Edited, memorised or added to reading queue
on 09-Feb-2017 (Thu)
Do you want BuboFlash to help you learning these things? Click here to log in or create user.
Flashcard 1427360058636
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itEl secretario de la Defensa Nacional, Salvador Cienfuegos, señaló que urge nuevamente que se apruebe un marco legal que regule la actuación del Ejército en las calles.
Original toplevel document
Desnaturalizan nuestra función, advierte SedenaEl secretario de la Defensa Nacional, Salvador Cienfuegos, señaló que urge nuevamente que se apruebe un marco legal que regule la actuación del Ejército en las calles. Salvador Cienfuegos, titular de Sedena, pidió que se definan tiempos y labores para las Fuerzas Armadas. (Especial) “No nos sentimos a gusto, ninguno de los qu
Flashcard 1429051411724
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itWords are categorized by their relationship to being and to each other.
Original toplevel document (pdf)
cannot see any pdfsFlashcard 1429109345548
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itA speculative st udy is one that merely seeks to know—for example, astronomy. We can merely know about the heavenly bodies. We cannot influence their movement s
Original toplevel document (pdf)
cannot see any pdfsFlashcard 1429153647884
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itRhetoric recognizes various levels of discourse, such as the literary (maiden or damsel, steed), the common (girl, horse), the illiterate (gal, hoss), the slang (skirt, plug), the technical (homo sapiens, equus caballus), each with its appropriate use.</s
Original toplevel document (pdf)
cannot see any pdfsFlashcard 1429297302796
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itthe seven fine arts (architecture, instrumental music, sculpture, painting, literature, t he drama, and the dance)
Original toplevel document (pdf)
cannot see any pdfsFlashcard 1429303594252
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itArithmetic, t he theory of number, and music, an application of the theory of number (the measurement of discrete quantities in motion), are the arts of discrete quantity or number.
Original toplevel document (pdf)
cannot see any pdfsFlashcard 1429316963596
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itThe pupil must cooperate with the teacher; he must be active, not passive. The teacher may be present either directly or indirectly. When one studies a book, the author is a teacher indirectly present through the book.
Original toplevel document (pdf)
cannot see any pdfsFlashcard 1430519418124
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itwhich there is some actual common value that will ultimately be revealed after the auction is settled. Prior to the auction’s settlement, however, bidders must estimate that true value. An example of a common value auction would be bidding on <span>a jar containing many coins. Each bidder could estimate the value; but until someone buys the jar and actually counts the coins, no one knows with certainty the true value.<span><body><html>
Original toplevel document
3.8. Auctions as a Way to Find Equilibrium Price> Sometimes markets really do use auctions to arrive at equilibrium price. Auctions can be categorized into two types depending on whether the value of the item being sold is the same for each bidder or is unique to each bidder. <span>The first case is called a common value auction in which there is some actual common value that will ultimately be revealed after the auction is settled. Prior to the auction’s settlement, however, bidders must estimate that true value. An example of a common value auction would be bidding on a jar containing many coins. Each bidder could estimate the value; but until someone buys the jar and actually counts the coins, no one knows with certainty the true value. In the second case, called a private value auction , each buyer places a subjective value on the item, and in general their values differ. An example might be an auction for a unique p
Flashcard 1432424680716
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itsurable goods are those which are desired for their own sake because of the satisfaction they give their possessor. For instance, happiness, an honorable reputation, social prestige, flowers, and savory food are pleasurable goods. <span>They do not add to the intrinsic worth of their possessor, nor are they desired as means, yet they may be associated with valuable goods or useful goods. For instance, knowledg
Original toplevel document (pdf)
cannot see any pdfsFlashcard 1432695475468
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itNouns referring to human beings or animals sometimes have the same grammatical gender as their natural gender, but not always (see below).
Original toplevel document (pdf)
cannot see any pdfsFlashcard 1432719854860
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itNumber Unlike gender, the grammatical concept of singular or plural (‘number’) causes no problem for speakers of English. Occasionally (as in English) a singular noun is used to refer to a collective entity that one might expect to be grammatically plur
Original toplevel document (pdf)
cannot see any pdfsFlashcard 1443032337676
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
An Introduction
The readings in this study session describe the general principles of financial reporting, underscoring the critical role of the analysis of financial reports in investment decision making. The first reading introduces the range of information that is available
The readings in this study session describe the general principles of financial reporting, underscoring the critical role of the analysis of financial reports in investment decision making. The first reading introduces the range of information that is available
Flashcard 1471488855308
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itThis pattern of binding multiple names to multiple values in a fixed-length sequence is called sequence unpacking; it is the same pattern that we see in assignment statements that bind multiple names to multiple values.
Original toplevel document
2.3 Sequenceswo names in its header will bind each name x and y to the first and second elements in each pair, respectively. >>> for x, y in pairs: if x == y: same_count = same_count + 1 >>> same_count 2 <span>This pattern of binding multiple names to multiple values in a fixed-length sequence is called sequence unpacking; it is the same pattern that we see in assignment statements that bind multiple names to multiple values. Ranges. A range is another built-in type of sequence in Python, which represents a range of integers. Ranges are created with range , which takes two integer arguments: the first
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Growth
• At birth = 35cm (avg) o <32cm small head = small brain until proven otherwise • May be inaccurate at birth due to caput succedaneum, molding • 0‐3mths = +2cm/mth • 3‐6mths =+1cm/mth • 6‐12mths = +0.5cm/mth <span>Height • At birth = 50cm (avg) • Doubles height by 4 years • Measure recumbent length until 2 years, then standing height Normal Growth Velocity Growth Charts • Critical to use gender and age appropriate growth charts • In 2010, the CPS, RCFPC and the Dieticians of Can
Flashcard 1473486130444
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itThe basic idea of data abstraction is to structure programs so that they operate on abstract data. That is, our programs should use data in such a way as to make as few assumptions about the data as possible
Original toplevel document
2.2 Data Abstractionwe can make an abstraction that separates the way the function is used from the details of how the function is implemented. Analogously, data abstraction isolates how a compound data value is used from the details of how it is constructed. <span>The basic idea of data abstraction is to structure programs so that they operate on abstract data. That is, our programs should use data in such a way as to make as few assumptions about the data as possible. At the same time, a concrete data representation is defined as an independent part of the program. These two parts of a program, the part that operates on abstract data and the part that defines a concrete representation, are connected by a small set of functions that implement abs
Flashcard 1473657048332
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itl information provided may include: A letter from the chairman of the company, A report from management discussing the results (typically called management discussion and analysis or management commentary), An <span>external auditor’s report providing assurances, A governance report describing the structure of the company’s board of directors, and a corporate responsibility report.<span><body><html>
Original toplevel document
3.1. Financial Statements and Supplementary Informationwith the required financial statements, a company typically provides additional information in its financial reports. In many jurisdictions, some or all of this additional information is mandated by regulators or accounting standards boards. <span>The additional information provided may include a letter from the chairman of the company, a report from management discussing the results (typically called management discussion and analysis [MD&A] or management commentary), an external auditor’s report providing assurances, a governance report describing the structure of the company’s board of directors, and a corporate responsibility report. As part of his or her analysis, the financial analyst should read and assess this additional information along with the financial statements. The following sections describe and illustr
Flashcard 1474081459468
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itThe exposure draft identifies five content elements of a “decision-useful management commentary.” Those content elements include 1) the nature of the business; 2) management’s objectives and strategies; 3) the company’s significant resources, risks, and relationships; 4) results of operations; and 5)
Original toplevel document
3.1.6. Management Commentary or Management’s Discussion and AnalysisASB) issued an exposure draft in June 2009 that proposed a framework for the preparation and presentation of management commentary. Per the exposure draft, that framework will provide guidance rather than set forth requirements in a standard. <span>The exposure draft identifies five content elements of a “decision-useful management commentary.” Those content elements include 1) the nature of the business; 2) management’s objectives and strategies; 3) the company’s significant resources, risks, and relationships; 4) results of operations; and 5) critical performance measures. In the United States, the SEC requires listed companies to provide an MD&A and specifies the content.7 Management must highlight any favorable or unfavorable trends and
Flashcard 1474124975372
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itThe standard independent audit report for a publicly traded company normally has several paragraphs under both the international and US auditing standards.
Original toplevel document
3.1.7. Auditor’s Reportsfinancial statements are fairly presented, meaning that there is a high probability that the audited financial statements are free from materialerror, fraud, or illegal acts that have a direct effect on the financial statements. <span>The standard independent audit report for a publicly traded company normally has several paragraphs under both the international and US auditing standards. The first or “introductory” paragraph describes the financial statements that were audited and the responsibilities of both management and the independent auditor. The second or “scope”
Flashcard 1474366147852
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itThe answer to a specific financial analysis question is rarely the numerical answer alone. Rather, the answer to the analytical question relies on the analyst’s interpretation of the output and the use of this interpreted output to support a conclusion or recommendation.
Original toplevel document
4.4. Analyze/Interpret the Processed DataOnce the data have been processed, the next step—critical to any analysis—is to interpret the output. The answer to a specific financial analysis question is seldom the numerical answer alone. Rather, the answer to the analytical question relies on the analyst’s interpretation of the output and the use of this interpreted output to support a conclusion or recommendation. The answers to the specific analytical questions may themselves achieve the underlying purpose of the analysis, but usually, a conclusion or recommendation is required. For example, an
Flashcard 1474563542284
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itFor presentation purposes, assets are sometimes categorized as “current” or “non-current.”
Original toplevel document
3.1. Financial Statement Elements and Accounts(e.g., rent, utilities, salaries, advertising) Depreciation and amortization Interest expense Tax expense Losses <span>For presentation purposes, assets are sometimes categorized as “current” or “non-current.” For example, Tesco (a large European retailer) presents the following major asset accounts in its 2006 financial reports: Non-current assets: In
Flashcard 1474647952652
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itA full term baby presents with an eating disorder (i.e. FTT). What is your DDx? ↓intake: non-organic , GERD, structural, CNS, genetic ↓absorption: CF, CMPA, short gut, biliary atresia, GI ↑loss: gastroenteritis ↑demand: cardiac, ↑THY, infection, res
Original toplevel document
Growthobstructive uropathy Ix: CBC/Fe, celiac screen (tTGT), lytes, urea, Cr, TSH, U/A, Ca 2+ , Vit ADE 14yo at 3 rd %ile weight + 10 th %ile height is not eating well. What are 3 possible causes? See above <span>A full term baby presents with an eating disorder (i.e. FTT). What is your DDx? ↓intake: non-organic , GERD, structural, CNS, genetic ↓absorption: CF, CMPA, short gut, biliary atresia, GI ↑loss: gastroenteritis ↑demand: cardiac, ↑THY, infection, respiratory Ineffective use: inborn error of metabolism Obesity 14yo ♂ with weight of 67 kg, height 150cm. Calculate BMI: 29.8 kg/m 2 4 complications of obesity: HTN, dyslipidemia, OSA, SCFE, nonEtO
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1475808201996
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itDevelopmental assessment Primitive reflexes Mnemonic: MPRAG M Moro P Placing reflex R Rooting A Atonic neck reflex G Grasp reflex
Original toplevel document
Developmentn one foot to undress, so she and mom can read a story together. A Wrinkle in Time. 5 years: Skip, Tie shoes, Difference between reality/fantasy Oz Baby: ties ruby shoes, skips down Yellow Brick Road back to Kansas <span>Developmental assessment Primitive reflexes Mnemonic: MPRAG M Moro P Placing reflex R Rooting A Atonic neck reflex G Grasp reflex Head circumference with age · Remember 3, 9, and multiples of 5: Newborn 35 cm 3 mos 40 cm 9 mos 45 cm 3 yrs 50 cm 9 yrs 5
Flashcard 1475809774860
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itDevelopmental assessment Primitive reflexes Mnemonic: MPRAG M Moro P Placing reflex R Rooting A Atonic neck reflex G Grasp reflex
Original toplevel document
Developmentn one foot to undress, so she and mom can read a story together. A Wrinkle in Time. 5 years: Skip, Tie shoes, Difference between reality/fantasy Oz Baby: ties ruby shoes, skips down Yellow Brick Road back to Kansas <span>Developmental assessment Primitive reflexes Mnemonic: MPRAG M Moro P Placing reflex R Rooting A Atonic neck reflex G Grasp reflex Head circumference with age · Remember 3, 9, and multiples of 5: Newborn 35 cm 3 mos 40 cm 9 mos 45 cm 3 yrs 50 cm 9 yrs 5
Flashcard 1475811347724
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itDevelopmental assessment Primitive reflexes Mnemonic: MPRAG M Moro P Placing reflex R Rooting A Atonic neck reflex G Grasp reflex
Original toplevel document
Developmentn one foot to undress, so she and mom can read a story together. A Wrinkle in Time. 5 years: Skip, Tie shoes, Difference between reality/fantasy Oz Baby: ties ruby shoes, skips down Yellow Brick Road back to Kansas <span>Developmental assessment Primitive reflexes Mnemonic: MPRAG M Moro P Placing reflex R Rooting A Atonic neck reflex G Grasp reflex Head circumference with age · Remember 3, 9, and multiples of 5: Newborn 35 cm 3 mos 40 cm 9 mos 45 cm 3 yrs 50 cm 9 yrs 5
Flashcard 1475812920588
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itDevelopmental assessment Primitive reflexes Mnemonic: MPRAG M Moro P Placing reflex R Rooting A Atonic neck reflex G Grasp reflex
Original toplevel document
Developmentn one foot to undress, so she and mom can read a story together. A Wrinkle in Time. 5 years: Skip, Tie shoes, Difference between reality/fantasy Oz Baby: ties ruby shoes, skips down Yellow Brick Road back to Kansas <span>Developmental assessment Primitive reflexes Mnemonic: MPRAG M Moro P Placing reflex R Rooting A Atonic neck reflex G Grasp reflex Head circumference with age · Remember 3, 9, and multiples of 5: Newborn 35 cm 3 mos 40 cm 9 mos 45 cm 3 yrs 50 cm 9 yrs 5
