, and tidal volume will be diminished. <span>Although the exact means by which the body makes the comparison between what is expected under normal conditions for a given efferent message and the actual outcome of that message remains unclear, the mismatch between the two (termed "efferent-reafferent dissociation" [51] or "neuromechanical dissociation" [52]) appears to worsen the intensity of dyspnea. This mechanism may in part explain the dyspnea associated with experimentally constrained ventilation [32,33], hyperinflation in COPD [34,52,53], hyperinflation in asthma [54], and in s
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
UTILIZATION — Anemia and cardiovascular deconditioning are two common clinical conditions that are associated with exertional dyspnea and do not readily fit into the categories outlined above. <span>Anemia — Patients with moderate to severe anemia typically experience breathing discomfort with light exercise despite the absence of a gas exchange abnormality or mechanical loading of the respiratory system. The response of the body to the reduced oxygen-carrying capacity of the blood is to increase cardiac output. This may necessitate an increase in left ventricular end-diastolic pressure with consequent increases in pulmonary venous pressures, the development of interstitial edema, and stimulation of C-fibers. However, tachycardia, rather than increased stroke volume, is often the first response of the cardiovascular system, and it is unclear to what extent intracardiac and pulmonary vascular pressures rise in this setting. An alternative explanation is that the reduced delivery of oxygen to the metabolically active muscles may lead to the development of a localized metabolic acidosis and the stimulation o
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
rate a greater cardiac output and by inducing capillary growth and enzyme changes in skeletal muscle to improve the delivery of oxygen and efficiency of oxygen use. (See "Exercise physiology".) <span>Many patients with chronic lung disease assume a sedentary lifestyle and become deconditioned; functional capabilities may be determined more by their level of fitness than by their underlying respiratory illness [60]. Dyspnea on exertion in these individuals may result primarily from reliance on anaerobic metabolism at low levels of exercise, development of a metabolic acidosis, and increased neural output from the respiratory centers. Whether the development of localized acidosis and stimulation of ergoreceptors also play a role in this situation remains uncertain. In addition, for some patients with chronic diseases that impair their functional capacity leading to a very limited lifestyle, normal increases in ventilation with exercise may be perceived as pathologic, ie, they become sensitized to dyspneic stimuli. NEURAL ACTIVATION ASSOCIATED WITH BREATHING DISCOMFORT — Investigators have begun to employ positron emission tomography and magnetic resonance imaging as tools to localize regions of t
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
t the emotional response to a stimulus that produces dyspnea varies and may be responsible, in part, for the different experiences and reports of the severity of dyspnea by patients [14,65,66]. <span>Furthermore, higher degrees of dyspnea-related fear may predict response to pulmonary rehabilitation in patients with chronic obstructive pulmonary disease (COPD) [67]. For the same degree of sensory discomfort, air hunger results in greater fear and anxiety than increased work of breathing [14]. SOCIETY GUIDELINE LINKS — Links to society and government-sponsored guidelines from selected countries and regions around the world are provided separately. (See "Society guideline link
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
opics are updated as new evidence becomes available and our peer review process is complete. Literature review current through: Mar 2021. | This topic last updated: Jun 26, 2019. INTRODUCTION — <span>The respiratory system is dependent upon adequate ventilation to supply oxygen, remove carbon dioxide, and help maintain acid-base homeostasis. Ventilation responds to changes in the arterial carbon dioxide tension (PaCO2), arterial oxygen tension (PaO2), and pH (figure 1), and may be modified in response to a number of mechanical and irritant stimuli arising from various structures within the thoracic cage, and probably from within muscles and joints during exercise. Broadly viewed, the respiratory control mechanisms respond to input from neural and chemical receptors. Respiratory centers in the brain integrate these inputs and provide neuronal driv
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
dins, and exogenous noxious agents. The C-fiber (ie, small diameter, unmyelinated sensory afferent fibers) endings in the airways and lung respond primarily to their local chemical environment. <span>Activation of these receptors and fibers signals the respiratory centers via the vagus nerve and affects the breathing pattern by increasing the respiratory rate and/or stimulating cough, bronchoconstriction, and mucus production. Input from these neural receptors likely accounts for the hyperventilation and hypocapnia that can occur in patients with pulmonary fibrosis even when hypoxemia is reversed by the administration of oxygen [4]. Hyperventilation may occur by this mechanism in patients with such problems as asthma, interstitial lung disease, pulmonary edema, pneumonia, and pulmonary embolism. PERIPHERAL CHEMORECEPTORS — The peripheral chemoreceptors, including the carotid and aortic bodies, are the primary sites for sensing the partial pressure of arterial oxygen (PaO2), but
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
Hyperventilation may occur by this mechanism in patients with such problems as asthma, interstitial lung disease, pulmonary edema, pneumonia, and pulmonary embolism. PERIPHERAL CHEMORECEPTORS — <span>The peripheral chemoreceptors, including the carotid and aortic bodies, are the primary sites for sensing the partial pressure of arterial oxygen (PaO2), but they also increase their discharge in response to hypercapnia or acidosis. The carotid chemoreceptors are more important in adults; aortic chemoreceptors are active in infancy and childhood and then become relatively quiescent [5]. Neural outflow from the carotid bodies is estimated to account for up to 15 percent of resting ventilation, since peripheral chemodenervation leads to a rise in partial pressure of arterial carbon dioxide (PCO2) of 5 to 10 mmHg [6,7]. The carotid bodies are located at the bifurcation of the common carotid arteries. Carotid body neuronal discharge increases as PaO2 falls below 75 mmHg and becomes marked and progressiv
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
estimated to account for up to 15 percent of resting ventilation, since peripheral chemodenervation leads to a rise in partial pressure of arterial carbon dioxide (PCO2) of 5 to 10 mmHg [6,7]. <span>The carotid bodies are located at the bifurcation of the common carotid arteries. Carotid body neuronal discharge increases as PaO2 falls below 75 mmHg and becomes marked and progressive when PaO2 is less than 50 to 55 mmHg [8]. The response of the carotid bodies to the combination of hypoxemia and hypercapnia is greater than the sum of the individual responses to each component. Carotid body resection leads to reduced hypoxic ventilatory response and to hypercapnia. (See "Disorders of ventilatory control", section on 'Cheyne-stokes respiration'.) S-Nitrosothiols (SNOs) are thought to have a crucial role in signaling in the respiratory system includ
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ses to each component. Carotid body resection leads to reduced hypoxic ventilatory response and to hypercapnia. (See "Disorders of ventilatory control", section on 'Cheyne-stokes respiration'.) <span>S-Nitrosothiols (SNOs) are thought to have a crucial role in signaling in the respiratory system including hypoxic ventilator drive [9]. Hypoxia leads to S-nitrosylation of Cystine thiols of certain proteins and peptides in red blood cells leading to S-nitrosothiols, which then activate carotid body cells. Impulses from the carotid bodies travel through the IX cranial nerve to the nucleus tractus solitarius (NTS), where excitatory neurotransmitters are released that result in increased ventilation [10]. Systemic N-acetylcysteine increases hypoxic ventilatory drive, likely acting via its effect on hemoglobin SNO [11]. There may be other, undefined peripheral receptors which help regulat
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
xture; however, they increase their ventilation and maintain their pre-existing PCO2 levels during exercise, and have a fall in PCO2 during passive leg cycling [14,15]. CENTRAL CHEMORECEPTORS — <span>Central nervous system (CNS) chemoreceptors have the major role in adjusting ventilation to maintain acid-base homeostasis. These receptors respond vigorously and almost instantaneously to changes in pH of the CNS environment. Several chemoreceptor sites have been identified in the medulla and mid-brain, the most significant ones being near the ventral surface of the medulla (VMS) and near the retrotrapezoid nucleus (RTN). RTN neurons receive input from carotid body chemoreceptors, and also express high levels of Phox2b, mutations of which are the cause of congenital central hypoventilation syndrome (CCHS) [16]. Acetylcholine and the parasympathetic nervous system play a major role determining the response to CO2 stimulation, and probably contribute to normal central rhythm generation [10]. Con