Flashcard 1475815542028
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itDevelopmental assessment Primitive reflexes Mnemonic: MPRAG M Moro P Placing reflex R Rooting A Atonic neck reflex G Grasp reflex
Original toplevel document
Developmentn one foot to undress, so she and mom can read a story together. A Wrinkle in Time. 5 years: Skip, Tie shoes, Difference between reality/fantasy Oz Baby: ties ruby shoes, skips down Yellow Brick Road back to Kansas <span>Developmental assessment Primitive reflexes Mnemonic: MPRAG M Moro P Placing reflex R Rooting A Atonic neck reflex G Grasp reflex Head circumference with age · Remember 3, 9, and multiples of 5: Newborn 35 cm 3 mos 40 cm 9 mos 45 cm 3 yrs 50 cm 9 yrs 5

| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open itProgress Note (Template) (Service) Progress Note Date, Time ID Age, sex with a history of (non‐active/chronic issues) admitted with (list active/acute issues for why the patient is admitted). Could also include a list of recent events that occurred since the most recent note. SUBJECTIVE • How was patient overnight, how they feel that day, any new concerns from the patient/parent • What has changed since the previous note? Does the patient
Original toplevel document
Documentationegular medications (may not need all; e.g., no need for previous PO antibiotics if starting IV) o Present: what does patient need now o Future: anticipate what patient may need; e.g., fever, nausea, pain, stools <span>Progress Note (Template) (Service) Progress Note Date, Time ID Age, sex with a history of (non‐active/chronic issues) admitted with (list active/acute issues for why the patient is admitted). Could also include a list of recent events that occurred since the most recent note. SUBJECTIVE • How was patient overnight, how they feel that day, any new concerns from the patient/parent • What has changed since the previous note? Does the patient have any new symptoms? Any pain? How is the patient coping with the active symptoms, progression, better/worse. • Ask the parents and patient’s nurse: behaviour, activity, sleep, appetite, in and outs. OBJECTIVE Vitals: HR, BP, RR, SaO2, Temp, daily weight, pain I/O: Inputs (Diet, IVF), Output (U/O, BM/Diarrhea, Vx, Drains), fluid balance General: what the patient is doing, appearance, behaviour, cognition, cooperation, disposition P/E: focused physical exam of system involved plus CVS, RESP, ABDO as it is common for hospitalized patients to develop problems in these regions. INVESTIGATIONS New lab results, imaging or diagnostic tests/ interventions and relevant results still pending MEDS Reviewed daily regarding changes such as new/held/discontinued/ restarted (e.g. Ampicillin day 2/10) IMPRESSION/ASSESSMENT (IMP) Summarize what the new findings mean, what progress is being made. Stable vs. Unstable? Improved vs. Worsened? Waiting investigations/ consult? Differential diagnosis if anything has been ruled in/out? PLAN (P) 1. Issue (1) plan (e.g., UTI on Day 2 of Empiric Abx, likely 14 day course required, await urine C&S) 2. Issue (2) plan 3. Issue (3) plan 4. Disposition – plans for home, transfer Discharge Summary (Template) Check patient’s name, medical record number, date of birth, date of admission, date of discharge, most responsible physician (MRP), ref
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open itID Age, sex with a history of (non‐active/chronic issues) admitted with (list active/acute issues for why the patient is admitted). Could also include a list of recent events that occurred since the most recent note. <span>SUBJECTIVE • How was patient overnight, how they feel that day, any new concerns from the patient/parent • What has changed since the previous note? Does the patient have any new symptoms? Any pain? How is the patient coping with the active symptoms, progression, better/worse. • Ask the parents and patient’s nurse: behaviour, activity, sleep, appetite, in and outs. OBJECTIVE Vitals: HR, BP, RR, SaO2, Temp, daily weight, pain I/O: Inputs (Diet, IVF), Output (U/O, BM/Diarrhea, Vx, Drains), fluid balance General: what the pat
Original toplevel document
Documentationegular medications (may not need all; e.g., no need for previous PO antibiotics if starting IV) o Present: what does patient need now o Future: anticipate what patient may need; e.g., fever, nausea, pain, stools <span>Progress Note (Template) (Service) Progress Note Date, Time ID Age, sex with a history of (non‐active/chronic issues) admitted with (list active/acute issues for why the patient is admitted). Could also include a list of recent events that occurred since the most recent note. SUBJECTIVE • How was patient overnight, how they feel that day, any new concerns from the patient/parent • What has changed since the previous note? Does the patient have any new symptoms? Any pain? How is the patient coping with the active symptoms, progression, better/worse. • Ask the parents and patient’s nurse: behaviour, activity, sleep, appetite, in and outs. OBJECTIVE Vitals: HR, BP, RR, SaO2, Temp, daily weight, pain I/O: Inputs (Diet, IVF), Output (U/O, BM/Diarrhea, Vx, Drains), fluid balance General: what the patient is doing, appearance, behaviour, cognition, cooperation, disposition P/E: focused physical exam of system involved plus CVS, RESP, ABDO as it is common for hospitalized patients to develop problems in these regions. INVESTIGATIONS New lab results, imaging or diagnostic tests/ interventions and relevant results still pending MEDS Reviewed daily regarding changes such as new/held/discontinued/ restarted (e.g. Ampicillin day 2/10) IMPRESSION/ASSESSMENT (IMP) Summarize what the new findings mean, what progress is being made. Stable vs. Unstable? Improved vs. Worsened? Waiting investigations/ consult? Differential diagnosis if anything has been ruled in/out? PLAN (P) 1. Issue (1) plan (e.g., UTI on Day 2 of Empiric Abx, likely 14 day course required, await urine C&S) 2. Issue (2) plan 3. Issue (3) plan 4. Disposition – plans for home, transfer Discharge Summary (Template) Check patient’s name, medical record number, date of birth, date of admission, date of discharge, most responsible physician (MRP), ref
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open itoes the patient have any new symptoms? Any pain? How is the patient coping with the active symptoms, progression, better/worse. • Ask the parents and patient’s nurse: behaviour, activity, sleep, appetite, in and outs. <span>OBJECTIVE Vitals: HR, BP, RR, SaO2, Temp, daily weight, pain I/O: Inputs (Diet, IVF), Output (U/O, BM/Diarrhea, Vx, Drains), fluid balance General: what the patient is doing, appearance, behaviour, cognition, cooperation, disposition P/E: focused physical exam of system involved plus CVS, RESP, ABDO as it is common for hospitalized patients to develop problems in these regions. INVESTIGATIONS New lab results, imaging or diagnostic tests/ interventions and relevant results still pending MEDS Reviewed daily regarding changes such as new/
Original toplevel document
Documentationegular medications (may not need all; e.g., no need for previous PO antibiotics if starting IV) o Present: what does patient need now o Future: anticipate what patient may need; e.g., fever, nausea, pain, stools <span>Progress Note (Template) (Service) Progress Note Date, Time ID Age, sex with a history of (non‐active/chronic issues) admitted with (list active/acute issues for why the patient is admitted). Could also include a list of recent events that occurred since the most recent note. SUBJECTIVE • How was patient overnight, how they feel that day, any new concerns from the patient/parent • What has changed since the previous note? Does the patient have any new symptoms? Any pain? How is the patient coping with the active symptoms, progression, better/worse. • Ask the parents and patient’s nurse: behaviour, activity, sleep, appetite, in and outs. OBJECTIVE Vitals: HR, BP, RR, SaO2, Temp, daily weight, pain I/O: Inputs (Diet, IVF), Output (U/O, BM/Diarrhea, Vx, Drains), fluid balance General: what the patient is doing, appearance, behaviour, cognition, cooperation, disposition P/E: focused physical exam of system involved plus CVS, RESP, ABDO as it is common for hospitalized patients to develop problems in these regions. INVESTIGATIONS New lab results, imaging or diagnostic tests/ interventions and relevant results still pending MEDS Reviewed daily regarding changes such as new/held/discontinued/ restarted (e.g. Ampicillin day 2/10) IMPRESSION/ASSESSMENT (IMP) Summarize what the new findings mean, what progress is being made. Stable vs. Unstable? Improved vs. Worsened? Waiting investigations/ consult? Differential diagnosis if anything has been ruled in/out? PLAN (P) 1. Issue (1) plan (e.g., UTI on Day 2 of Empiric Abx, likely 14 day course required, await urine C&S) 2. Issue (2) plan 3. Issue (3) plan 4. Disposition – plans for home, transfer Discharge Summary (Template) Check patient’s name, medical record number, date of birth, date of admission, date of discharge, most responsible physician (MRP), ref
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open itatient is doing, appearance, behaviour, cognition, cooperation, disposition P/E: focused physical exam of system involved plus CVS, RESP, ABDO as it is common for hospitalized patients to develop problems in these regions. <span>INVESTIGATIONS New lab results, imaging or diagnostic tests/ interventions and relevant results still pending MEDS Reviewed daily regarding changes such as new/held/discontinued/ restarted (e.g. Ampicillin day 2/10) IMPRESSION/ASSESSMENT (IMP) Summarize what the new fin
Original toplevel document
Documentationegular medications (may not need all; e.g., no need for previous PO antibiotics if starting IV) o Present: what does patient need now o Future: anticipate what patient may need; e.g., fever, nausea, pain, stools <span>Progress Note (Template) (Service) Progress Note Date, Time ID Age, sex with a history of (non‐active/chronic issues) admitted with (list active/acute issues for why the patient is admitted). Could also include a list of recent events that occurred since the most recent note. SUBJECTIVE • How was patient overnight, how they feel that day, any new concerns from the patient/parent • What has changed since the previous note? Does the patient have any new symptoms? Any pain? How is the patient coping with the active symptoms, progression, better/worse. • Ask the parents and patient’s nurse: behaviour, activity, sleep, appetite, in and outs. OBJECTIVE Vitals: HR, BP, RR, SaO2, Temp, daily weight, pain I/O: Inputs (Diet, IVF), Output (U/O, BM/Diarrhea, Vx, Drains), fluid balance General: what the patient is doing, appearance, behaviour, cognition, cooperation, disposition P/E: focused physical exam of system involved plus CVS, RESP, ABDO as it is common for hospitalized patients to develop problems in these regions. INVESTIGATIONS New lab results, imaging or diagnostic tests/ interventions and relevant results still pending MEDS Reviewed daily regarding changes such as new/held/discontinued/ restarted (e.g. Ampicillin day 2/10) IMPRESSION/ASSESSMENT (IMP) Summarize what the new findings mean, what progress is being made. Stable vs. Unstable? Improved vs. Worsened? Waiting investigations/ consult? Differential diagnosis if anything has been ruled in/out? PLAN (P) 1. Issue (1) plan (e.g., UTI on Day 2 of Empiric Abx, likely 14 day course required, await urine C&S) 2. Issue (2) plan 3. Issue (3) plan 4. Disposition – plans for home, transfer Discharge Summary (Template) Check patient’s name, medical record number, date of birth, date of admission, date of discharge, most responsible physician (MRP), ref
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open itvolved plus CVS, RESP, ABDO as it is common for hospitalized patients to develop problems in these regions. INVESTIGATIONS New lab results, imaging or diagnostic tests/ interventions and relevant results still pending <span>MEDS Reviewed daily regarding changes such as new/held/discontinued/ restarted (e.g. Ampicillin day 2/10) IMPRESSION/ASSESSMENT (IMP) Summarize what the new findings mean, what progress is being made. Stable vs. Unstable? Improved vs. Worsened? Waiting investigations/ co
Original toplevel document
Documentationegular medications (may not need all; e.g., no need for previous PO antibiotics if starting IV) o Present: what does patient need now o Future: anticipate what patient may need; e.g., fever, nausea, pain, stools <span>Progress Note (Template) (Service) Progress Note Date, Time ID Age, sex with a history of (non‐active/chronic issues) admitted with (list active/acute issues for why the patient is admitted). Could also include a list of recent events that occurred since the most recent note. SUBJECTIVE • How was patient overnight, how they feel that day, any new concerns from the patient/parent • What has changed since the previous note? Does the patient have any new symptoms? Any pain? How is the patient coping with the active symptoms, progression, better/worse. • Ask the parents and patient’s nurse: behaviour, activity, sleep, appetite, in and outs. OBJECTIVE Vitals: HR, BP, RR, SaO2, Temp, daily weight, pain I/O: Inputs (Diet, IVF), Output (U/O, BM/Diarrhea, Vx, Drains), fluid balance General: what the patient is doing, appearance, behaviour, cognition, cooperation, disposition P/E: focused physical exam of system involved plus CVS, RESP, ABDO as it is common for hospitalized patients to develop problems in these regions. INVESTIGATIONS New lab results, imaging or diagnostic tests/ interventions and relevant results still pending MEDS Reviewed daily regarding changes such as new/held/discontinued/ restarted (e.g. Ampicillin day 2/10) IMPRESSION/ASSESSMENT (IMP) Summarize what the new findings mean, what progress is being made. Stable vs. Unstable? Improved vs. Worsened? Waiting investigations/ consult? Differential diagnosis if anything has been ruled in/out? PLAN (P) 1. Issue (1) plan (e.g., UTI on Day 2 of Empiric Abx, likely 14 day course required, await urine C&S) 2. Issue (2) plan 3. Issue (3) plan 4. Disposition – plans for home, transfer Discharge Summary (Template) Check patient’s name, medical record number, date of birth, date of admission, date of discharge, most responsible physician (MRP), ref
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open itESTIGATIONS New lab results, imaging or diagnostic tests/ interventions and relevant results still pending MEDS Reviewed daily regarding changes such as new/held/discontinued/ restarted (e.g. Ampicillin day 2/10) <span>IMPRESSION/ASSESSMENT (IMP) Summarize what the new findings mean, what progress is being made. Stable vs. Unstable? Improved vs. Worsened? Waiting investigations/ consult? Differential diagnosis if anything has been ruled in/out? PLAN (P) 1. Issue (1) plan (e.g., UTI on Day 2 of Empiric Abx, likely 14 day course required, await urine C&S) 2. Issue (2) plan 3. Issue (3) plan
Original toplevel document
Documentationegular medications (may not need all; e.g., no need for previous PO antibiotics if starting IV) o Present: what does patient need now o Future: anticipate what patient may need; e.g., fever, nausea, pain, stools <span>Progress Note (Template) (Service) Progress Note Date, Time ID Age, sex with a history of (non‐active/chronic issues) admitted with (list active/acute issues for why the patient is admitted). Could also include a list of recent events that occurred since the most recent note. SUBJECTIVE • How was patient overnight, how they feel that day, any new concerns from the patient/parent • What has changed since the previous note? Does the patient have any new symptoms? Any pain? How is the patient coping with the active symptoms, progression, better/worse. • Ask the parents and patient’s nurse: behaviour, activity, sleep, appetite, in and outs. OBJECTIVE Vitals: HR, BP, RR, SaO2, Temp, daily weight, pain I/O: Inputs (Diet, IVF), Output (U/O, BM/Diarrhea, Vx, Drains), fluid balance General: what the patient is doing, appearance, behaviour, cognition, cooperation, disposition P/E: focused physical exam of system involved plus CVS, RESP, ABDO as it is common for hospitalized patients to develop problems in these regions. INVESTIGATIONS New lab results, imaging or diagnostic tests/ interventions and relevant results still pending MEDS Reviewed daily regarding changes such as new/held/discontinued/ restarted (e.g. Ampicillin day 2/10) IMPRESSION/ASSESSMENT (IMP) Summarize what the new findings mean, what progress is being made. Stable vs. Unstable? Improved vs. Worsened? Waiting investigations/ consult? Differential diagnosis if anything has been ruled in/out? PLAN (P) 1. Issue (1) plan (e.g., UTI on Day 2 of Empiric Abx, likely 14 day course required, await urine C&S) 2. Issue (2) plan 3. Issue (3) plan 4. Disposition – plans for home, transfer Discharge Summary (Template) Check patient’s name, medical record number, date of birth, date of admission, date of discharge, most responsible physician (MRP), ref
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open itION/ASSESSMENT (IMP) Summarize what the new findings mean, what progress is being made. Stable vs. Unstable? Improved vs. Worsened? Waiting investigations/ consult? Differential diagnosis if anything has been ruled in/out? <span>PLAN (P) 1. Issue (1) plan (e.g., UTI on Day 2 of Empiric Abx, likely 14 day course required, await urine C&S) 2. Issue (2) plan 3. Issue (3) plan 4. Disposition – plans for home, transfer<span><body><html>
Original toplevel document
Documentationegular medications (may not need all; e.g., no need for previous PO antibiotics if starting IV) o Present: what does patient need now o Future: anticipate what patient may need; e.g., fever, nausea, pain, stools <span>Progress Note (Template) (Service) Progress Note Date, Time ID Age, sex with a history of (non‐active/chronic issues) admitted with (list active/acute issues for why the patient is admitted). Could also include a list of recent events that occurred since the most recent note. SUBJECTIVE • How was patient overnight, how they feel that day, any new concerns from the patient/parent • What has changed since the previous note? Does the patient have any new symptoms? Any pain? How is the patient coping with the active symptoms, progression, better/worse. • Ask the parents and patient’s nurse: behaviour, activity, sleep, appetite, in and outs. OBJECTIVE Vitals: HR, BP, RR, SaO2, Temp, daily weight, pain I/O: Inputs (Diet, IVF), Output (U/O, BM/Diarrhea, Vx, Drains), fluid balance General: what the patient is doing, appearance, behaviour, cognition, cooperation, disposition P/E: focused physical exam of system involved plus CVS, RESP, ABDO as it is common for hospitalized patients to develop problems in these regions. INVESTIGATIONS New lab results, imaging or diagnostic tests/ interventions and relevant results still pending MEDS Reviewed daily regarding changes such as new/held/discontinued/ restarted (e.g. Ampicillin day 2/10) IMPRESSION/ASSESSMENT (IMP) Summarize what the new findings mean, what progress is being made. Stable vs. Unstable? Improved vs. Worsened? Waiting investigations/ consult? Differential diagnosis if anything has been ruled in/out? PLAN (P) 1. Issue (1) plan (e.g., UTI on Day 2 of Empiric Abx, likely 14 day course required, await urine C&S) 2. Issue (2) plan 3. Issue (3) plan 4. Disposition – plans for home, transfer Discharge Summary (Template) Check patient’s name, medical record number, date of birth, date of admission, date of discharge, most responsible physician (MRP), ref
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open itIrritability may be the only way that a young child can express pain or discomfort from any source, including: Meningeal irritation Headache from intracranial irritation Simple exhaustion
Original toplevel document
CLIPP 11 - Kawasaki11. 5-year-old with fever and adenopathy - Jason January 27, 2017 2:09:56 PM EST Knowledge Irritability in a Child Irritability may be the only way that a young child can express pain or discomfort from any source, including: Meningeal irritation Headache from intracranial irritation Simple exhaustion Pediatric Vital Signs As a child gets older, the normal ranges for vital signs change, making it important to look at ageappropriate reference values. The normal hea
Flashcard 1475880291596
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open ith Fever (Part 1) Children get many different kinds of rashes-many, though not all, related to infections. Below are descriptions and photos of rashes associated with fever. Cho Sooyoung - sooyoung.cho@mail.utoronto.ca 1/15 <span>Enterovirus Usually erythematous and maculopapular, and may involve the palms and soles. Infrequently, it can be petechial. In hand-foot-and-mouth disease (caused by Coxsackie virus), presents as a vesicular rash on the hands and feet and with ulcers in the mouth. Usually seen in late summer a
Original toplevel document
CLIPP 11 - Kawasaki; Pediatric Vital Signs As a child gets older, the normal ranges for vital signs change, making it important to look at ageappropriate reference values. The normal heart rate for a 5-year-old is 80 to 100 beats per minute. <span>Rashes Associated with Fever (Part 1) Children get many different kinds of rashes-many, though not all, related to infections. Below are descriptions and photos of rashes associated with fever. Cho Sooyoung - sooyoung.cho@mail.utoronto.ca 1/15 Enterovirus Usually erythematous and maculopapular, and may involve the palms and soles. Infrequently, it can be petechial. In hand-foot-and-mouth disease (caused by Coxsackie virus), presents as a vesicular rash on the hands and feet and with ulcers in the mouth. Usually seen in late summer and early fall. While the fever associated with enteroviruses may be high, it usually lasts only a few days. Erythema infectiosum Also called fifth disease, this is caused by parvovirus B19. There is frequently an associated low-grade fever (37.8-38.3 degrees C, or 100
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open itand photos of rashes associated with fever. Cho Sooyoung - sooyoung.cho@mail.utoronto.ca 1/15 Enterovirus Usually erythematous and maculopapular, and may involve the palms and soles. Infrequently, it can be petechial. <span>In hand-foot-and-mouth disease (caused by Coxsackie virus), presents as a vesicular rash on the hands and feet and with ulcers in the mouth. Usually seen in late summer and early fall. While the fever associated with enteroviruses may be high, it usually lasts only a few days.<span><body><html>
Original toplevel document
CLIPP 11 - Kawasaki; Pediatric Vital Signs As a child gets older, the normal ranges for vital signs change, making it important to look at ageappropriate reference values. The normal heart rate for a 5-year-old is 80 to 100 beats per minute. <span>Rashes Associated with Fever (Part 1) Children get many different kinds of rashes-many, though not all, related to infections. Below are descriptions and photos of rashes associated with fever. Cho Sooyoung - sooyoung.cho@mail.utoronto.ca 1/15 Enterovirus Usually erythematous and maculopapular, and may involve the palms and soles. Infrequently, it can be petechial. In hand-foot-and-mouth disease (caused by Coxsackie virus), presents as a vesicular rash on the hands and feet and with ulcers in the mouth. Usually seen in late summer and early fall. While the fever associated with enteroviruses may be high, it usually lasts only a few days. Erythema infectiosum Also called fifth disease, this is caused by parvovirus B19. There is frequently an associated low-grade fever (37.8-38.3 degrees C, or 100
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open itopapular, and may involve the palms and soles. Infrequently, it can be petechial. In hand-foot-and-mouth disease (caused by Coxsackie virus), presents as a vesicular rash on the hands and feet and with ulcers in the mouth. <span>Usually seen in late summer and early fall. While the fever associated with enteroviruses may be high, it usually lasts only a few days.<span><body><html>
Original toplevel document
CLIPP 11 - Kawasaki; Pediatric Vital Signs As a child gets older, the normal ranges for vital signs change, making it important to look at ageappropriate reference values. The normal heart rate for a 5-year-old is 80 to 100 beats per minute. <span>Rashes Associated with Fever (Part 1) Children get many different kinds of rashes-many, though not all, related to infections. Below are descriptions and photos of rashes associated with fever. Cho Sooyoung - sooyoung.cho@mail.utoronto.ca 1/15 Enterovirus Usually erythematous and maculopapular, and may involve the palms and soles. Infrequently, it can be petechial. In hand-foot-and-mouth disease (caused by Coxsackie virus), presents as a vesicular rash on the hands and feet and with ulcers in the mouth. Usually seen in late summer and early fall. While the fever associated with enteroviruses may be high, it usually lasts only a few days. Erythema infectiosum Also called fifth disease, this is caused by parvovirus B19. There is frequently an associated low-grade fever (37.8-38.3 degrees C, or 100
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open its. Infrequently, it can be petechial. In hand-foot-and-mouth disease (caused by Coxsackie virus), presents as a vesicular rash on the hands and feet and with ulcers in the mouth. Usually seen in late summer and early fall. <span>While the fever associated with enteroviruses may be high, it usually lasts only a few days.<span><body><html>
Original toplevel document
CLIPP 11 - Kawasaki; Pediatric Vital Signs As a child gets older, the normal ranges for vital signs change, making it important to look at ageappropriate reference values. The normal heart rate for a 5-year-old is 80 to 100 beats per minute. <span>Rashes Associated with Fever (Part 1) Children get many different kinds of rashes-many, though not all, related to infections. Below are descriptions and photos of rashes associated with fever. Cho Sooyoung - sooyoung.cho@mail.utoronto.ca 1/15 Enterovirus Usually erythematous and maculopapular, and may involve the palms and soles. Infrequently, it can be petechial. In hand-foot-and-mouth disease (caused by Coxsackie virus), presents as a vesicular rash on the hands and feet and with ulcers in the mouth. Usually seen in late summer and early fall. While the fever associated with enteroviruses may be high, it usually lasts only a few days. Erythema infectiosum Also called fifth disease, this is caused by parvovirus B19. There is frequently an associated low-grade fever (37.8-38.3 degrees C, or 100
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open itChildren get many different kinds of rashes-many, though not all, related to infections. Below are descriptions and photos of rashes associated with fever. Erythema infectiosum Also called fifth disease, this is caused by parvovirus B19. There is frequently an associated low-grade fever (37.8-38.3 degrees C, or 100-101 degrees F), with a rash appearing seven to ten days later. The characteristic rash star
Original toplevel document
CLIPP 11 - Kawasakipresents as a vesicular rash on the hands and feet and with ulcers in the mouth. Usually seen in late summer and early fall. While the fever associated with enteroviruses may be high, it usually lasts only a few days. <span>Erythema infectiosum Also called fifth disease, this is caused by parvovirus B19. There is frequently an associated low-grade fever (37.8-38.3 degrees C, or 100-101 degrees F), with a rash appearing seven to ten days later. The characteristic rash starts as facial erythema-the "slapped cheek" appearance. This can spread to the trunk and have an erythematous macular appearance. Central clearing of the rash appears, giving a lacy appearance. The rash often lasts longest on the extremities, where it has a lacy, reticular appearance. People with fifth disease can also develop pain and swelling in their joints (polyarthropathy syndrome). Individuals with underlying immune deficiencies who are exposed to this virus are at risk for developing aplastic anemia. Measles After a prodrome of fever (over 38.3 C, or 101 F), cough, coryza, and conjunctivitis, this maculopapular rash starts on the neck, behind the ears, and along
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open itfferent kinds of rashes-many, though not all, related to infections. Below are descriptions and photos of rashes associated with fever. Erythema infectiosum Also called fifth disease, this is caused by parvovirus B19. <span>There is frequently an associated low-grade fever (37.8-38.3 degrees C, or 100-101 degrees F), with a rash appearing seven to ten days later. The characteristic rash starts as facial erythema-the "slapped cheek" appearance. This can spread to the trunk and have an erythematous macular appearance. Cent
Original toplevel document
CLIPP 11 - Kawasakipresents as a vesicular rash on the hands and feet and with ulcers in the mouth. Usually seen in late summer and early fall. While the fever associated with enteroviruses may be high, it usually lasts only a few days. <span>Erythema infectiosum Also called fifth disease, this is caused by parvovirus B19. There is frequently an associated low-grade fever (37.8-38.3 degrees C, or 100-101 degrees F), with a rash appearing seven to ten days later. The characteristic rash starts as facial erythema-the "slapped cheek" appearance. This can spread to the trunk and have an erythematous macular appearance. Central clearing of the rash appears, giving a lacy appearance. The rash often lasts longest on the extremities, where it has a lacy, reticular appearance. People with fifth disease can also develop pain and swelling in their joints (polyarthropathy syndrome). Individuals with underlying immune deficiencies who are exposed to this virus are at risk for developing aplastic anemia. Measles After a prodrome of fever (over 38.3 C, or 101 F), cough, coryza, and conjunctivitis, this maculopapular rash starts on the neck, behind the ears, and along
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open itma infectiosum Also called fifth disease, this is caused by parvovirus B19. There is frequently an associated low-grade fever (37.8-38.3 degrees C, or 100-101 degrees F), with a rash appearing seven to ten days later. <span>The characteristic rash starts as facial erythema-the "slapped cheek" appearance. This can spread to the trunk and have an erythematous macular appearance. Central clearing of the rash appears, giving a lacy appearance. The rash often lasts longest on the e
Original toplevel document
CLIPP 11 - Kawasakipresents as a vesicular rash on the hands and feet and with ulcers in the mouth. Usually seen in late summer and early fall. While the fever associated with enteroviruses may be high, it usually lasts only a few days. <span>Erythema infectiosum Also called fifth disease, this is caused by parvovirus B19. There is frequently an associated low-grade fever (37.8-38.3 degrees C, or 100-101 degrees F), with a rash appearing seven to ten days later. The characteristic rash starts as facial erythema-the "slapped cheek" appearance. This can spread to the trunk and have an erythematous macular appearance. Central clearing of the rash appears, giving a lacy appearance. The rash often lasts longest on the extremities, where it has a lacy, reticular appearance. People with fifth disease can also develop pain and swelling in their joints (polyarthropathy syndrome). Individuals with underlying immune deficiencies who are exposed to this virus are at risk for developing aplastic anemia. Measles After a prodrome of fever (over 38.3 C, or 101 F), cough, coryza, and conjunctivitis, this maculopapular rash starts on the neck, behind the ears, and along
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open itis frequently an associated low-grade fever (37.8-38.3 degrees C, or 100-101 degrees F), with a rash appearing seven to ten days later. The characteristic rash starts as facial erythema-the "slapped cheek" appearance. <span>This can spread to the trunk and have an erythematous macular appearance. Central clearing of the rash appears, giving a lacy appearance. The rash often lasts longest on the extremities, where it has a lacy, reticular appearance. People with f
Original toplevel document
CLIPP 11 - Kawasakipresents as a vesicular rash on the hands and feet and with ulcers in the mouth. Usually seen in late summer and early fall. While the fever associated with enteroviruses may be high, it usually lasts only a few days. <span>Erythema infectiosum Also called fifth disease, this is caused by parvovirus B19. There is frequently an associated low-grade fever (37.8-38.3 degrees C, or 100-101 degrees F), with a rash appearing seven to ten days later. The characteristic rash starts as facial erythema-the "slapped cheek" appearance. This can spread to the trunk and have an erythematous macular appearance. Central clearing of the rash appears, giving a lacy appearance. The rash often lasts longest on the extremities, where it has a lacy, reticular appearance. People with fifth disease can also develop pain and swelling in their joints (polyarthropathy syndrome). Individuals with underlying immune deficiencies who are exposed to this virus are at risk for developing aplastic anemia. Measles After a prodrome of fever (over 38.3 C, or 101 F), cough, coryza, and conjunctivitis, this maculopapular rash starts on the neck, behind the ears, and along
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open it01 degrees F), with a rash appearing seven to ten days later. The characteristic rash starts as facial erythema-the "slapped cheek" appearance. This can spread to the trunk and have an erythematous macular appearance. <span>Central clearing of the rash appears, giving a lacy appearance. The rash often lasts longest on the extremities, where it has a lacy, reticular appearance. People with fifth disease can also develop pain and swelling in their joints&#
Original toplevel document