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
RTN neurons receive input from carotid body chemoreceptors, and also express high levels of Phox2b, mutations of which are the cause of congenital central hypoventilation syndrome (CCHS) [16]. <span>Acetylcholine and the parasympathetic nervous system play a major role determining the response to CO2 stimulation, and probably contribute to normal central rhythm generation [10]. Congenital central hypoventilation syndrome has nearly absent ventilatory response to hypoxia and hypercapnia, is associated with Hirschsprung's disease, and usually requires ventilatory support. (See "Disorders of ventilatory control", section on 'Congenital central hypoventilation syndrome' and "Congenital central hypoventilation syndrome and other causes of sleep-related hypo
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ventilation syndrome' and "Congenital central hypoventilation syndrome and other causes of sleep-related hypoventilation in children", section on 'Congenital central hypoventilation syndrome'.) <span>Because CO2 is lipid-soluble, it crosses the blood-brain barrier rapidly; thus, changes in arterial carbon dioxide tension (PaCO2) are sensed rapidly in the brain, producing changes in pH and ventilation. In comparison, the electrolyte composition in the CNS changes over a period of hours [17]. Thus, the effect on central chemoreceptors is less rapid with metabolic than with respiratory acid-base changes. Ventral medullary pH and alpha-imidazole receptors — Chemoreceptors responsive to pH changes are scattered throughout the ventral surface of the medulla [18]. When these areas become mo
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
son, the electrolyte composition in the CNS changes over a period of hours [17]. Thus, the effect on central chemoreceptors is less rapid with metabolic than with respiratory acid-base changes. <span>Ventral medullary pH and alpha-imidazole receptors — Chemoreceptors responsive to pH changes are scattered throughout the ventral surface of the medulla [18]. When these areas become more acidic, hyperventilation ensues and PaCO2 is reduced. In contrast, when the pH rises at these chemoreceptor sites, hypoventilation occurs in order to raise partial pressure of arterial carbon dioxide (PCO2) and normalize pH. Ventilation is dependent upon brain interstitial fluid pH at constant body temperature [19]. However, ventilation does not track with pH if temperature varies; in this setting, ventilat
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
and PaCO2 is reduced. In contrast, when the pH rises at these chemoreceptor sites, hypoventilation occurs in order to raise partial pressure of arterial carbon dioxide (PCO2) and normalize pH. <span>Ventilation is dependent upon brain interstitial fluid pH at constant body temperature [19]. However, ventilation does not track with pH if temperature varies; in this setting, ventilation correlates with the local levels of alpha-imidazole, the fractional dissociation of the imidazole moiety of histidine [20]. At a given temperature, small changes in brain interstitial fluid pH result in large changes in ventilation. For example, perfusion of the brain ventricular system of the turtle with mock cerebrospinal fluid (CSF) with pH 0.03 units below normal resulted in a four-fold increase in ventilation at 20ºC. A 2ºC rise in temperature also changes CSF pH by 0.03 units, but affects neither ventilation nor alpha-imidazole. Regulation of respiration to keep a constant level of alpha-imidazole (the "alphastat") maintains relatively constant protein charge states and enzymatic functions despite changes in te
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
.03 units below normal resulted in a four-fold increase in ventilation at 20ºC. A 2ºC rise in temperature also changes CSF pH by 0.03 units, but affects neither ventilation nor alpha-imidazole. <span>Regulation of respiration to keep a constant level of alpha-imidazole (the "alphastat") maintains relatively constant protein charge states and enzymatic functions despite changes in temperature and pH [21]. Alpha-imidazole regulation of ventilation is presumed to act at the ventral surface of the medulla [22,23]. Brain extracellular fluid composition — In addition to local PaCO2, the pH of brain extracellular fluid (ECF) depends upon CSF electrolyte composition, which changes within several hour
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ein charge states and enzymatic functions despite changes in temperature and pH [21]. Alpha-imidazole regulation of ventilation is presumed to act at the ventral surface of the medulla [22,23]. <span>Brain extracellular fluid composition — In addition to local PaCO2, the pH of brain extracellular fluid (ECF) depends upon CSF electrolyte composition, which changes within several hours of arterial acid-base changes. Local regulation of brain ECF acid-base status is a complex process which involves a number of metabolically active cells, including glial cells, cells of the choroid plexus, and cells which maintain the brain blood-barrier [24]. Alterations in serum pH also eventually lead to changes in brain CSF composition, likely via effects on CSF formation by the choroid plexus. Chronic respiratory acidosis leads to a higher serum and CSF bicarbonate concentration, which ultimately lowers central ventilatory drive as the acidosis is ameliorated [25]. Similarly, CSF pH becomes alkaline due to chronic respiratory alkalosis, as occurs with exposure to high altitude; it then returns toward baseline over the next few days [26]. (See "High altitude illness: Physiology, risk factors, and general prevention".) RESPONSES TO METABOLIC ACIDOSIS AND ALKALOSIS — There is a linear relationship between the plasma bicarb
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
lkalosis, as occurs with exposure to high altitude; it then returns toward baseline over the next few days [26]. (See "High altitude illness: Physiology, risk factors, and general prevention".) <span>RESPONSES TO METABOLIC ACIDOSIS AND ALKALOSIS — There is a linear relationship between the plasma bicarbonate concentration and the change in arterial carbon dioxide tension (PaCO2) in metabolic acidosis and alkalosis [27] (see "Simple and mixed acid-base disorders"). The expected compensations are somewhat different in these disorders: ●For every 1 mEq/L rise in plasma bicarbonate concentration in metabolic alkalosis, the PaCO2 rises by 0.6 to 0.7 mmHg (figure 2) [27]. Thus, for a plasma bicarbonate concentration of 34 mEq/L (10 mEq/L above normal), the expected partial pressure of arterial carbon dioxide (PCO2) is 46 to 47 mmHg. ●For every 1 mEq/L fall in plasma bicarbonate concentration in metabolic acidosis, the PaCO2 falls by approximately 1.2 mmHg [28]. Thus, for a plasma bicarbonate concentration of 14 mEq/L (10 mEq/L below normal), the expected PCO2 is 28 mmHg. Values substantially different from expected reflect a superimposed acid-base disorder. (See "Simple and mixed acid-base disorders".) INTEGRATION OF NEURAL AND CHEMORECEPTOR INPUT — Central respiratory centers receive stimulatory input from central respiratory pacer cells
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
Eq/L (10 mEq/L below normal), the expected PCO2 is 28 mmHg. Values substantially different from expected reflect a superimposed acid-base disorder. (See "Simple and mixed acid-base disorders".) <span>INTEGRATION OF NEURAL AND CHEMORECEPTOR INPUT — Central respiratory centers receive stimulatory input from central respiratory pacer cells, central and peripheral chemoreceptors, upper airway receptors, other areas of the brain, and volitional pathways. Central respiratory centers integrate these signals into a combined output to the muscles of respiration. Much of the effect of peripheral chemoreceptors on ventilation appears to be mediated by its effect on central chemoreceptors. Carotid body peripheral chemoreceptor inputs (both O2 and CO2) have marked synergistic, hyperadditive influences on central chemoreceptor ventilatory sensitivity to central CO2 in studi
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
hese signals into a combined output to the muscles of respiration. Much of the effect of peripheral chemoreceptors on ventilation appears to be mediated by its effect on central chemoreceptors. <span>Carotid body peripheral chemoreceptor inputs (both O2 and CO2) have marked synergistic, hyperadditive influences on central chemoreceptor ventilatory sensitivity to central CO2 in studies in unanesthetized dogs [29,30]. During sleep, the respiratory drive is reduced, usually resulting in a rise in arterial carbon dioxide tension (PaCO2) of 3 to 4 mmHg [31]. (See "Central sleep apnea: Pathogenesis".) There normally is a mild inhibitory input from the cerebral cortex to the respiratory centers. Some stroke patients lose this inhibitory input
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
s [29,30]. During sleep, the respiratory drive is reduced, usually resulting in a rise in arterial carbon dioxide tension (PaCO2) of 3 to 4 mmHg [31]. (See "Central sleep apnea: Pathogenesis".) <span>There normally is a mild inhibitory input from the cerebral cortex to the respiratory centers. Some stroke patients lose this inhibitory input leading to a lower baseline PaCO2 and a tendency toward Cheyne-Stokes respiration [32]. There is also an increased tendency to develop obstructive sleep apnea related to decreased output to the upper airway muscles of respiration. All of these stimulatory and inhibitory signals act to modify the characteristics of respiratory rhythm signals which emanate from central pattern generator cells in the medulla. From the medulla, neural outflow drives the breathing frequency, inspiratory time, and expiratory time. Lesions of the brainstem may cause characteristic abnormalities in breathing pattern. Ataxic, or grossly irregular breathing can occur with medullary lesions, while apneustic breathing,
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
iratory rhythm signals which emanate from central pattern generator cells in the medulla. From the medulla, neural outflow drives the breathing frequency, inspiratory time, and expiratory time. <span>Lesions of the brainstem may cause characteristic abnormalities in breathing pattern. Ataxic, or grossly irregular breathing can occur with medullary lesions, while apneustic breathing, characterized by sustained inspiration, can occur with pontine lesions. EVALUATION OF RESPIRATORY DRIVE AND CONTROL — Assessment of a patient with hypercapnia or abnormal ventilation (eg, increased minute ventilation with a normal arterial carbon dioxide te
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
Polysomnography in the evaluation of sleep-disordered breathing in adults" and "Disorders of ventilatory control" and "Central sleep apnea: Risk factors, clinical presentation, and diagnosis".) <span>Tests of respiratory control are primarily used for research purposes or under special circumstances when pulmonary function testing and respiratory muscle strength have failed to provide an explanation for abnormal levels of arterial oxygen tension (PaO2) or PaCO2. The various tests include measurement of hypoxic and hypercapnic ventilatory responses, mouth occlusion pressure, elastic and resistive load testing, and analysis of the patient's breathing pattern. Tests of ventilatory responses to hypoxia and hypercapnia are potentially hazardous, and there are significant variations among normals. As a result, the clinical condition of the patient and the indications for testing should be carefully considered. During testing, both pulse O2 saturation and end-tidal CO2 tension should be monitored. Respiratory muscle forces — Respiratory muscle forces are easily measured with manometers to quantify airway pressure with the patient breathing against a closed mouthpiece. Maximum pre
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
f the patient and the indications for testing should be carefully considered. During testing, both pulse O2 saturation and end-tidal CO2 tension should be monitored. Respiratory muscle forces — <span>Respiratory muscle forces are easily measured with manometers to quantify airway pressure with the patient breathing against a closed mouthpiece. Maximum pressure generated at the beginning of a full inspiration from residual volume reflects the strength of the inspiratory muscles, while mouth pressure during a forceful expiration from total lung capacity reflects the strength of the expiratory muscles. Respiratory muscle force is dependent upon age, sex, and lung volume; all of these factors should be incorporated into the predicted values for each patient [33-35]. (See "Tests of res
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
upon age, sex, and lung volume; all of these factors should be incorporated into the predicted values for each patient [33-35]. (See "Tests of respiratory muscle strength".) Hypoxic challenge — <span>Testing of the hypoxic ventilatory response is generally limited to research settings or rare circumstances when the etiology of hypoxemia is unclear. Testing is performed by delivering a hypoxic gas mixture (usually 10 to 12 percent O2) to the patient via a rebreathing apparatus, resulting in progressive hypoxemia over four to six minutes. The partial pressures of alveolar and blood CO2 are kept constant by removing CO2 from the rebreathing bag with a soda lime apparatus [36]. Testing can also be performed by having the subject breathe a gas mixture with 8 percent O2 for two minutes [37]. The hypoxic ventilatory response assesses the integrity of the peripheral chemoreceptors and the sensory pathways to the respiratory centers. As arterial oxygen tension falls, peripheral chemoreceptors are stimulated and respiratory drive increases. The normal ventilatory response to oxygen desaturation is linear, with ventilation increasing approximately 1 L/min for each 1 percent fall in oxygen saturation (figure 3). The ventilat
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
of the peripheral chemoreceptors and the sensory pathways to the respiratory centers. As arterial oxygen tension falls, peripheral chemoreceptors are stimulated and respiratory drive increases. <span>The normal ventilatory response to oxygen desaturation is linear, with ventilation increasing approximately 1 L/min for each 1 percent fall in oxygen saturation (figure 3). The ventilatory response is curvilinear if plotted instead against PaO2; as the PaO2 falls below 50 to 55 mmHg, progressively larger increases in minute ventilation occur for equivalent reductions in oxygen tension. Most normal individuals increase their ventilation about three to six times resting values when the arterial PO2 has reached a value of 40 mmHg, which generally corresponds to a hemoglobin saturation of 75 percent. An abnormal hypoxic response generally indicates decreased output from the peripheral chemoreceptors, as occurs with various disease states or senescence, but is also observed in endura
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ls increase their ventilation about three to six times resting values when the arterial PO2 has reached a value of 40 mmHg, which generally corresponds to a hemoglobin saturation of 75 percent. <span>An abnormal hypoxic response generally indicates decreased output from the peripheral chemoreceptors, as occurs with various disease states or senescence, but is also observed in endurance athletes and in persons who reside at high altitudes [38-40]. In the latter two situations, modulation of the hypoxic ventilatory drive may be advantageous by limiting the sensation of dyspnea. (See "Exercise physiology" and "High altitude illness: Physiology, risk factors, and general prevention".) Hypercapnic challenge — Hypercapnic challenge testing is usually used in resea
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
rive may be advantageous by limiting the sensation of dyspnea. (See "Exercise physiology" and "High altitude illness: Physiology, risk factors, and general prevention".) Hypercapnic challenge — <span>Hypercapnic challenge testing is usually used in research settings. The ventilatory response to hypercapnia is usually determined by a rebreathing technique in which the subject rebreathes a hyperoxic gas mixture and gradually increases the PaCO2 over four to six minutes [41,42]. A carbon dioxide analyzer in the mouthpiece measures the end-tidal CO2 tension, which in normal lungs approximates the alveolar and arterial CO2 tension. End-tidal partial pressure of arterial carbon dioxide (PCO2) often poorly reflects PaCO2 in patients with airflow obstruction and other lung abnormalities; direct measurement of arterial PaCO2 is required in these patients. The ventilatory response to CO2 primarily reflects the activity of the central chemoreceptors. The rise in ventilation in response to increases in PaCO2 is linear, generally in the range of 2.5 to 3 L/min for each mmHg increase in PaCO2 [43]. Alterations in ventilatory response to CO2 and O2 — Approximately 15 percent of adults have a diminished response to CO2, defined as an augmentation of ventilation of less than 1 L/min
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
se in ventilation in response to increases in PaCO2 is linear, generally in the range of 2.5 to 3 L/min for each mmHg increase in PaCO2 [43]. Alterations in ventilatory response to CO2 and O2 — <span>Approximately 15 percent of adults have a diminished response to CO2, defined as an augmentation of ventilation of less than 1 L/min per mmHg rise in arterial PCO2. These individuals are likely to develop CO2 retention when additional respiratory problems arise, such as obesity, obstructive lung disease, or status asthmaticus [44-46] (see "Disorders of ventilatory control", section on 'Chronic obstructive pulmonary disease' and "Disorders of ventilatory control", section on 'Asthma'). As with reductions in hypoxic v