CLIPP 11 - Kawasakipresents as a vesicular rash on the hands and feet and with ulcers in the mouth. Usually seen in late summer and early fall. While the fever associated with enteroviruses may be high, it usually lasts only a few days. <span>Erythema infectiosum Also called fifth disease, this is caused by parvovirus B19. There is frequently an associated low-grade fever (37.8-38.3 degrees C, or 100-101 degrees F), with a rash appearing seven to ten days later. The characteristic rash starts as facial erythema-the "slapped cheek" appearance. This can spread to the trunk and have an erythematous macular appearance. Central clearing of the rash appears, giving a lacy appearance. The rash often lasts longest on the extremities, where it has a lacy, reticular appearance. People with fifth disease can also develop pain and swelling in their joints (polyarthropathy syndrome). Individuals with underlying immune deficiencies who are exposed to this virus are at risk for developing aplastic anemia. Measles After a prodrome of fever (over 38.3 C, or 101 F), cough, coryza, and conjunctivitis, this maculopapular rash starts on the neck, behind the ears, and along
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open ite characteristic rash starts as facial erythema-the "slapped cheek" appearance. This can spread to the trunk and have an erythematous macular appearance. Central clearing of the rash appears, giving a lacy appearance. <span>The rash often lasts longest on the extremities, where it has a lacy, reticular appearance. People with fifth disease can also develop pain and swelling in their joints (polyarthropathy syndrome). Individuals with underlying immune deficiencies who are exposed t
Original toplevel document
CLIPP 11 - Kawasakipresents as a vesicular rash on the hands and feet and with ulcers in the mouth. Usually seen in late summer and early fall. While the fever associated with enteroviruses may be high, it usually lasts only a few days. <span>Erythema infectiosum Also called fifth disease, this is caused by parvovirus B19. There is frequently an associated low-grade fever (37.8-38.3 degrees C, or 100-101 degrees F), with a rash appearing seven to ten days later. The characteristic rash starts as facial erythema-the "slapped cheek" appearance. This can spread to the trunk and have an erythematous macular appearance. Central clearing of the rash appears, giving a lacy appearance. The rash often lasts longest on the extremities, where it has a lacy, reticular appearance. People with fifth disease can also develop pain and swelling in their joints (polyarthropathy syndrome). Individuals with underlying immune deficiencies who are exposed to this virus are at risk for developing aplastic anemia. Measles After a prodrome of fever (over 38.3 C, or 101 F), cough, coryza, and conjunctivitis, this maculopapular rash starts on the neck, behind the ears, and along
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open itn spread to the trunk and have an erythematous macular appearance. Central clearing of the rash appears, giving a lacy appearance. The rash often lasts longest on the extremities, where it has a lacy, reticular appearance. <span>People with fifth disease can also develop pain and swelling in their joints (polyarthropathy syndrome). Individuals with underlying immune deficiencies who are exposed to this virus are at risk for developing aplastic anemia.<span><body><html>
Original toplevel document
CLIPP 11 - Kawasakipresents as a vesicular rash on the hands and feet and with ulcers in the mouth. Usually seen in late summer and early fall. While the fever associated with enteroviruses may be high, it usually lasts only a few days. <span>Erythema infectiosum Also called fifth disease, this is caused by parvovirus B19. There is frequently an associated low-grade fever (37.8-38.3 degrees C, or 100-101 degrees F), with a rash appearing seven to ten days later. The characteristic rash starts as facial erythema-the "slapped cheek" appearance. This can spread to the trunk and have an erythematous macular appearance. Central clearing of the rash appears, giving a lacy appearance. The rash often lasts longest on the extremities, where it has a lacy, reticular appearance. People with fifth disease can also develop pain and swelling in their joints (polyarthropathy syndrome). Individuals with underlying immune deficiencies who are exposed to this virus are at risk for developing aplastic anemia. Measles After a prodrome of fever (over 38.3 C, or 101 F), cough, coryza, and conjunctivitis, this maculopapular rash starts on the neck, behind the ears, and along
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open itg a lacy appearance. The rash often lasts longest on the extremities, where it has a lacy, reticular appearance. People with fifth disease can also develop pain and swelling in their joints (polyarthropathy syndrome). <span>Individuals with underlying immune deficiencies who are exposed to this virus are at risk for developing aplastic anemia.<span><body><html>
Original toplevel document
CLIPP 11 - Kawasakipresents as a vesicular rash on the hands and feet and with ulcers in the mouth. Usually seen in late summer and early fall. While the fever associated with enteroviruses may be high, it usually lasts only a few days. <span>Erythema infectiosum Also called fifth disease, this is caused by parvovirus B19. There is frequently an associated low-grade fever (37.8-38.3 degrees C, or 100-101 degrees F), with a rash appearing seven to ten days later. The characteristic rash starts as facial erythema-the "slapped cheek" appearance. This can spread to the trunk and have an erythematous macular appearance. Central clearing of the rash appears, giving a lacy appearance. The rash often lasts longest on the extremities, where it has a lacy, reticular appearance. People with fifth disease can also develop pain and swelling in their joints (polyarthropathy syndrome). Individuals with underlying immune deficiencies who are exposed to this virus are at risk for developing aplastic anemia. Measles After a prodrome of fever (over 38.3 C, or 101 F), cough, coryza, and conjunctivitis, this maculopapular rash starts on the neck, behind the ears, and along
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open itChildren get many different kinds of rashes-many, though not all, related to infections. Below are descriptions and photos of rashes associated with fever. Measles After a prodrome of fever (over 38.3 C, or 101 F), cough, coryza, and conjunctivitis, this maculopapular rash starts on the neck, behind the ears, and along the hairline. The rash spreads downward, reaching the feet in two or three days. The initial rash appears on the buccal mucosa as red lesions with bluish white spots in the center (kno
Original toplevel document
CLIPP 11 - Kawasakile with fifth disease can also develop pain and swelling in their joints (polyarthropathy syndrome). Individuals with underlying immune deficiencies who are exposed to this virus are at risk for developing aplastic anemia. <span>Measles After a prodrome of fever (over 38.3 C, or 101 F), cough, coryza, and conjunctivitis, this maculopapular rash starts on the neck, behind the ears, and along the hairline. The rash spreads downward, reaching the feet in two or three days. The initial rash appears on the buccal mucosa as red lesions with bluish white spots in the center (known as Koplik spots). These have frequently disappeared by the time the patient presents to medical attention. Immunization is very effective in preventing this infection. All photos in this case showing disease manifestations are courtesy of Gary Williams, MD, and the University of Wisconsin teaching file. Hyperlink "hands "
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open ithotos of rashes associated with fever. Measles After a prodrome of fever (over 38.3 C, or 101 F), cough, coryza, and conjunctivitis, this maculopapular rash starts on the neck, behind the ears, and along the hairline. <span>The rash spreads downward, reaching the feet in two or three days. The initial rash appears on the buccal mucosa as red lesions with bluish white spots in the center (known as Koplik spots). These have frequently disappeared by the time
Original toplevel document
CLIPP 11 - Kawasakile with fifth disease can also develop pain and swelling in their joints (polyarthropathy syndrome). Individuals with underlying immune deficiencies who are exposed to this virus are at risk for developing aplastic anemia. <span>Measles After a prodrome of fever (over 38.3 C, or 101 F), cough, coryza, and conjunctivitis, this maculopapular rash starts on the neck, behind the ears, and along the hairline. The rash spreads downward, reaching the feet in two or three days. The initial rash appears on the buccal mucosa as red lesions with bluish white spots in the center (known as Koplik spots). These have frequently disappeared by the time the patient presents to medical attention. Immunization is very effective in preventing this infection. All photos in this case showing disease manifestations are courtesy of Gary Williams, MD, and the University of Wisconsin teaching file. Hyperlink "hands "
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open ite of fever (over 38.3 C, or 101 F), cough, coryza, and conjunctivitis, this maculopapular rash starts on the neck, behind the ears, and along the hairline. The rash spreads downward, reaching the feet in two or three days. <span>The initial rash appears on the buccal mucosa as red lesions with bluish white spots in the center (known as Koplik spots). These have frequently disappeared by the time the patient presents to medical attention. Immunization is very effective in preventing this infection.<span><body><html>
Original toplevel document
CLIPP 11 - Kawasakile with fifth disease can also develop pain and swelling in their joints (polyarthropathy syndrome). Individuals with underlying immune deficiencies who are exposed to this virus are at risk for developing aplastic anemia. <span>Measles After a prodrome of fever (over 38.3 C, or 101 F), cough, coryza, and conjunctivitis, this maculopapular rash starts on the neck, behind the ears, and along the hairline. The rash spreads downward, reaching the feet in two or three days. The initial rash appears on the buccal mucosa as red lesions with bluish white spots in the center (known as Koplik spots). These have frequently disappeared by the time the patient presents to medical attention. Immunization is very effective in preventing this infection. All photos in this case showing disease manifestations are courtesy of Gary Williams, MD, and the University of Wisconsin teaching file. Hyperlink "hands "
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open itree days. The initial rash appears on the buccal mucosa as red lesions with bluish white spots in the center (known as Koplik spots). These have frequently disappeared by the time the patient presents to medical attention. <span>Immunization is very effective in preventing this infection.<span><body><html>
Original toplevel document
CLIPP 11 - Kawasakile with fifth disease can also develop pain and swelling in their joints (polyarthropathy syndrome). Individuals with underlying immune deficiencies who are exposed to this virus are at risk for developing aplastic anemia. <span>Measles After a prodrome of fever (over 38.3 C, or 101 F), cough, coryza, and conjunctivitis, this maculopapular rash starts on the neck, behind the ears, and along the hairline. The rash spreads downward, reaching the feet in two or three days. The initial rash appears on the buccal mucosa as red lesions with bluish white spots in the center (known as Koplik spots). These have frequently disappeared by the time the patient presents to medical attention. Immunization is very effective in preventing this infection. All photos in this case showing disease manifestations are courtesy of Gary Williams, MD, and the University of Wisconsin teaching file. Hyperlink "hands "
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open itChildren get many different kinds of rashes-many, though not all, related to infections. Below are descriptions and photos of rashes associated with fever. Scarlet fever This rash, caused by infection with group A Streptococcus, consists of very fine papules, often described as feeling like sandpaper. It is erythematous, but blanches. The rash starts in the groin, axillae, and neck, but rapidly spreads. The fever can be high, and the disease is usually self-limited, la
Original toplevel document
CLIPP 11 - Kawasakis and neck. There is usually less involvement of the face and legs. The rash is preceded by three or four days of high fevers, which end as the rash appears. Usually seen in children less than two years old. 3/15 <span>Scarlet fever This rash, caused by infection with group A Streptococcus, consists of very fine papules, often described as feeling like sandpaper. It is erythematous, but blanches. The rash starts in the groin, axillae, and neck, but rapidly spreads. The fever can be high, and the disease is usually self-limited, lasting less than 10 days. It is important to treat with antibiotics to prevent non-suppurative complications of strep, including rheumatic fever. Varicella The rash, also known as chicken pox, starts on the trunk and spreads to the extremities and head. Each lesion progresses from an erythematous macule to pap
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open itns. Below are descriptions and photos of rashes associated with fever. Scarlet fever This rash, caused by infection with group A Streptococcus, consists of very fine papules, often described as feeling like sandpaper. <span>It is erythematous, but blanches. The rash starts in the groin, axillae, and neck, but rapidly spreads. The fever can be high, and the disease is usually self-limited, lasting less than 10 days. It i
Original toplevel document
CLIPP 11 - Kawasakis and neck. There is usually less involvement of the face and legs. The rash is preceded by three or four days of high fevers, which end as the rash appears. Usually seen in children less than two years old. 3/15 <span>Scarlet fever This rash, caused by infection with group A Streptococcus, consists of very fine papules, often described as feeling like sandpaper. It is erythematous, but blanches. The rash starts in the groin, axillae, and neck, but rapidly spreads. The fever can be high, and the disease is usually self-limited, lasting less than 10 days. It is important to treat with antibiotics to prevent non-suppurative complications of strep, including rheumatic fever. Varicella The rash, also known as chicken pox, starts on the trunk and spreads to the extremities and head. Each lesion progresses from an erythematous macule to pap
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open ittos of rashes associated with fever. Scarlet fever This rash, caused by infection with group A Streptococcus, consists of very fine papules, often described as feeling like sandpaper. It is erythematous, but blanches. <span>The rash starts in the groin, axillae, and neck, but rapidly spreads. The fever can be high, and the disease is usually self-limited, lasting less than 10 days. It is important to treat with antibiotics to prevent non-suppurative compl
Original toplevel document
CLIPP 11 - Kawasakis and neck. There is usually less involvement of the face and legs. The rash is preceded by three or four days of high fevers, which end as the rash appears. Usually seen in children less than two years old. 3/15 <span>Scarlet fever This rash, caused by infection with group A Streptococcus, consists of very fine papules, often described as feeling like sandpaper. It is erythematous, but blanches. The rash starts in the groin, axillae, and neck, but rapidly spreads. The fever can be high, and the disease is usually self-limited, lasting less than 10 days. It is important to treat with antibiotics to prevent non-suppurative complications of strep, including rheumatic fever. Varicella The rash, also known as chicken pox, starts on the trunk and spreads to the extremities and head. Each lesion progresses from an erythematous macule to pap
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open itsed by infection with group A Streptococcus, consists of very fine papules, often described as feeling like sandpaper. It is erythematous, but blanches. The rash starts in the groin, axillae, and neck, but rapidly spreads. <span>The fever can be high, and the disease is usually self-limited, lasting less than 10 days. It is important to treat with antibiotics to prevent non-suppurative complications of strep, including rheumatic fever.<span><body><html>
Original toplevel document
CLIPP 11 - Kawasakis and neck. There is usually less involvement of the face and legs. The rash is preceded by three or four days of high fevers, which end as the rash appears. Usually seen in children less than two years old. 3/15 <span>Scarlet fever This rash, caused by infection with group A Streptococcus, consists of very fine papules, often described as feeling like sandpaper. It is erythematous, but blanches. The rash starts in the groin, axillae, and neck, but rapidly spreads. The fever can be high, and the disease is usually self-limited, lasting less than 10 days. It is important to treat with antibiotics to prevent non-suppurative complications of strep, including rheumatic fever. Varicella The rash, also known as chicken pox, starts on the trunk and spreads to the extremities and head. Each lesion progresses from an erythematous macule to pap
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open iteeling like sandpaper. It is erythematous, but blanches. The rash starts in the groin, axillae, and neck, but rapidly spreads. The fever can be high, and the disease is usually self-limited, lasting less than 10 days. <span>It is important to treat with antibiotics to prevent non-suppurative complications of strep, including rheumatic fever.<span><body><html>
Original toplevel document
CLIPP 11 - Kawasakis and neck. There is usually less involvement of the face and legs. The rash is preceded by three or four days of high fevers, which end as the rash appears. Usually seen in children less than two years old. 3/15 <span>Scarlet fever This rash, caused by infection with group A Streptococcus, consists of very fine papules, often described as feeling like sandpaper. It is erythematous, but blanches. The rash starts in the groin, axillae, and neck, but rapidly spreads. The fever can be high, and the disease is usually self-limited, lasting less than 10 days. It is important to treat with antibiotics to prevent non-suppurative complications of strep, including rheumatic fever. Varicella The rash, also known as chicken pox, starts on the trunk and spreads to the extremities and head. Each lesion progresses from an erythematous macule to pap
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
"HEADDS" Up on Talking With Teenagers
ocial information that is important for maintaining a teenager's well-being. BUILDING RAPPORT The opening vignette underscores the importance of the following measures in establishing rapport with a teenager: •<span>When you enter the examination room, introduce yourself to the teenager first and shake hands before addressing the parent (if present). •Take the history while the teenager is dressed and ask him to disrobe only for the examination. •Face the adolescent and maintain eye contact as much as possible
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
"HEADDS" Up on Talking With Teenagers
and maintain eye contact as much as possible while listening to the parent. If the teenager perceives that he is the central person in the doctor- patient relationship, he will feel respected and will be more likely to trust you. •<span>When the parent has a laundry list of concerns, make sure to interject occasionally and politely ask the adolescent whether he shares those concerns, which can be addressed one-on-one with the teenager later in the visit. With a new patient and family, I find it invaluable to discuss confidentiality up front. I usually say, "At this office, we encourage teens be honest with their doctor.
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
"HEADDS" Up on Talking With Teenagers
3; •When the parent has a laundry list of concerns, make sure to interject occasionally and politely ask the adolescent whether he shares those concerns, which can be addressed one-on-one with the teenager later in the visit. <span>With a new patient and family, I find it invaluable to discuss confidentiality up front. I usually say, "At this office, we encourage teens be honest with their doctor. It helps ensure that health concerns and questions are addressed. It also helps teens prepare for a rapidly approaching adulthood, when they will have to know how to discuss health concerns with their physician. Occasionally, we discuss sensitive issues such as sexuality and drugs and, for the most part, we agree to keep these conversations private. We expect teens to ask questions that will ultimately keep them healthy and safe." I also discuss the contingencies of when confidentiality must be broken. Specifically, I explain that when there are issues that may put the teen's (or someone else's) life o
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
"HEADDS" Up on Talking With Teenagers
an. Occasionally, we discuss sensitive issues such as sexuality and drugs and, for the most part, we agree to keep these conversations private. We expect teens to ask questions that will ultimately keep them healthy and safe." <span>I also discuss the contingencies of when confidentiality must be broken. Specifically, I explain that when there are issues that may put the teen's (or someone else's) life or health at risk, confidentiality must be broken and adults must be brought in who can help keep him/her safe. I tell the adolescent that I never break confidentiality without telling him first. The teen always has the option to decide how he would like the parent to find out. THE "HEADDS" SCREENING TOOL The "HEADDS" mnemonic reminds clinicians about the psychosocial factors that influence the physical and emotional w
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
"HEADDS" Up on Talking With Teenagers
"HEADDS" mnemonic reminds clinicians about the psychosocial factors that influence the physical and emotional well-being of teenagers. This is a helpful screening tool for identifying potential problems and risk factors. <span>Home •Try to get a general picture . . . Who lives with the patient? Does the family live in a house? Cramped quarters? Does the adolescent have any privacy? •Do the parents live together? If not, is the out-of-house parent involved with the patient--and to what extent? •Have there been recent changes in the family dynamic--a new sibling, the death of a close grandparent, a parental separation or divorce? Is a family member sick? If so, how is this affecting the patient? •How many siblings live at home and where in the birth order is the patient? In some large families, the responsibilities for younger children may fall on the oldest child. This level of responsibility may seem appropriate or it may overwhelm the teen. These questions are best asked when the parent is present so that objective information (that can be discussed with the teen alone) can be obtained. Education Many busy practitioners hesitate to explore issues about education because they believe that this is outside their domain. I would argue that avoiding a
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
"HEADDS" Up on Talking With Teenagers
oners hesitate to explore issues about education because they believe that this is outside their domain. I would argue that avoiding a discussion about school performance prevents a real understanding of any underlying issues facing the teen. <span>School is the adolescent's primary job, and almost all teens want to succeed. When things are going poorly in school, I see this as a manifestation of some other process that is inhibiting success. Such processes frequently include ADHD, learning disabilities, depression, anxiety, bullying, or school phobia. It can be immensely helpful to ask the teen how well school is going while the parent is in the room. Teens often report that everything is "fine"; parents may coun
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
"HEADDS" Up on Talking With Teenagers
When things are going poorly in school, I see this as a manifestation of some other process that is inhibiting success. Such processes frequently include ADHD, learning disabilities, depression, anxiety, bullying, or school phobia. <span>It can be immensely helpful to ask the teen how well school is going while the parent is in the room. Teens often report that everything is "fine"; parents may counter that the adolescent has been skipping classes or is earning poor grades. Some other key issues to inquire about: •Have there been any changes (for better or worse) in the teen's academic progress during the past year? •If the
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
"HEADDS" Up on Talking With Teenagers
helpful to ask the teen how well school is going while the parent is in the room. Teens often report that everything is "fine"; parents may counter that the adolescent has been skipping classes or is earning poor grades. <span>Some other key issues to inquire about: •Have there been any changes (for better or worse) in the teen's academic progress during the past year? •If the teen is doing poorly, find out why. Does he have difficulty paying attention in class or during homework time? Do homework assignments take forever to complete? Positive answers suggest the possibility of ADHD. •Have teachers mentioned any problems with the student's ability to learn, digest, and understand information? Positive answers suggest possible learning disabilities. In this situation, the student might benefit from psychoeducational testing and/or the development of an individualized education plan. •Is the student skipping classes? Has he joined a new peer group? Do the parents suspect any drug or alcohol use? Any significant mood changes recently? Could there be an underlying mood disorder (depression, anxiety) that prevents the student from focusing? •Is the student having trouble waking up to get to school on time? Is he falling asleep in class? Are homework assignments incomplete because the student sleeps for hours each afternoon or early evening? The duration and quality of sleep can profoundly influence an adolescent's academic performance and should be addressed whenever academic concerns arise. •What are the student's life plans and goals? Younger teenagers may simply want to be a "pro basketball player," a developmentally appropriate goal. By high school, there should be some discussions about the teen's post-high school plans. If the student is planning on going to college, is he pursuing the academics and activities necessary to meet this goal? Be on the lookout for the adolescent with strong cognitive abilities who is faltering academically. An evaluation for mood disorders, substance abuse, ADHD, or learning disab
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
"HEADDS" Up on Talking With Teenagers
meet this goal? Be on the lookout for the adolescent with strong cognitive abilities who is faltering academically. An evaluation for mood disorders, substance abuse, ADHD, or learning disabilities is usually warranted. <span>Activities After-school activities (or lack thereof) can profoundly affect an adolescent's physical well-being. I generally obtain this history without the parent in the room because the teen usually answers more honestly. If the history suggests participation in an activity that could be detrimental to the patient's health, this may warrant a private or a 3-way discussion with the parent. Other key points to ask about: •What activities does the teen participate in after school? Most adolescents need to be involved with some activity in addition to academics. Watching TV or Internet chatting all afternoon does not count as a healthy activity. The American Academy of Pediatrics recommends no more than 1 to 2 hours each day of "screen time." •Simple "chilling" and "hanging out" generally spell trouble. With whom does the adolescent spend time? Is he home alone with a girlfriend or out on the street with peers? If an adolescent spends afternoons alone every day, some investigation of possible mood disorder or social issues is warranted. The adolescent who naps for 2 to 3 hours every afternoon may require an evaluation for depression, substance use, or sleep cycle disorders. Overactivity also needs to be identified. Teenagers (like everyone else) need time to relax and have fun. Some teens (or their parents) may require a friendly "prescription" from the doctor instructing them to incorporate this into their busy schedules. Drugs and Drinking There is no one "right" way to approach the topic, but the following tactics can be helpful: •Start with a generalized conv
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
"HEADDS" Up on Talking With Teenagers
entified. Teenagers (like everyone else) need time to relax and have fun. Some teens (or their parents) may require a friendly "prescription" from the doctor instructing them to incorporate this into their busy schedules. <span>Drugs and Drinking There is no one "right" way to approach the topic, but the following tactics can be helpful: •Start with a generalized conversation and open-ended questions: eg, "Many of my teenage patients tell me their friends sometimes try drugs and alcohol. What kinds of things have your friends talked about trying?" •As the adolescent answers, start bringing the conversation closer to home. "It must be a challenge for you to be at a party where your friends are drinking and getting drunk. How do you deal with it when they offer you (or pressure you with) something to drink?" •Congratulate the teen who continually insists that he has never indulged in any of these substances for making good, mature decisions for his health. •If the teen admits to trying various substances, be careful not to sound judgmental. Explore the benefits (and consequences) the teen gets from the substance use, how it makes him feel the next day, how often he is using the substance. •When you identify a substance use problem, encourage a follow-up appointment. Let the teen know that you can see why he is attracted to the substance, but that you have concerns for his safety. •Suspected habitual substance use by a teenager who will not follow up with you constitutes a safety issue that requires breaking confidentiality. Sex and Sexuality Addressing sexual development can help prevent unplanned pregnancies, sexually transmitted infections, and HIV/AIDS. Data consistently indicate t
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
"HEADDS" Up on Talking With Teenagers
attractions or experiences. Many adolescents who are unsure of their sexual orientation tend to avoid labels such as "gay," "lesbian," or "bisexual." A good way to broach this topic with a male teenager might be: <span>"I see lots of teenagers, and we frequently talk about sex. Some like girls, some like guys, some like both, and some are just not sure. When you think about dating or having sex, do you think about guys, girls, or both?" •Patients frequently use slang to describe genitalia or different kinds of sexual activity. If you are unsure, ask for clarification. •Teens hate lectures. Rather
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
"HEADDS" Up on Talking With Teenagers
you think about dating or having sex, do you think about guys, girls, or both?" •Patients frequently use slang to describe genitalia or different kinds of sexual activity. If you are unsure, ask for clarification. •<span>Teens hate lectures. Rather than lecturing on safer sex, involve the teen in a discussion on how he would approach various situations. For example, ask a female patient how she would negotiate not having sex with a partner who did not have a condom. Ask a teenage boy how he might behave if he was about to have intercourse and his girlfriend changed her mind. Suicidality and Mental Health The following approach can help you quickly assess the patient's mood and mental health status: •Explain that many teenage
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
"HEADDS" Up on Talking With Teenagers
emotions during adolescence that can sometimes make them feel "out of control." •Ask about mood-related symptoms. Does the teen feel "down" more often than his friends do? How many days a week is he happy? Sad? <span>Inquire about persistent irritability--a presenting symptom of depression in teens. •Ask about fatigue and/or inability to fall asleep. Does the patient wake early in the morning, unable to get back to sleep? Has his appetite changed recently? •Do
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Highlight doc Day 2 - maltx
MALTREATMENT: phys/emo/sex/neglect/exploitationàactual/potential harm to child’s health/survival/development/dignity within relationship of responsibility/trust/power Child isn't walking, but XR shows spiral fracture in femur. What's next? MCQ : full body XR Suspected child abuse: when are you suspicious, what t
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Highlight doc Day 2 - maltx
MALTREATMENT: phys/emo/sex/neglect/exploitationàactual/potential harm to child’s health/survival/development/dignity within relationship of responsibility/trust/power Child isn't walking, but XR shows spiral fracture in femur. What's next? MCQ : full body XR Suspected child abuse: when are you suspicious, what to ask on Hx, and what is Tx? Red Flags: inj inconsistent w/ hx (mechanism, force, age/developmental stag
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Highlight doc Day 2 - maltx
ity/trust/power Child isn't walking, but XR shows spiral fracture in femur. What's next? MCQ : full body XR Suspected child abuse: when are you suspicious, what to ask on Hx, and what is Tx? <span>Red Flags: inj inconsistent w/ hx (mechanism, force, age/developmental stage), hx inconsistent/changes, medical attn delay, multiple inj, different age inj, bruises (non-amb bruises, well-cushioned, patterned), # (non-amb, different ages, location) Fractures: metaphyseal/ribs/scapula/vertebrae/sternum/mult skull #s Hx: events leading up to injury Location & time, who present, detailed events, child’s response, caregiver’s response, other children at risk, rel
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Highlight doc Day 2 - maltx