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
disease, or status asthmaticus [44-46] (see "Disorders of ventilatory control", section on 'Chronic obstructive pulmonary disease' and "Disorders of ventilatory control", section on 'Asthma'). <span>As with reductions in hypoxic ventilatory drive, diminution of the response to hypercapnia is observed in elderly individuals, endurance athletes, and patients with hypothyroidism [38,47,48]. (See "Respiratory function in thyroid disease".) Depressed ventilatory responses to CO2 can also occur with elevation of serum and brain extracellular fluid (ECF) bicarbonate, such as
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
, diminution of the response to hypercapnia is observed in elderly individuals, endurance athletes, and patients with hypothyroidism [38,47,48]. (See "Respiratory function in thyroid disease".) <span>Depressed ventilatory responses to CO2 can also occur with elevation of serum and brain extracellular fluid (ECF) bicarbonate, such as occurs with metabolic alkalosis or chronic CO2 retention [49]. With a higher brain ECF bicarbonate concentration, the pH will change less for a given change in PCO2, producing less change in ventilation. The ventilatory response can be increased in this setting if the bicarbonate concentration is lowered, as with an infusion of ammonium chloride [50]. Thus, the slope of the ventilatory response to CO2 needs to be evaluated in the context of the patient's acid-base status. (See "Pathogenesis of metabolic alkalosis".) Patients with chronic CO2 retention are often more dependent upon their hypoxic ventilatory drive because they are thought to have a depress
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
f ammonium chloride [50]. Thus, the slope of the ventilatory response to CO2 needs to be evaluated in the context of the patient's acid-base status. (See "Pathogenesis of metabolic alkalosis".) <span>Patients with chronic CO2 retention are often more dependent upon their hypoxic ventilatory drive because they are thought to have a depressed ventilatory response to CO2 (due in large part to the compensatory elevation in the plasma bicarbonate concentration). In these individuals, administration of a high fraction of inspired O2 can depress ventilation, particularly when the PaO2 is raised above 60 mmHg. However, reduction in hypoxic vasoconstriction (with worsening of ventilation-perfusion mismatch) and a shift in the CO2-hemoglobin dissociation curve (the Haldane effect) appear to be more important mechanisms for the increased CO2 retention following O2 administration [51]. Regardless of the mechanism, oxygen should not be withheld from hypoxic patients who have evidence of chronic CO2 retention; in these circumstances oxygen is a life saving measure. (See "The evaluation, diagnosis, and treatment of the adult patient with acute hypercapnic respiratory failure".) Native populations living at high or low altitude in different areas of the world have varied ventilatory responses. Tibetans have higher hypoxic ventilatory responses, higher resting v
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
0 to 10, with 0 being normal breathing and 10 being extreme dyspnea. Normal individuals have short expirations during elastic loading and long inspirations during inspiratory resistive loading. <span>Breathing pattern — The normal response to hypercapnic or hypoxic stimuli is to increase tidal volume with little change in respiratory frequency. Patients with a variety of neuromuscular diseases have a breathing pattern with a low tidal volume and a high frequency, and they maintain this pattern during hypoxic or hypercapnic stress [53,54]. Thus, a disproportionate rise in breathing frequency is suggestive of a disorder of respiratory muscle strength or a stimulus that arises from the thorax, rather than an abnormality of central control. OTHER MEASUREMENTS OF RESPIRATORY EFFORT — The ventilatory drive of patients with severe pulmonary, chest wall, or muscle diseases may not be accurately reflected in measurements of min
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ntercostal muscles is increased in patients with myasthenia gravis compared with normal individuals, while respiratory muscle strength (eg, inspiratory and expiratory forces) is decreased [55]. <span>Neural respiratory drive is also increased in patients with cystic fibrosis and chronic obstructive pulmonary disease (COPD) and is related to severity of disease [56,57]. The EMG response to CO2 rebreathing does not increase as much as does the P0.1 response (see 'Mouth occlusion pressure' below). This suggests that there may be recruitment of additional
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
onse (see 'Mouth occlusion pressure' below). This suggests that there may be recruitment of additional respiratory muscles or enhanced diaphragm muscle efficiency during acute hypercapnia [58]. <span>Mouth occlusion pressure — Measurement of the maximal pressure generated during the first 0.1 second of normal inspiratory effort when the mouth has been occluded (abbreviated P0.1) is helpful in evaluating central ventilatory drive. Effects of respiratory mechanics are minimized in the absence of airflow, and the occlusion is too short to be influenced by muscle weakness or by conscious alterations in respiration [59]. The lack of reduction in P0.1 with muscle weakness is illustrated by the fact that the measurement increases in normal volunteers given curare [60]. P0.1 can be used to assess the ventilatory response to hypoxia and hypercapnia and to assist with weaning patients from mechanical ventilation [61]. A high P0.1 indicates that the patient is exerting near maximal effort and has little reserve. (See "Weaning from mechanical ventilation: Readiness testing".) P0.1 values decrease with age [62], and evidence suggests that individuals born with depressed P0.1 responses are predisp
Flashcard 6321062153484
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321063988492
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321065823500
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321067658508
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321069493516
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321073163532

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321074474252
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321077882124
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321079192844
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321082600716

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321085484300
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321088630028

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321091513612
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321094397196
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321095707916
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321097542924
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321099377932
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321101212940
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321104882956

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321106193676
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321109601548
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321110912268
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321114582284

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321115893004
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321117728012
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321119563020
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321121398028
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321123233036
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321125068044
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321126903052
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321130310924
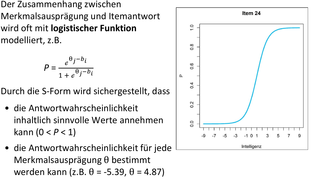
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321131621644
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
gic aspects of ventilatory control and the evaluation of patients with disorders of ventilation are discussed separately. (See "Control of ventilation".) CHRONIC OBSTRUCTIVE PULMONARY DISEASE — <span>Development of hypercapnia in patients with chronic obstructive pulmonary disease (COPD) generally is associated with more severe disease, but is inconsistent among patients with similar degrees of airflow obstruction. Thus, patients with similar spirometric values can exhibit the "blue bloater" profile of hypercapnia (CO2 retention, with an elevated arterial carbon dioxide tension [PaCO2]) and hypoxemia or the "pink puffer" profile with eucapnia and relatively normal oxygen levels [1,2]. Those in the first group have reduced respiratory drive whereas the latter have increased drive. The pattern of breathing in patients with chronic CO2 retention is characterized by a low tidal volume and high frequency, usually ≥22 breaths/minute. This respiratory pattern in combin