cal attn delay, multiple inj, different age inj, bruises (non-amb bruises, well-cushioned, patterned), # (non-amb, different ages, location) Fractures: metaphyseal/ribs/scapula/vertebrae/sternum/mult skull #s <span>Hx: events leading up to injury Location & time, who present, detailed events, child’s response, caregiver’s response, other children at risk, relevant PHx Thorough O/E (completely undress): head, skin (ears, genitalia, buttocks), neuro (fontanelle, HC, fundi), mouth (frenulum), abdo, msk (swelling, pain), g/u (by specialized team
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Highlight doc Day 2 - maltx
scapula/vertebrae/sternum/mult skull #s Hx: events leading up to injury Location & time, who present, detailed events, child’s response, caregiver’s response, other children at risk, relevant PHx <span>Thorough O/E (completely undress): head, skin (ears, genitalia, buttocks), neuro (fontanelle, HC, fundi), mouth (frenulum), abdo, msk (swelling, pain), g/u (by specialized team) Palpate everywhere Document all injuries on a body diagram: type, location, size, shape, colour, pattern Photography of skin injuries is ideal (police or hospital camera) Ix (suspected non-accide
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Highlight doc Day 2 - maltx
at risk, relevant PHx Thorough O/E (completely undress): head, skin (ears, genitalia, buttocks), neuro (fontanelle, HC, fundi), mouth (frenulum), abdo, msk (swelling, pain), g/u (by specialized team) Palpate everywhere <span>Document all injuries on a body diagram: type, location, size, shape, colour, pattern Photography of skin injuries is ideal (police or hospital camera) Ix (suspected non-accidental in non-ambulating children/infants): skeletal survey (all <2yo if NAI suspected), CT h
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Highlight doc Day 2 - maltx
), abdo, msk (swelling, pain), g/u (by specialized team) Palpate everywhere Document all injuries on a body diagram: type, location, size, shape, colour, pattern Photography of skin injuries is ideal (police or hospital camera) <span>Ix (suspected non-accidental in non-ambulating children/infants): skeletal survey (all <2yo if NAI suspected), CT head, direct ophthalmoscopy, labs for occult trauma (AST, ALT, lipase, UA) Fractures: bone density on XR, Ca 2+ , Mg 2+ , Phos, ALP, PTH, VIT D Ddx: accidental inj, osteogenesis imperfecta, Menkes dz, osteopenia (rickets, prematurity, meds), os
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Highlight doc Day 2 - maltx
uries is ideal (police or hospital camera) Ix (suspected non-accidental in non-ambulating children/infants): skeletal survey (all <2yo if NAI suspected), CT head, direct ophthalmoscopy, labs for occult trauma (AST, ALT, lipase, UA) <span>Fractures: bone density on XR, Ca 2+ , Mg 2+ , Phos, ALP, PTH, VIT D Ddx: accidental inj, osteogenesis imperfecta, Menkes dz, osteopenia (rickets, prematurity, meds), osteomyelitis, bone tumours Bruising: CBC, diff, smear, INR, PTT, von Willebrand, clotting factors VII, IX, X, XIII. Ddx: accidental inj, bleeding d/o (ITP, thrombocytopenia, hemophilia),
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Highlight doc Day 2 - maltx
T, lipase, UA) Fractures: bone density on XR, Ca 2+ , Mg 2+ , Phos, ALP, PTH, VIT D Ddx: accidental inj, osteogenesis imperfecta, Menkes dz, osteopenia (rickets, prematurity, meds), osteomyelitis, bone tumours <span>Bruising: CBC, diff, smear, INR, PTT, von Willebrand, clotting factors VII, IX, X, XIII. Ddx: accidental inj, bleeding d/o (ITP, thrombocytopenia, hemophilia), connective tissue d/o (Ehlers Danlos), Mongolian spots, folk healing practices, phytophotodermatitis, ink/paint Intracranial bleed: bruising workup + urine organic acids head trauma often missed b/c: non-specific sx’s (vomiting, crying, irritable) Sexual abuse: STIs r/o o
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Highlight doc Day 2 - maltx
llebrand, clotting factors VII, IX, X, XIII. Ddx: accidental inj, bleeding d/o (ITP, thrombocytopenia, hemophilia), connective tissue d/o (Ehlers Danlos), Mongolian spots, folk healing practices, phytophotodermatitis, ink/paint <span>Intracranial bleed: bruising workup + urine organic acids head trauma often missed b/c: non-specific sx’s (vomiting, crying, irritable) Sexual abuse: STIs r/o other causes (ddx) CAS duties: 1) report (reasonable grounds to suspect needs protection) 2) ongoing report (additional reasonable grounds) 3) no delega
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Highlight doc Day 2 - maltx
ctices, phytophotodermatitis, ink/paint Intracranial bleed: bruising workup + urine organic acids head trauma often missed b/c: non-specific sx’s (vomiting, crying, irritable) Sexual abuse: STIs r/o other causes (ddx) <span>CAS duties: 1) report (reasonable grounds to suspect needs protection) 2) ongoing report (additional reasonable grounds) 3) no delegation àinvestigation (CAS (safety) + police (criminal charges)) How to report Provide basis for suspicion, address, religion, relationship w/ offender, other children A father is known to hit his son for disciplin
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Highlight doc Day 2 - maltx
: STIs r/o other causes (ddx) CAS duties: 1) report (reasonable grounds to suspect needs protection) 2) ongoing report (additional reasonable grounds) 3) no delegation àinvestigation (CAS (safety) + police (criminal charges)) <span>How to report Provide basis for suspicion, address, religion, relationship w/ offender, other children A father is known to hit his son for discipline. The child says his dad hits him with a ruler. Father says he hits his son only with a hand. How can you tell O/E
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Highlight doc Day 2 - maltx
l reasonable grounds) 3) no delegation àinvestigation (CAS (safety) + police (criminal charges)) How to report Provide basis for suspicion, address, religion, relationship w/ offender, other children <span>A father is known to hit his son for discipline. The child says his dad hits him with a ruler. Father says he hits his son only with a hand. How can you tell O/E how the child was hit? Is this discipline or child abuse? O/E: shape of imprint/bruise, type of injury Abuse: potentially meets definition (depends on injury) Child abuse (2 MCQ questions, what tests would you do; can't remember scenario) (See above) You "see bruises on infant" and also that t
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Highlight doc Day 3 - imm
2 DTaP-IPV-Hib Pneu-C-13 Rot-1 4 DTaP-IPV-Hib Pneu-C-13 Rot-1 6 DTaP-IPV-Hib 12 Men-C-C Pneu-C-13 MMR 15 Var 18 DTaP-IPV-Hib 4-6 Tdap-IPV MMRV Gr 7 Men-C-ACYW HPV-4 HB 14-16 Tdap Yr Infl Live (MMR + V)àSC Td q10y >24, Pneu q5y, shingles >65 HEALTH SUPERVISION IMMUNIZATIONS ( know Ontario immunization schedule) All IM excl MMR & V (SC) & Rota (oral)
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Highlight doc Day 3 - imm
MMR 15 Var 18 DTaP-IPV-Hib 4-6 Tdap-IPV MMRV Gr 7 Men-C-ACYW HPV-4 HB 14-16 Tdap Yr Infl Live (MMR + V)àSC Td q10y >24, Pneu q5y, shingles >65 HEALTH SUPERVISION <span>IMMUNIZATIONS ( know Ontario immunization schedule) All IM excl MMR & V (SC) & Rota (oral) “Do vaccines cause ASD?” How do you advise the parents? Discuss how you would calm mom's fear of autism in a child receiving MMR. Unders
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Highlight doc Day 3 - imm
y >24, Pneu q5y, shingles >65 HEALTH SUPERVISION IMMUNIZATIONS ( know Ontario immunization schedule) All IM excl MMR & V (SC) & Rota (oral) <span>“Do vaccines cause ASD?” How do you advise the parents? Discuss how you would calm mom's fear of autism in a child receiving MMR. Understand concern: worries, understanding of dz risks & Vaccine benefits & risks, validate why may have belief if concerned re: ASD, discuss how original info was fraud & no evidence to support link; give anecdotes of children affected by vaccine-preventable dz’s stick to msg: vaccines are safe & effective & serious dz can be prevented w/ imm vaccine benefits & risks, herd protection not 100% (tetanus from soil), ‘wait and see’ not good b/c many need mult doses & take time to protect vaccine safety system: held to higher safety standard than drugs, usually approved in Canada after use in other countries address pain assc w/ imm don’t dismiss from practice if parents refuse: majority of parents accept when concerns addressed Adverse reaction of MMR vaccine? (give 3) MMR: measles rash (7-14d), ITP, parotitis, febrile seizure Local : induration, tenderness, redness, swe
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Highlight doc Day 3 - imm
stem: held to higher safety standard than drugs, usually approved in Canada after use in other countries address pain assc w/ imm don’t dismiss from practice if parents refuse: majority of parents accept when concerns addressed <span>Adverse reaction of MMR vaccine? (give 3) MMR: measles rash (7-14d), ITP, parotitis, febrile seizure Local : induration, tenderness, redness, swelling Allergic : urticaria, rhinitis, anaphylaxis Systemic : ↑T, rash, irritability, lymphadenopathy, arthr/myalgia, arthritis CIs: moderate/severe illness ± fever (not mild URTI) , component allergy During a 6mo ♀ wellness visit, which diseases is the child being inoculated against (3 marks; there are five diseases, which opens up the possibility that I am wron
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Highlight doc Day 3 - imm
against (3 marks; there are five diseases, which opens up the possibility that I am wrong)? Name the AEs of such a vaccine (3 marks). Diphtheria, tetanus, pertussis (whooping cough), polio, Haemophilus influenzae type B (Hib) <span>AEs: serious s/e rare. Mild pain, swelling, redness x few days at site. Some get fever/rash/lose appetite/fussy/drowsy x1-2d after shot (acetaminophen to prevent pain & fever). Mother being counselled about HPV vaccine. Which of the following are correct? protects against genital warts
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Highlight doc Day 3 - imm
ugh), polio, Haemophilus influenzae type B (Hib) AEs: serious s/e rare. Mild pain, swelling, redness x few days at site. Some get fever/rash/lose appetite/fussy/drowsy x1-2d after shot (acetaminophen to prevent pain & fever). <span>Mother being counselled about HPV vaccine. Which of the following are correct? protects against genital warts T (not 100%) HPV causes cervical and anal cancer T (HPV 16,18) most of us will get the infection and clear it on our own F (10% incidence) injection at 0, 2, 6 months T (0, 1-2, 6) side effects are common F protects against four high-risk subtypes F (not HPV 6,11) doesn’t require yearly paps T (q3y) average time from acquiring high-risk genotype to cancer is 30-40 y F (15y) Which vaccination should an 11yo ♀ get before leaving for summer school? I answered DTaP booster. Hepatitis B, and meningococcal C 15mo well-baby
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Growth
se • Provide education about age‐appropriate foods, mealtime scheduling and behaviour • Caloric fortification of food • May need referral to dietitian, social work Overweight and Obesity Introduction • <span>Growth monitoring should be performed at primary care visits for children and youth ages 17 and younger • BMI = mass (kg) / height (m2) o WHO Growth Charts for Canada are recommended which have different cutpoints for the definition of overweight and obesity than the U
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Growth
fication of food • May need referral to dietitian, social work Overweight and Obesity Introduction • Growth monitoring should be performed at primary care visits for children and youth ages 17 and younger • <span>BMI = mass (kg) / height (m2) o WHO Growth Charts for Canada are recommended which have different cutpoints for the definition of overweight and obesity than the US‐based CDC charts • Cut‐off poi
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Growth
WHO Growth Charts for Canada are recommended which have different cutpoints for the definition of overweight and obesity than the US‐based CDC charts • Cut‐off points for overweight and obese depend on age and BMI (WHO) o <span>Birth to 2 years ‐ Risk of overweight – Weight for length > 85th ‐ Overweight – Weight for length > 97th ‐ Obese – Weight for length > 99.9th o 2 to 5 years ‐ Risk of overweight – BMI > 85th ‐ Overweight – BMI > 97th ‐ Obese – BMI > 99.9th o 5 to 19 years ‐ Overweight – BMI > 85th
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Growth
ff points for overweight and obese depend on age and BMI (WHO) o Birth to 2 years ‐ Risk of overweight – Weight for length > 85th ‐ Overweight – Weight for length > 97th ‐ Obese – Weight for length > 99.9th o <span>2 to 5 years ‐ Risk of overweight – BMI > 85th ‐ Overweight – BMI > 97th ‐ Obese – BMI > 99.9th o 5 to 19 years ‐ Overweight – BMI > 85th ‐ Obese – BMI > 97th ‐ Severely obese – BMI > 99.9th • Over 60% of overweight children will have at least one
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Growth
ength > 85th ‐ Overweight – Weight for length > 97th ‐ Obese – Weight for length > 99.9th o 2 to 5 years ‐ Risk of overweight – BMI > 85th ‐ Overweight – BMI > 97th ‐ Obese – BMI > 99.9th o <span>5 to 19 years ‐ Overweight – BMI > 85th ‐ Obese – BMI > 97th ‐ Severely obese – BMI > 99.9th • Over 60% of overweight children will have at least one CV risk factor History • What concerns, if any, do you have about your child’s weight? When did weight
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Growth
ears ‐ Risk of overweight – BMI > 85th ‐ Overweight – BMI > 97th ‐ Obese – BMI > 99.9th o 5 to 19 years ‐ Overweight – BMI > 85th ‐ Obese – BMI > 97th ‐ Severely obese – BMI > 99.9th • <span>Over 60% of overweight children will have at least one CV risk factor History • What concerns, if any, do you have about your child’s weight? When did weight gain start? Has gain been slow over time or sudden? • What, if any, pas
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Growth
#13; ‐ Obese – BMI > 99.9th o 5 to 19 years ‐ Overweight – BMI > 85th ‐ Obese – BMI > 97th ‐ Severely obese – BMI > 99.9th • Over 60% of overweight children will have at least one CV risk factor <span>History • What concerns, if any, do you have about your child’s weight? When did weight gain start? Has gain been slow over time or sudden? • What, if any, past attempts at weight loss have been made? • Review of systems for comorbidities and etiologies of obesity: o Headaches, blurred vision (hypertension, intracranial hypertension) o Breathing pauses when sleeping, snoring, daytime sleepiness (OSA) o Joint pain (slipped femoral capital epiphysis, blount disease) o Menstrual history, hirsutism, acne (hyperandrogenism, PCOS) o Polyuria, nocturia (T2DM) o Increased fatigue, cold intolerance, constipation, dry skin (hypothyroidism) o Stunted growth, striae (Cushing’s) • Family History o Identify obesity in first degree relatives o Evaluate history of cardiovascular disease, type 2 DM, cancer in first degree or second‐degree relatives • Diet o Identify caretakers who feed the child o Identify foods high in calories and low in nutritional value that can be reduced, eliminated, or replaced o Assess eating patterns (e.g. timing, content, location of meals and snacks) o Estimate the type and quantity of beverage intake (sugar sweetened beverages, juice, pop) o Frequency of dining out • Activity o Identify barriers to walking or riding a bike to school o Evaluate time spent in play o Evaluate school recess and physical education (frequency, duration and intensity) o Assess after‐school and weekend activities o Assess screen time (television, computer, movies, video games) • Assess psychological impact of weight on child (bullying, depression, anxiety, social isolation etc.) Physical Exam • Obtain and plot weight, height, BMI on WHO Growth Charts for Canada Complete physical exam • Findings to look for o Hypertension o En
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Growth
3; o Assess after‐school and weekend activities o Assess screen time (television, computer, movies, video games) • Assess psychological impact of weight on child (bullying, depression, anxiety, social isolation etc.) <span>Physical Exam • Obtain and plot weight, height, BMI on WHO Growth Charts for Canada Complete physical exam • Findings to look for o Hypertension o Enlarged thyroid o Acanthosis nigricans (insulin resistance) o Striae o Hepatomegaly o Hirsutism o Hip/knee pain or decreased ROM (Blounts, SCFE) o Sexual maturity rating Investigations • Investigations can be performed for children who meet cut‐off point for obesity • Lipid profile, glucose, HbA1C • Liver enzymes (specific
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Growth
for o Hypertension o Enlarged thyroid o Acanthosis nigricans (insulin resistance) o Striae o Hepatomegaly o Hirsutism o Hip/knee pain or decreased ROM (Blounts, SCFE) o Sexual maturity rating <span>Investigations • Investigations can be performed for children who meet cut‐off point for obesity • Lipid profile, glucose, HbA1C • Liver enzymes (specifically ALT) every 2 years • Consider ultrasound of liver if liver enzymes are abnormal • Fasting lipid profile every 2 years • Fasting plasma glucose, HbA1C every 2 years, if severe obesity (consider 2 h OGTT (1.75 mg/kg upto max 75 g) • Sleep study if symptoms present Management • Structured behavior programs should not be offered to children/youth who are at a healthy weight to prevent obesity • The subject of talking about