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
hypoxemia or the "pink puffer" profile with eucapnia and relatively normal oxygen levels [1,2]. Those in the first group have reduced respiratory drive whereas the latter have increased drive. <span>The pattern of breathing in patients with chronic CO2 retention is characterized by a low tidal volume and high frequency, usually ≥22 breaths/minute. This respiratory pattern in combination with impaired matching of ventilation and perfusion leads to increased dead space ventilation and diminished alveolar ventilation, which contributes to CO2 retention [3]. Some hypercapnic, hypoxemic patients with COPD develop increased CO2 retention when O2 is administered. Such patients usually have both blunted hypercapnic and hypoxic drives [4]. Other
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
pattern in combination with impaired matching of ventilation and perfusion leads to increased dead space ventilation and diminished alveolar ventilation, which contributes to CO2 retention [3]. <span>Some hypercapnic, hypoxemic patients with COPD develop increased CO2 retention when O2 is administered. Such patients usually have both blunted hypercapnic and hypoxic drives [4]. Other factors contributing to CO2 retention during O2 breathing include worsening of ventilation-perfusion distribution secondary to relief of compensatory pulmonary vasoconstriction [5], and unloading of CO2 due to the Haldane effect [6]. (See "The evaluation, diagnosis, and treatment of the adult patient with acute hypercapnic respiratory failure".) ASTHMA — In some patients with asthma, an increased risk of near fatal
Flashcard 6321136602380
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321140010252
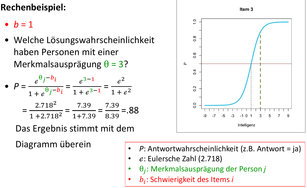
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
sulting in their increased risk of fatal asthma. Asthmatic subjects who develop CO2 retention during an asthma attack are likely to repeat the same in subsequent attacks [7-9]. ONDINE'S CURSE — <span>The term Ondine's curse has been applied to patients with alveolar hypoventilation due to impaired autonomic control of ventilation, but whose voluntary control remains intact. Classically, they "forget to breathe" when they fall asleep, but maintain relatively normal blood gases while awake [10,11]. Ondine's curse is usually due to congenital central hypoventilation syndrome, but can also be caused by brainstem tumors and surgical incisions into the second cervical segment of the s
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
control of ventilation, but whose voluntary control remains intact. Classically, they "forget to breathe" when they fall asleep, but maintain relatively normal blood gases while awake [10,11]. <span>Ondine's curse is usually due to congenital central hypoventilation syndrome, but can also be caused by brainstem tumors and surgical incisions into the second cervical segment of the spinal cord to relieve intractable pain [12,13]. Paroxysmal central apnea has also been observed following medullary infarction [14,15]. (See "Complications of stroke: An overview", section on 'Pulmonary complications'.) Congenital central hypoventilation syndrome — Congenital central hypoventilation syndrome (CCHS) is a
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
escribed separately. (See "Congenital central hypoventilation syndrome and other causes of sleep-related hypoventilation in children", section on 'Congenital central hypoventilation syndrome'.) <span>Late-onset central hypoventilation syndrome — Unlike congenital central hypoventilation syndrome (CCHS), which has a neonatal onset, late-onset central hypoventilation syndrome (LO-CHS) can develop anytime from infancy through adulthood. Like CCHS, these late-presenting cases are caused by PHOX2B mutations. The clinical features, diagnosis, and management of LO-CHS are described separately. (See "Congenital central hypoventilation syndrome and other causes of sleep-related hypoventilation in children", section on 'Late-onset central hypoventilation syndrome'.) Rapid-onset
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
s of sleep-related hypoventilation in children", section on 'Rapid-onset obesity with hypothalamic dysfunction, hypoventilation, and autonomic dysregulation (ROHHAD)'.) CAROTID BODY RESECTION — <span>Carotid body resection, or glomectomy, was introduced as a treatment for asthma in Japan during the 1940s, and used in the United States until the 1960s, when controlled studies of the procedure did not support its efficacy [28]. Carotid body resection has been used for relief of dyspnea in patients with severe COPD, leading to improved dyspnea, but worse hypoxemia and hypercapnia [29]. Glomectomy depresses the hypoxic ventilatory response during exercise; minor abnormalities may also be seen in CO2 regulation during exercise, but eucapnia is generally present at rest
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
]. Glomectomy depresses the hypoxic ventilatory response during exercise; minor abnormalities may also be seen in CO2 regulation during exercise, but eucapnia is generally present at rest [30]. <span>Bilateral endarterectomy for carotid occlusive disease also may result in destruction of peripheral chemoreceptors, with diminution of hypoxic ventilatory response and slight elevation of resting arterial tension of carbon dioxide (PaCO2). CHEYNE-STOKES RESPIRATION — Cheyne-Stokes respiration (CSR) describes cyclic breathing in which apnea is followed by gradually increasing respiratory frequency and tidal volume (ie, hyp
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
disease also may result in destruction of peripheral chemoreceptors, with diminution of hypoxic ventilatory response and slight elevation of resting arterial tension of carbon dioxide (PaCO2). <span>CHEYNE-STOKES RESPIRATION — Cheyne-Stokes respiration (CSR) describes cyclic breathing in which apnea is followed by gradually increasing respiratory frequency and tidal volume (ie, hyperpnea), then gradually decreasing respiratory frequency and tidal volume until the next apneic period [31]. It is considered a type of central sleep apnea syndrome. (See "Sleep-disordered breathing in heart failure".) Mechanism — Delay between changes in ventilation and detection of the resulting arterial tension of carbon dioxide (ie, PaCO2) by the central chemoreceptors maintains a cyclic pattern o
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ecreasing respiratory frequency and tidal volume until the next apneic period [31]. It is considered a type of central sleep apnea syndrome. (See "Sleep-disordered breathing in heart failure".) <span>Mechanism — Delay between changes in ventilation and detection of the resulting arterial tension of carbon dioxide (ie, PaCO2) by the central chemoreceptors maintains a cyclic pattern of respiration. Factors believed to contribute to this delay include prolonged lung to brain circulation time, reduced tissue and lung CO2 and O2 stores, and increased ventilatory drive. The increased ventilatory drive is due, at least in part, to loss of effective damping factors. In contrast to normal physiology, the lowest arterial oxygen saturation and highest PaCO2 occur near peak hyperpnea in CSR, suggesting that the level of PaCO2 at any given moment reflects the patient's stimulation to breathe and not the effectiveness of ventilation. Comorbidities — Cheyne-Stokes respiration is commonly associated with cardiac disease; it can also accompany neurologic disease, sedation, normal sleep, acid-base disturbances, prematur
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
adaptive servoventilation (ASV) in selected patients. The management of CSR is discussed in more detail separately. (See "Sleep-disordered breathing in heart failure", section on 'Management'.) <span>MYXEDEMA — Hypoventilation can occur in patients with severe hypothyroidism [36]. It probably reflects both respiratory muscle weakness and depression of ventilatory drive [37,38]. Some patients will need noninvasive or invasive ventilatory support during the initial phases of thyroid replacement. The evaluation and management of myxedema are discussed separately.
Flashcard 6321151282444
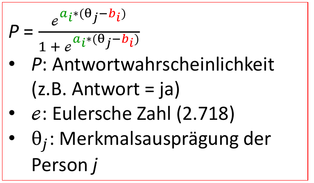
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
upport during the initial phases of thyroid replacement. The evaluation and management of myxedema are discussed separately. (See "Respiratory function in thyroid disease" and "Myxedema coma".) <span>STARVATION — The hypoxic ventilatory response falls approximately 40 percent among normal volunteers following 10 days of 500 kcal/day diet restriction [39]. There is little change in the hypercapnic ventilatory response. Prolonged caloric restriction can have other effects on pulmonary function, including the development of hyperinflation combined with emphysematous radiographic changes [40]. (See "Anorexia nervosa in adults and adolescents: Medical complications and their management", section on 'Pulmonary'.) NEUROMUSCULAR DISEASE — Impairment of the ventilatory response to