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Growth
e abnormal • Fasting lipid profile every 2 years • Fasting plasma glucose, HbA1C every 2 years, if severe obesity (consider 2 h OGTT (1.75 mg/kg upto max 75 g) • Sleep study if symptoms present Management • <span>Structured behavior programs should not be offered to children/youth who are at a healthy weight to prevent obesity • The subject of talking about a patient’s weight can often be a very sensitive topic. o Ask for permission to discuss weight o Assess obesity related risk and poten
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Growth
; Management • Structured behavior programs should not be offered to children/youth who are at a healthy weight to prevent obesity • The subject of talking about a patient’s weight can often be a very sensitive topic. <span>o Ask for permission to discuss weight o Assess obesity related risk and potential ‘root causes’of weight gain o Advice on obesity risks, discuss treatment benefits and options o Agree on a realistic SMART plan to achieve health behavior outcomes o Assist in addressing drivers and barriers, offer education and resources, refer as necessary and arrange follow‐up • Stress the importance of achieving behavioural and health‐related improvements rather than focusing primarily on numbers on a scale. • Behaviour modification – can prod
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Growth
eatment benefits and options o Agree on a realistic SMART plan to achieve health behavior outcomes o Assist in addressing drivers and barriers, offer education and resources, refer as necessary and arrange follow‐up • <span>Stress the importance of achieving behavioural and health‐related improvements rather than focusing primarily on numbers on a scale. • Behaviour modification – can produce weight loss of 5‐20% over 3‐6 months • Lifestyle modification strategies can be broadly categorized as: o Controlling the envi
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Growth
and barriers, offer education and resources, refer as necessary and arrange follow‐up • Stress the importance of achieving behavioural and health‐related improvements rather than focusing primarily on numbers on a scale. • <span>Behaviour modification – can produce weight loss of 5‐20% over 3‐6 months • Lifestyle modification strategies can be broadly categorized as: o Controlling the environment – include the entire family in healthy changes rather than child alone
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Growth
w‐up • Stress the importance of achieving behavioural and health‐related improvements rather than focusing primarily on numbers on a scale. • Behaviour modification – can produce weight loss of 5‐20% over 3‐6 months • <span>Lifestyle modification strategies can be broadly categorized as: o Controlling the environment – include the entire family in healthy changes rather than child alone o Monitoring behavior o Assessing motivation o Setting realistic goals o Rewarding successful changes in behavior o Arrange short‐term follow‐up to review progress • Involve a multidisciplinary team (dietitian, exercise therapist, social worker, psychologist) • There is no role of medications (such as orlistat) for healthy weight
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Growth
in healthy changes rather than child alone o Monitoring behavior o Assessing motivation o Setting realistic goals o Rewarding successful changes in behavior o Arrange short‐term follow‐up to review progress <span>• Involve a multidisciplinary team (dietitian, exercise therapist, social worker, psychologist) • There is no role of medications (such as orlistat) for healthy weight management in children 2‐11 years old or for routine use in youth 12‐ 17 • Surgical management can be offered in a select group of adolescents – there is no role for routine referral for surgical management for overweight/obesity Healthy Active Living Syllabus: Lipnowski et al. Healthy Active Living: Physical activity guidelines for children and adolescents . Paediatr Child Health. 2012;17(4
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Growth
r overweight/obesity Healthy Active Living Syllabus: Lipnowski et al. Healthy Active Living: Physical activity guidelines for children and adolescents . Paediatr Child Health. 2012;17(4):209. Introduction • <span>‘Healthy living’ is described by Health Canada as making choices that enhance physical, mental, social and spiritual health • Health care professionals should be promoting physical activity and reducing sedentary time in children and adolescents Canadian guidelines for physical activity
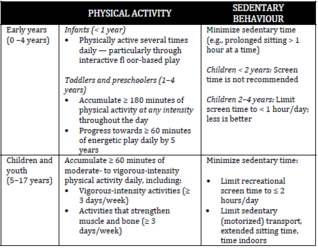
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Growth
by Health Canada as making choices that enhance physical, mental, social and spiritual health • Health care professionals should be promoting physical activity and reducing sedentary time in children and adolescents <span>Canadian guidelines for physical activity and sedentary behavior Short stature: differential ABCDEFG : A lone (neglected infant) B one dysplasias (rickets, scoliosis, mucopolysaccharidoses) C hromosomal (Turner's
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Growth
spiritual health • Health care professionals should be promoting physical activity and reducing sedentary time in children and adolescents Canadian guidelines for physical activity and sedentary behavior <span>Short stature: differential ABCDEFG : A lone (neglected infant) B one dysplasias (rickets, scoliosis, mucopolysaccharidoses) C hromosomal (Turner's, Down's) D elayed growth E ndocrine (low growth hormone, Cushing's, hypothyroid) F amilial G I malabsorption (celiac, Crohn's) <span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
Abstract Although immunization has decreased the incidence of bacterial pneumonia in vaccinated children, pneumonia remains common in healthy children. Symptoms of bacterial pneumonia frequently overlap those present with viral infections or reactive airway disease. Optimally, the diagnosis of bacterial pneumonia should be supported by a chest radiograph before starting antimicrobials. Factors such as age, vital signs and other measures of illness
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
zation has decreased the incidence of bacterial pneumonia in vaccinated children, pneumonia remains common in healthy children. Symptoms of bacterial pneumonia frequently overlap those present with viral infections or reactive airway disease. <span>Optimally, the diagnosis of bacterial pneumonia should be supported by a chest radiograph before starting antimicrobials. Factors such as age, vital signs and other measures of illness severity are critical when deciding whether to admit a patient to hospital. Because Streptococcus pneumoniae continues to
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
f bacterial pneumonia should be supported by a chest radiograph before starting antimicrobials. Factors such as age, vital signs and other measures of illness severity are critical when deciding whether to admit a patient to hospital. Because <span>Streptococcus pneumoniae continues to be the most common cause of bacterial pneumonia in children, prescribing amoxicillin or ampicillin for seven to 10 days remains the mainstay of empirical therapy for nonsevere pneumonia .If improvement does not occur, consideration should be giv
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
gnosis of bacterial pneumonia should be supported by a chest radiograph before starting antimicrobials. Factors such as age, vital signs and other measures of illness severity are critical when deciding whether to admit a patient to hospital. <span>Because Streptococcus pneumoniae continues to be the most common cause of bacterial pneumonia in children, prescribing amoxicillin or ampicillin for seven to 10 days remains the mainstay of empirical therapy for nonsevere pneumonia .If improvement does not occur, consideration should be given to searching for complications (empyema or lung abscess). Routine chest radiographs at the end of therapy are not recommend
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
hospital. Because Streptococcus pneumoniae continues to be the most common cause of bacterial pneumonia in children, prescribing amoxicillin or ampicillin for seven to 10 days remains the mainstay of empirical therapy for nonsevere pneumonia .<span>If improvement does not occur, consideration should be given to searching for complications (empyema or lung abscess). Routine chest radiographs at the end of therapy are not recommended unless clinically indicated. Key Words: Antimicrobial therapy; Bacterial pneumonia; Viral pneumonia &#
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
escribing amoxicillin or ampicillin for seven to 10 days remains the mainstay of empirical therapy for nonsevere pneumonia .If improvement does not occur, consideration should be given to searching for complications (empyema or lung abscess). <span>Routine chest radiographs at the end of therapy are not recommended unless clinically indicated. Key Words: Antimicrobial therapy; Bacterial pneumonia; Viral pneumonia Most physicians who care for children and youth have had experience with managing acute
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
y, because these pneumonias may be caused by different pathogens or require more extensive investigation. The present practice point replaces a previous document published in 2011.[4] Definition and host risk factors <span>Pneumonia is an acute inflammation of the parenchyma of the lower respiratory tract caused by a microbial pathogen. Bacterial infections are usually primary but, occasionally, viral respiratory tract infections such as influenza are followed by bacterial pneumonias.[5] Uncomplicated pneumonias may be accompanied by small parapneumonic effusions. Evidence of empyema (pus in the pleural space), a lung abscess or a necrotic portion of lung parenchyma implies the development of a complicated pneumonia. Etiology The most common causes of pneumonia in infants and preschool children are viruses that usually, but not exclusively, circulate in winter (eg, respirat
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
ay be accompanied by small parapneumonic effusions. Evidence of empyema (pus in the pleural space), a lung abscess or a necrotic portion of lung parenchyma implies the development of a complicated pneumonia. Etiology <span>The most common causes of pneumonia in infants and preschool children are viruses that usually, but not exclusively, circulate in winter (eg, respiratory syncytial virus, influenza, parainfluenza virus and human metapneumovirus). Viruses as a sole cause of pneumonia are less common in older children, with the exception of influenza. Among bacteria, Streptococcus pneumoniae continues to be the most common bacterial pathogen causing pneumonia in children of all ages. Group A streptococcal pneumonia is mu
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
xclusively, circulate in winter (eg, respiratory syncytial virus, influenza, parainfluenza virus and human metapneumovirus). Viruses as a sole cause of pneumonia are less common in older children, with the exception of influenza. <span>Among bacteria, Streptococcus pneumoniae continues to be the most common bacterial pathogen causing pneumonia in children of all ages. Group A streptococcal pneumonia is much less common. Although Staphylococcus aureus is not a common cause of paediatric pneumonia, it has been increasingly encountered in communities where methicillin-resistant S aureus (MRSA) is prevalent. Haemophilus influenzae type b has almost disappeared because of vaccination. Mycoplasma pneumoniae and Chlamydophila pneumoniae are more common causes of pneumonia among school-age children, but they occasionally cause pneumonia in younger children.[6] Symptoms and signs of acute pneumonia The symptoms of pneumonia may be nonspecific, especially in infants and younger children. Acute onset of fever, cough
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
n. Mycoplasma pneumoniae and Chlamydophila pneumoniae are more common causes of pneumonia among school-age children, but they occasionally cause pneumonia in younger children.[6] Symptoms and signs of acute pneumonia <span>The symptoms of pneumonia may be nonspecific, especially in infants and younger children. Acute onset of fever, cough, difficulty breathing, poor feeding or vomiting, and lack of interest in normal activities are common symptoms. Chest or abdominal pain may also be prominent
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
among school-age children, but they occasionally cause pneumonia in younger children.[6] Symptoms and signs of acute pneumonia The symptoms of pneumonia may be nonspecific, especially in infants and younger children. <span>Acute onset of fever, cough, difficulty breathing, poor feeding or vomiting, and lack of interest in normal activities are common symptoms. Chest or abdominal pain may also be prominent features. Abrupt onset of rigors favours a bacterial cause. M pneumoniae is typically characterized by malaise and headache for seven to 1
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
The symptoms of pneumonia may be nonspecific, especially in infants and younger children. Acute onset of fever, cough, difficulty breathing, poor feeding or vomiting, and lack of interest in normal activities are common symptoms. <span>Chest or abdominal pain may also be prominent features. Abrupt onset of rigors favours a bacterial cause. M pneumoniae is typically characterized by malaise and headache for seven to 10 days before the onset of fever and cough, which then pr
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
c, especially in infants and younger children. Acute onset of fever, cough, difficulty breathing, poor feeding or vomiting, and lack of interest in normal activities are common symptoms. Chest or abdominal pain may also be prominent features. <span>Abrupt onset of rigors favours a bacterial cause. M pneumoniae is typically characterized by malaise and headache for seven to 10 days before the onset of fever and cough, which then predominate. During annual influenza season, influe
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
te onset of fever, cough, difficulty breathing, poor feeding or vomiting, and lack of interest in normal activities are common symptoms. Chest or abdominal pain may also be prominent features. Abrupt onset of rigors favours a bacterial cause. <span>M pneumoniae is typically characterized by malaise and headache for seven to 10 days before the onset of fever and cough, which then predominate. During annual influenza season, influenza (with or without a secondary bacterial infection) as a cause of pneumonia should be strongly considered. Influenza infections may be heralded
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
abdominal pain may also be prominent features. Abrupt onset of rigors favours a bacterial cause. M pneumoniae is typically characterized by malaise and headache for seven to 10 days before the onset of fever and cough, which then predominate. <span>During annual influenza season, influenza (with or without a secondary bacterial infection) as a cause of pneumonia should be strongly considered. Influenza infections may be heralded by the sudden onset of systemic symptoms such as diffuse myalgias and fever, which are then followed by cough, sore throat or other respiratory symptoms. Children typically experience fever and tachypnea (determined by counting the respiratory rate for 60 s in a calm state) (Table 1). Indrawing, retractions and/or a trachea
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
y symptoms. Children typically experience fever and tachypnea (determined by counting the respiratory rate for 60 s in a calm state) (Table 1). Indrawing, retractions and/or a tracheal tug indicate respiratory distress (dyspnea). <span>Measurement of oxygen saturation with pulse oximetry is indicated in all patients presenting to a hospital or with significant illness because hypoxemia may not be clinically apparent and cyanosis is only associated with severe hypoxemia. However, a normal oxygen saturation does not exclude the possibility of pneumonia. Physical signs suggesting pneumonic consolidation include dullness to percussion, increased tactile fremitus, reduced normal vesicular breath sounds and increased bronchial
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
cal signs suggesting pneumonic consolidation include dullness to percussion, increased tactile fremitus, reduced normal vesicular breath sounds and increased bronchial breath sounds – all of which may be difficult to detect in young children. <span>The predominance of wheezing and hypoxia should suggest the possibility of bronchiolitis or mucous plugging from asthma, rather than pneumonia. Signs of an effusion include dullness to percussion, decreased tactile fremitus, and decreased or absent breath sounds. There may be associated signs of dehydration and/or sepsis. 