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
of hyperinflation combined with emphysematous radiographic changes [40]. (See "Anorexia nervosa in adults and adolescents: Medical complications and their management", section on 'Pulmonary'.) <span>NEUROMUSCULAR DISEASE — Impairment of the ventilatory response to CO2 occurs in patients with a wide variety of neuromuscular diseases [41]. The reduced ventilatory response is due to neuromuscular weakness, and ventilatory drive, as measured by mouth occlusion pressure, is usually well preserved [42-44]. (See "Control of ventilation", section on 'Mouth occlusion pressure'.) Patients with neuromuscular disease show different first-breath ventilatory responses to graded elastic and resist
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
RY DRIVE — A variety of drugs can affect central ventilatory drive. These medications may either depress or stimulate ventilation, and may be useful therapeutically in some clinical situations. <span>Central nervous system depressants — Several classes of drugs suppress central respiratory drive, including opiates, barbiturates, and benzodiazepines. These medications should be used judiciously in patients with preexisting hypoventilation, but may be useful in patients with hyperventilation secondary to pain, anxiety, or malignant pleural effusion [46]. (See "Pain control in the critically ill adult patient" and "Sedative-analgesic medications in critically ill adults: Selection, initiation, maintenance, and withdrawal".) Medroxyproges
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
leural effusion [46]. (See "Pain control in the critically ill adult patient" and "Sedative-analgesic medications in critically ill adults: Selection, initiation, maintenance, and withdrawal".) <span>Medroxyprogesterone — Medroxyprogesterone increases the ventilatory drive in normal males, leading to about a 5 mmHg (0.67 kPa) fall in arterial tension of carbon dioxide (PaCO2) [47]. The drug has been used to treat patients with excessive polycythemia of high altitude and central hypoventilation syndromes, such as the obesity-hypoventilation syndrome [48-50]. (See "Treatment and prognosis of the obesity hypoventilation syndrome".) Its effectiveness in treating hypercapnia associated with COPD is unclear; reductions in PaCO2 are not generally
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
used successfully to treat a woman with diabetes mellitus, neuropathy, and end stage renal disease who had multiple cardiorespiratory arrests secondary to severe Cheyne-Stokes respiration [53]. <span>Acetazolamide — Acetazolamide, an inhibitor of carbonic anhydrase, has several effects relevant to ventilation. ●In the brain, by blocking CO2 conversion to bicarbonate in tissue capillaries, acetazolamide can acutely raise local tissue partial pressure of carbon dioxide (PCO2). Acetazolamide also lowers cerebrospinal fluid bicarbonate in normal individuals at both 3000 and 14,000 feet [54]. Locally elevated PCO2 and lower pH in the brain would increase central ventilatory drive and lower PaCO2. ●In the kidney, acetazolamide increases retention of hydrogen ion and increases renal excretion of bicarbonate, causing a metabolic acidosis over several hours; the metabolic acidosis further increases respiratory drive. ●Opposing the effects that promote increased ventilation, acetazolamide blocks the reciprocal conversion of bicarbonate to CO2 in pulmonary capillaries, thereby impairing the lung's ability to excrete CO2. This could lead to an increase in PaCO2 if ventilation remained constant. However, in normal individuals acetazolamide leads to increased minute ventilation resulting in lower end-tidal PCO2, lower PaCO2, and higher arterial oxygen tension (PaO2) [54,55]. Patients receiving acetazolamide who are able to increase their ventilation will decrease their PaCO2 because their increased ventilatory drive will surpass their impaired lung excretio
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
d constant. However, in normal individuals acetazolamide leads to increased minute ventilation resulting in lower end-tidal PCO2, lower PaCO2, and higher arterial oxygen tension (PaO2) [54,55]. <span>Patients receiving acetazolamide who are able to increase their ventilation will decrease their PaCO2 because their increased ventilatory drive will surpass their impaired lung excretion of CO2. In contrast, patients who are unable to augment their ventilation (eg, those with severe COPD) may develop a severe respiratory acidosis on acetazolamide [56]. A review of the use of acetazolamide in patients with COPD raises concerns of its use in those with severe COPD [57]. Acetazolamide is effective in the prophylaxis and treatment of acute and chronic mountain sickness [58-60]. This effect is likely due to increased ventilation and decreased oxygen desat
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
vere COPD) may develop a severe respiratory acidosis on acetazolamide [56]. A review of the use of acetazolamide in patients with COPD raises concerns of its use in those with severe COPD [57]. <span>Acetazolamide is effective in the prophylaxis and treatment of acute and chronic mountain sickness [58-60]. This effect is likely due to increased ventilation and decreased oxygen desaturation with acetazolamide. (See "High altitude illness: Physiology, risk factors, and general prevention".) In addition, acetazolamide reduces central sleep apneas in patients with heart failure and Cheyne-Stokes
Flashcard 6321162816780
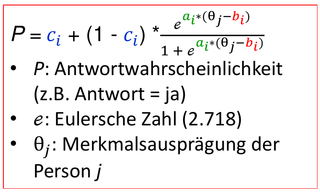
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321165700364
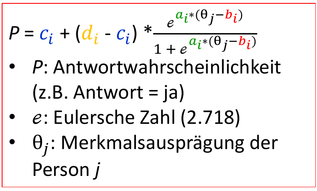
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
review, measures of oxygenation and mechanisms of hypoxemia are discussed. Oxygen delivery and consumption are discussed separately. (See "Oxygen delivery and consumption".) GENERAL CONCEPTS — <span>The process of taking oxygen from the inspired air and using it to sustain aerobic cellular metabolism throughout the body can be conceptualized as having three steps: ●Oxygenation is the process of oxygen diffusing passively from the alveolus to the pulmonary capillary, where it binds to hemoglobin in red blood cells or dissolves into the plasma. Insufficient oxygenation is termed hypoxemia. This is to be differentiated from hypoxia, which is an abnormally low oxygen content in a tissue or organ. ●Oxygen delivery is the rate of oxygen transport from the lungs to the peripheral tissues. ●Oxygen consumption is the rate at which oxygen is removed from the blood for use by the tissues. MEASURES OF OXYGENATION — There are numerous ways to measure whether oxygenation is impaired and at risk of being insufficient to meet the metabolic requirements of the peripheral tissu
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
rous ways to measure whether oxygenation is impaired and at risk of being insufficient to meet the metabolic requirements of the peripheral tissues. Arterial oxygen saturation (SpO2 and SaO2) — <span>SaO2 is a direct measurement of the percent of oxyhemoglobin (oxygen saturated hemoglobin) in the blood using lab tests on arterial blood while SpO2 is a noninvasive measurement of the percent of saturated hemoglobin in the capillary bed using co-oximetry with a pulse oximeter. An SpO2 does not measure the molecule which is saturating hemoglobin such as carboxyhemoglobin or methemoglobin. The oxygen content of arterial blood (CaO2) includes bound and dissolved
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
turated hemoglobin in the capillary bed using co-oximetry with a pulse oximeter. An SpO2 does not measure the molecule which is saturating hemoglobin such as carboxyhemoglobin or methemoglobin. <span>The oxygen content of arterial blood (CaO2) includes bound and dissolved oxygen and is calculated as the following: CaO2 (mL O2/dL) = (1.34 x hemoglobin concentration x SaO2) + (0.0031 x arterial oxygen tension [PaO2]). Most of the oxygen that diffuses from the alveolus to the pulmonary capillary binds to hemoglobin in red blood cells. The SaO2 is the proportion of red blood cells whose hemoglobin is
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
rial blood (CaO2) includes bound and dissolved oxygen and is calculated as the following: CaO2 (mL O2/dL) = (1.34 x hemoglobin concentration x SaO2) + (0.0031 x arterial oxygen tension [PaO2]). <span>Most of the oxygen that diffuses from the alveolus to the pulmonary capillary binds to hemoglobin in red blood cells. The SaO2 is the proportion of red blood cells whose hemoglobin is bound to oxygen. It is most commonly measured noninvasively by pulse oximetry, but can also be measured by arterial blood gas. (See "Pulse oximetry" and "Arterial blood gases".) Abnormal SaO2 has not been defined because an exact threshold below which tissue hypoxia occurs has not been identified. This reflects
Flashcard 6321172778252
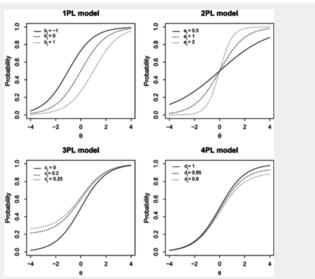
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
e hemoglobin is bound to oxygen. It is most commonly measured noninvasively by pulse oximetry, but can also be measured by arterial blood gas. (See "Pulse oximetry" and "Arterial blood gases".) <span>Abnormal SaO2 has not been defined because an exact threshold below which tissue hypoxia occurs has not been identified. This reflects the multifactorial nature of tissue hypoxia. It seems reasonable to consider a resting SaO2 ≤95 percent or exercise desaturation ≥5 percent abnormal, although these values should not be considered in isolation [1,2]. As an example, a resting SaO2 of 95 percent could be abnormal if a patient previously had a resting SaO2 of 99 percent. However, in general when administering oxygen a resting saturation at sea level should typically target between 94 and 98 percent, unless the patient has COPD in which case 88 to 92 percent is appropriate. Arterial oxygen tension (PaO2) — A small amount of the oxygen that diffuses from the alveolus to the pulmonary capillary dissolves into the plasma. The arterial oxygen tension (PaO2) is
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
general when administering oxygen a resting saturation at sea level should typically target between 94 and 98 percent, unless the patient has COPD in which case 88 to 92 percent is appropriate. <span>Arterial oxygen tension (PaO2) — A small amount of the oxygen that diffuses from the alveolus to the pulmonary capillary dissolves into the plasma. The arterial oxygen tension (PaO2) is the amount of oxygen dissolved in the plasma, which is measured by arterial blood gas. Similar to oxygen saturation, an abnormal PaO2 has not been precisely defined because a threshold below which tissue hypoxia predictably occurs has not been identified. However, it seems reasonable to consider a PaO2 <80 mmHg abnormal, although the value should not be considered in isolation [3]. (See "Arterial blood gases".) A-a oxygen gradient — The alveolar to arterial (A-a) oxygen gradient is a common measure of oxygenation ("A" denotes alveolar and "a" denotes arterial oxyg
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ygenation). It is the difference between the amount of the oxygen in the alveoli (ie, the alveolar oxygen tension [PAO2]) and the amount of oxygen dissolved in the plasma (PaO2) (calculator 1): <span>A-a oxygen gradient = PAO2 - PaO2 PaO2 is measured by arterial blood gas, while PAO2 is calculated using the alveolar gas equation: PAO2 = (FiO2 x [Patm - PH2O]) - (PaCO2 ÷ R) where FiO2 is the fraction of inspired oxygen (0.21 at room air), Patm is the atmospheric pressure (760 mmHg at sea level), PH2O is the partial pressure of water (47 mmHg at 37ºC), PaCO2 is the arterial carbon dioxide tension, and R is the respiratory quotient. The respiratory quotient is approximately 0.8 at steady state, but varies according to the relative utilization of carbohydrate, protein, and fat. The A-a gradient calculated using this alveolar gas equation may deviate from the true gradient by up to 10 mmHg. This reflects the equation's simplification from the more rigorous full calculation and the imprecision of several independent variables (eg, FiO2 and R). The normal A-a gradient varies with age and can be estimated from the following equation, assuming the patient is breathing room air (calculator 1) [4]: A-a gradient = 2.5 + 0.21 x age
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
om the true gradient by up to 10 mmHg. This reflects the equation's simplification from the more rigorous full calculation and the imprecision of several independent variables (eg, FiO2 and R). <span>The normal A-a gradient varies with age and can be estimated from the following equation, assuming the patient is breathing room air (calculator 1) [4]: A-a gradient = 2.5 + 0.21 x age in years The A-a gradient increases with higher FiO2. When a patient receives a high FiO2, both PAO2 and PaO2 increase. However, the PAO2 increases disproportionately, causing the A-a gradient t
Flashcard 6321178283276
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
The normal A-a gradient varies with age and can be estimated from the following equation, assuming the patient is breathing room air (calculator 1) [4]: A-a gradient = 2.5 + 0.21 x age in years <span>The A-a gradient increases with higher FiO2. When a patient receives a high FiO2, both PAO2 and PaO2 increase. However, the PAO2 increases disproportionately, causing the A-a gradient to increase. In one series, the A-a gradient in men breathing air and 100 percent oxygen varied from 8 to 82 mmHg in patients younger than 40 years of age and from 3 to 120 mmHg in patients older than 40 years of age [5]. Proper determinations of the A-a gradient requires exact measurement of FiO2 such as when patients are breathing room air or are receiving mechanical ventilation. The FiO2 of patients r
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
y vary from the predicted, limiting its usefulness. The use of a 100 percent non-rebreathing mask reasonably approximates actual delivery of 100 percent oxygen and can be used to measure shunt. <span>PaO2/FiO2 ratio — The PaO2/FiO2 ratio is another common measure of oxygenation and is most often employed in ventilated patients. A normal PaO2/FiO2 ratio is 300 to 500 mmHg, with values less than 300 mmHg indicating abnormal gas exchange and values less than 200 mmHg indicates severe hypoxemia [6]. As an example, a patient whose PaO2 is 60 mmHg while receiving an FiO2 of 0.5 (ie, 50 percent) has a PaO2/FiO2 ratio of 120 mmHg. a-A oxygen ratio — The arterial to alveolar (a-A) oxyg
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
e and values less than 200 mmHg indicates severe hypoxemia [6]. As an example, a patient whose PaO2 is 60 mmHg while receiving an FiO2 of 0.5 (ie, 50 percent) has a PaO2/FiO2 ratio of 120 mmHg. <span>a-A oxygen ratio — The arterial to alveolar (a-A) oxygen ratio is determined by dividing the PaO2 by the PAO2 ("A" denotes alveolar and "a" denotes arterial oxygenation) [6-8]: a-A oxygen ratio = PaO2 ÷ PAO2 The a-A oxygen ratio is commonly used to predict the change in PaO2 that will result when the FiO2 is changed. Its lower limit of normal is 0.77 to 0.82 and it is most reliable when the FiO2 is less than 0.55 (ie, 55 percent) [7]. Oxygenation index — The oxygenation index (OI) is most commonly used in neonates with persistent pulmonary hypertension of the newborn to determine the severity of hypoxemia and to guid
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
e, low partial oxygen tension). Hypoxia is defined as a condition where the oxygen supply is inadequate either to the body as a whole (general hypoxia) or to a specific region (tissue hypoxia). <span>Hypoxemia does not necessarily indicate tissue hypoxia. It can be caused by hypoventilation, ventilation-perfusion mismatch, right-to-left shunt, diffusion impairment, reduced inspired oxygen tension [11], genetic disorders of hemoglobin oxygen affinity, and other hemoglobin issues which affect oxygen delivery. (See "Genetic disorders of hemoglobin oxygen affinity".) Hypoventilation — The lung alveolus is a space in which gas makes up 100 percent of the contents. This means that once the parti
Flashcard 6321185885452
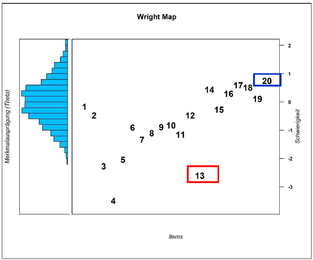
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321188769036
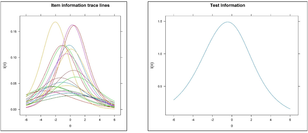
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
inspired oxygen tension [11], genetic disorders of hemoglobin oxygen affinity, and other hemoglobin issues which affect oxygen delivery. (See "Genetic disorders of hemoglobin oxygen affinity".) <span>Hypoventilation — The lung alveolus is a space in which gas makes up 100 percent of the contents. This means that once the partial pressure of one gas rises, the other must decrease. Both arterial (PaCO2) and alveolar (PACO2) carbon dioxide tension increase during hypoventilation, which causes the alveolar oxygen tension (PAO2) to decrease. As a result, diffusion of oxygen from the alveolus to the pulmonary capillary declines with a net effect of hypoxemia and hypercapnia. Because the respiratory quotient (Defined as CO2 eliminated/O2 consumed) is assumed to be 0.8, hypoventilation affects PaCO2 more than O2. (See "The evaluation, diagnosis, and treatment of the adult patient with acute hypercapnic respiratory failure" and "Mechanisms, causes, and effects of hypercapnia".) Hypoxemia due to p
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ffects PaCO2 more than O2. (See "The evaluation, diagnosis, and treatment of the adult patient with acute hypercapnic respiratory failure" and "Mechanisms, causes, and effects of hypercapnia".) <span>Hypoxemia due to pure hypoventilation (ie, in the absence of an elevated A-a gradient) can be identified by two characteristics. First, it readily corrects with a small increase in the fraction of inspired oxygen (FiO2). Second, the paCO2 is elevated. An exception exists when the hypoventilation is prolonged because atelectasis can occur, which will increase the A-a gradient [12]. Abnormalities that cause pure hypoventilation include: ●CNS depression, such as drug overdose, structural CNS lesions, or ischemic CNS lesions that impact the respiratory center ●Obesity hypoventilation (Pickwickian) syndrome ●Impaired neural conduction, such as amyotrophic lateral sclerosis, Guillain-Barré syndrome, high cervical spine injury, phrenic nerve paralysis, or aminoglycoside blockade ●Muscular weakness, such as myasthenia gravis, idiopathic diaphragmatic paralysis, polymyositis, muscular dystrophy, or severe hypothyroidism ●Poor chest wall elasticity, such as a flail chest or kyphoscoliosis V/Q mismatch — Ventilation-perfusion (V/Q) mismatch refers to an imbalance of blood flow and ventilation. It causes the composition of alveolar gas to vary among lung regions: ●Lung reg