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
gging from asthma, rather than pneumonia. Signs of an effusion include dullness to percussion, decreased tactile fremitus, and decreased or absent breath sounds. There may be associated signs of dehydration and/or sepsis. TABLE 1 <span>Age-specific criteria for tachypnea Age Approximate normal respiratory rates Upper limit that should be used to define tachypnea <2 months 34–50 60 2–12 months 25–40 50 1–5 years 20–30 40 >5 years 15–25 30 Data presented as breaths/min Investigations Imaging Radiographs are not indicated for children experiencing wheezing with a typical presentation
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
spiratory rates Upper limit that should be used to define tachypnea <2 months 34–50 60 2–12 months 25–40 50 1–5 years 20–30 40 >5 years 15–25 30 Data presented as breaths/min Investigations Imaging <span>Radiographs are not indicated for children experiencing wheezing with a typical presentation of bronchiolitis or asthma because bacterial pneumonia is very unlikely. When bacterial pneumonia is suspected clinically (a febrile child with acute respiratory symptoms and physical findings compatible with consolidation or pleural effusion), a chest radio
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
as breaths/min Investigations Imaging Radiographs are not indicated for children experiencing wheezing with a typical presentation of bronchiolitis or asthma because bacterial pneumonia is very unlikely. <span>When bacterial pneumonia is suspected clinically (a febrile child with acute respiratory symptoms and physical findings compatible with consolidation or pleural effusion), a chest radiograph (both postero-anterior and lateral) should usually be obtained. The reason for imaging is that the clinical features of other conditions overlap with bacterial pneumonia, and antibiotics may be avoided if the chest radiograph does not s
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
ally be obtained. The reason for imaging is that the clinical features of other conditions overlap with bacterial pneumonia, and antibiotics may be avoided if the chest radiograph does not suggest bacterial pneumonia.[7] However, <span>in cases where the diagnosis of bacterial pneumonia is highly suspected from history, combined with typical clinical and physical findings and the child is not sufficiently ill to require hospitalization, a chest radiograph is not essential. All hospitalized children should have a chest radiograph performed to assess the extent of pneumonia and determine the presence of pleural effusion or abscess. The promine
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
in cases where the diagnosis of bacterial pneumonia is highly suspected from history, combined with typical clinical and physical findings and the child is not sufficiently ill to require hospitalization, a chest radiograph is not essential. <span>All hospitalized children should have a chest radiograph performed to assess the extent of pneumonia and determine the presence of pleural effusion or abscess. The prominent radiographic pattern in bacterial pneumonia is alveolar/airspace disease that is seen as consolidations. Classically, these present as lobar consolidations wi
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
ill to require hospitalization, a chest radiograph is not essential. All hospitalized children should have a chest radiograph performed to assess the extent of pneumonia and determine the presence of pleural effusion or abscess. <span>The prominent radiographic pattern in bacterial pneumonia is alveolar/airspace disease that is seen as consolidations. Classically, these present as lobar consolidations with air bronchograms; however, airspace disease may also take the form of subsegmental or nodular opacities (eg, round pneumonia) or infiltrates. Clinical correlation is always important, especially when considering other, rarer causes of similar radiographic patterns. Poorly defined patches of infiltrates or atelectasis are more indicative of a viral etiology.[8] The ‘atypical’ pathogens, M pneumoniae or C pneumoniae, classically produce
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
disease may also take the form of subsegmental or nodular opacities (eg, round pneumonia) or infiltrates. Clinical correlation is always important, especially when considering other, rarer causes of similar radiographic patterns. <span>Poorly defined patches of infiltrates or atelectasis are more indicative of a viral etiology.[8] The ‘atypical’ pathogens, M pneumoniae or C pneumoniae, classically produce bilateral focal or interstitial infiltrates that appear to be more extensive relative to the milder but p
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
a is difficult in children. Most cases are not bacteremic at the time of diagnosis. If sputum is available (usually only in children >10 years of age), it should be sent for Gram staining and, if considered adequate, cultured. <span>Viral testing of nasopharyngeal secretions is usually not indicated for outpatients with suspected pneumonia. However, such testing should be strongly considered in children admitted during influenza season with possible viral pneumonia because antivirals are likely to be of benefit for influenza pneumonia, particularly in moderately to severely ill children.[11][12] Children (usually school age) with subacute, nonsevere pneumonia, presenting with features such as prominent cough, minimal leukocytosis and a nonlobar infiltrate, may have pne
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
a positive result may indicate remote infection. Bloodwork Typical bacterial pneumonias usually present with higher peripheral white blood cell counts than ‘atypical’ bacterial or viral pneumonias (eg, M pneumoniae). <span>A complete blood count with differential testing and blood cultures (before starting antimicrobial therapy, if possible) are indicated for children who are hospitalized. Even though the yield from blood cultures is low, a positive result is helpful, especially if the child subsequently experiences a complicated course. Furthermore, it is an important p
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
inimum volume of blood cultured should be at least 1 mL to 2 mL in infants, 4 mL to 5 mL in children <10 years of age and 10 mL to 20 mL in older children. Guidelines for referral to hospital or hospital admission <span>Most children with pneumonia can be managed as outpatients. Specific paediatric criteria for admission are not available. Hospitalization is generally indicated if a child has inadequate oral intake, is intolerant of oral therapy, has severe il
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
nd 10 mL to 20 mL in older children. Guidelines for referral to hospital or hospital admission Most children with pneumonia can be managed as outpatients. Specific paediatric criteria for admission are not available. <span>Hospitalization is generally indicated if a child has inadequate oral intake, is intolerant of oral therapy, has severe illness or respiratory compromise (eg, grunting, nasal flaring, apnea, hypoxemia), or if the pneumonia is complicated. There should be a lower threshold for admitting infants younger than six months of age to hospital because they may need more supportive care and monitoring, and it can be difficult to
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
r threshold for admitting infants younger than six months of age to hospital because they may need more supportive care and monitoring, and it can be difficult to recognize subtle deterioration clinically. Management <span>If influenza is detected or suspected, strong consideration should be given to prompt treatment with neuraminidase inhibitors (oseltamivir, zanamivir). Treatment with antivirals has been shown to provide benefit and may prevent secondary bacterial infections, particularly in hospitalized or moderately to severely ill children.[12]-[14] When other viruses are detected in a nasopharyngeal sample and/or the chest radiograph is most compatible with viral pneumonia (ie, without consolidations), manage with support
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
with neuraminidase inhibitors (oseltamivir, zanamivir). Treatment with antivirals has been shown to provide benefit and may prevent secondary bacterial infections, particularly in hospitalized or moderately to severely ill children.[12]-[14] <span>When other viruses are detected in a nasopharyngeal sample and/or the chest radiograph is most compatible with viral pneumonia (ie, without consolidations), manage with supportive care (ie, oxygen and rehydration if required) without antibiotics, unless there is convincing evidence of a secondary bacterial pneumonia. The primary goal of antimicrobial therapy, for the vast majority of uncomplicated community-acquired pneumonias, is to provide good coverage for S pneumoniae, because mole
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
most compatible with viral pneumonia (ie, without consolidations), manage with supportive care (ie, oxygen and rehydration if required) without antibiotics, unless there is convincing evidence of a secondary bacterial pneumonia. <span>The primary goal of antimicrobial therapy, for the vast majority of uncomplicated community-acquired pneumonias, is to provide good coverage for S pneumoniae, because molecular-based techniques have shown this to be the predominant bacterial pathogen.[15]-[17] Therefore, outpatients with lobar or broncho-pneumonia should usually be treated with oral amoxicillin. Patients who require hospitalization but do not have a life-threatening
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
f antimicrobial therapy, for the vast majority of uncomplicated community-acquired pneumonias, is to provide good coverage for S pneumoniae, because molecular-based techniques have shown this to be the predominant bacterial pathogen.[15]-[17] <span>Therefore, outpatients with lobar or broncho-pneumonia should usually be treated with oral amoxicillin. Patients who require hospitalization but do not have a life-threatening illness should usually be started empirically on intravenous ampicillin. There is recent data demonstrating that
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
vide good coverage for S pneumoniae, because molecular-based techniques have shown this to be the predominant bacterial pathogen.[15]-[17] Therefore, outpatients with lobar or broncho-pneumonia should usually be treated with oral amoxicillin. <span>Patients who require hospitalization but do not have a life-threatening illness should usually be started empirically on intravenous ampicillin. There is recent data demonstrating that ampicillin alone leads to a good clinical outcome in almost all cases of community-acquired pneumonia, including cases that require hospitalization.[18]-[20] Children who experience respiratory failure or septic shock associated with pneumonia should receive empiric therapy with a third-generation cephalosporin because
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
ally on intravenous ampicillin. There is recent data demonstrating that ampicillin alone leads to a good clinical outcome in almost all cases of community-acquired pneumonia, including cases that require hospitalization.[18]-[20] <span>Children who experience respiratory failure or septic shock associated with pneumonia should receive empiric therapy with a third-generation cephalosporin because it offers broader coverage. Ceftriaxone or cefotaxime offer better coverage than amoxicillin or ampicillin for beta-lactamase-producing H influenzae and may be more efficacious against high-level penicillin-resistant pneumococcus – and possibly provide empirical coverage for the rare methicillin-susceptible S aureus (a rare cause of pneumonia).[21] However, when there is rapidly progressing multilobar disease or pneumatoceles, the addition of vancomycin is suggested empirically to provide extra coverage for MRSA until culture
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
or beta-lactamase-producing H influenzae and may be more efficacious against high-level penicillin-resistant pneumococcus – and possibly provide empirical coverage for the rare methicillin-susceptible S aureus (a rare cause of pneumonia).[21] <span>However, when there is rapidly progressing multilobar disease or pneumatoceles, the addition of vancomycin is suggested empirically to provide extra coverage for MRSA until culture results are available. If results of microbiological investigations in these patients do not reveal a pathogen, transitioning to ampicillin with subsequent oral amoxicillin is reasonable. The antimicrobial management of patients with suspected empyema is similar to that of patients without empyema because there is a predominance of S pneumoniae being the et
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Uncomplicated Pneumonia
or penicillin is recommended, followed by oral therapy with amoxicillin. If another pathogen is detected in pleural fluid or blood, modifications to the antimicrobial regimen should be made based on antimicrobial susceptibility. T<span>he role of antimicrobials in treating both M pneumoniae and C pneumoniae is unknown because most children resolve infection without macrolides. However, treatment may