Flashcard 6321193749772
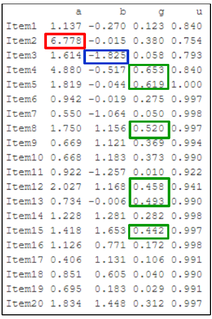
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
s, such as myasthenia gravis, idiopathic diaphragmatic paralysis, polymyositis, muscular dystrophy, or severe hypothyroidism ●Poor chest wall elasticity, such as a flail chest or kyphoscoliosis <span>V/Q mismatch — Ventilation-perfusion (V/Q) mismatch refers to an imbalance of blood flow and ventilation. It causes the composition of alveolar gas to vary among lung regions: ●Lung regions with low ventilation compared to perfusion will have a low alveolar oxygen content and high CO2 content ●Lung regions with high ventilation compared to perfusion will have a low CO2 content and high oxygen content In the normal lung, there is V/Q mismatch because perfusion and ventilation are heterogeneous. Both ventilation and perfusion are greater in the bases than in the apices (when in an upright position). However, the difference between apical and basilar ventilation is smaller than the difference between apical and basilar perfusion. As a result, the V/Q ratio is higher in the apices than in the bases. V/Q mismatch is responsible for the normal physiologic occurring A-a gradient. In the diseased lung, V/Q mismatch increases because heterogeneity of both ventilation and perfusion worsen. The net effect is hypoxemia. Hypoxemia due to V/Q mismatch can be corrected
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
erence between apical and basilar perfusion. As a result, the V/Q ratio is higher in the apices than in the bases. V/Q mismatch is responsible for the normal physiologic occurring A-a gradient. <span>In the diseased lung, V/Q mismatch increases because heterogeneity of both ventilation and perfusion worsen. The net effect is hypoxemia. Hypoxemia due to V/Q mismatch can be corrected with low to moderate flow supplemental oxygen and is characterized by an increased A-a gradient. Common causes of hypoxemia due to V/Q mismatch include obstructive lung diseases, pulmonary vascular diseases, and interstitial diseases. Right-to-left shunt — A right-to-left shunt exists when blood passes from the right to the left side of the heart without being oxygenated. There are two types of right-to-left shunts:
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
ygen and is characterized by an increased A-a gradient. Common causes of hypoxemia due to V/Q mismatch include obstructive lung diseases, pulmonary vascular diseases, and interstitial diseases. <span>Right-to-left shunt — A right-to-left shunt exists when blood passes from the right to the left side of the heart without being oxygenated. There are two types of right-to-left shunts: ●Anatomic shunts exist when the alveoli are bypassed. Examples include intracardiac shunts, pulmonary arteriovenous malformations (AVMs), and hepatopulmonary syndrome. ●Physiologic shunts exist when non-ventilated alveoli are perfused. Examples include atelectasis and diseases with alveolar filling (eg, pneumonia, acute respiratory distress syndrome). Right-to-left shunts cause extreme V/Q mismatch, with a V/Q ratio of zero in some lung regions. The net effect is hypoxemia, which is difficult to correct with supplemental oxygen. The degree of shunt can be quantified from the shunt equation: Qs/Qt = (CcO2 - CaO2) ÷ (CcO2 - CvO2) where Qs/Qt is the shunt fraction, CcO2 is the end-capillary oxygen content, CaO2 is
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
and CvO2 are calculated from arterial and mixed venous blood gas measurements, respectively. CcO2 is estimated from the PAO2. (See "Oxygen delivery and consumption", section on 'Definitions'.) <span>Diffusion limitation — Diffusion limitation exists when the movement of oxygen from the alveolus to the pulmonary capillary is impaired. It is usually a consequence of alveolar and/or interstitial inflammation and fibrosis, such as that due to interstitial lung disease. In such diseases, diffusion limitation usually coexists with V/Q mismatch, which makes the relative contribution of each to the patient's hypoxemia uncertain. Diffusion limitation is characterized by exercise-induced or -exacerbated hypoxemia. This is illustrated by the following: ●During rest, blood traverses the lung relatively slowly. Thus
Flashcard 6321202400524
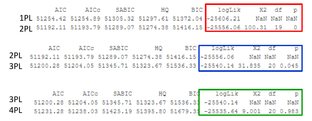
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
due to interstitial lung disease. In such diseases, diffusion limitation usually coexists with V/Q mismatch, which makes the relative contribution of each to the patient's hypoxemia uncertain. <span>Diffusion limitation is characterized by exercise-induced or -exacerbated hypoxemia. This is illustrated by the following: ●During rest, blood traverses the lung relatively slowly. Thus, there is usually sufficient time for oxygenation to occur even if diffusion limitation exists. ●During exercise, cardiac output increases and blood traverses the lung more quickly. As a result, there is less time for oxygenation. •In the healthy individuals, several compensatory mechanisms occur. Pulmonary capillaries dilate, which increases the surface area available for gas exchange by perfusing additional regions of lung. PAO2 also increases, which promotes oxygen diffusion by increasing the oxygen gradient from the alveolus to the artery. The net effect is that full oxygenation is sustained. •In patients with diffusion limitation (such as with pulmonary fibrosis), there is insufficient time for oxygenation to occur. In addition, most such patients have parenchymal destruction, which renders it impossible to recruit additional surface area for gas exchange. The net effect is measurable hypoxemia. Reduced inspired oxygen tension — The inspired oxygen tension (PiO2) is a component of the alveolar gas equation that was described above. It can be determined by the equation: PiO2 = F
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
is insufficient oxygen to meet the metabolic demands of a given tissue. It can result from impaired perfusion (ischemia) and/or diminished arterial oxygen content (due to anemia or hypoxemia). <span>Cellular tolerance of hypoxia is variable. As examples, skeletal muscle cells can recover fully after 30 minutes of hypoxia, but irreversible damage occurs in brain cells after only four to six minutes of similar hypoxic stress [13,14]. Therefore, life-threatening hypoxemia needs to be treated with the administration of oxygen (and sometimes with red cell transfusion) while measures are being initiated to treat the pri
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
UpToDate
atening hypoxemia needs to be treated with the administration of oxygen (and sometimes with red cell transfusion) while measures are being initiated to treat the primary cardiopulmonary insult. <span>Cellular mechanisms that contribute to hypoxic cell injury include depletion of ATP, development of intracellular acidosis, increased concentrations of metabolic by-products, generation of oxygen free radicals, and destruction of membrane phospholipids. There is also a dramatic increase in intracellular calcium concentration, contributing to cellular injury via a variety of mechanisms, including direct damage to the cytoskeleton and induction of genes that contribute to apoptosis [13]. Hypoxia also induces an inflammatory reaction characterized by neutrophilic infiltration, thus augmenting cellular damage via release of cytokine mediators, oxygen free radicals, and by intensifying ischemia due to disruption of the microcirculation. SUMMARY AND RECOMMENDATIONS ●Oxygenation is the process of oxygen diffusing passively from the alveolus to the pulmonary capillary, where it binds to hemoglobin in red blood cells or d
Flashcard 6321208429836
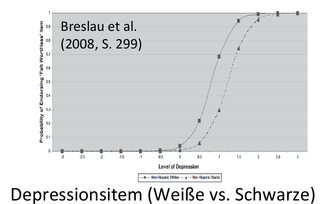
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321211575564

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321215507724

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321218391308
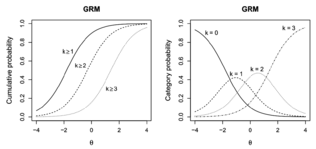
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321221274892

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321224158476

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321227042060
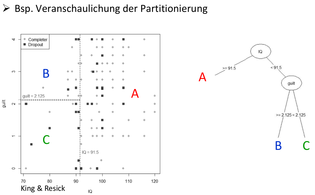
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321228352780
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321232547084

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321235692812

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 6321237003532
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |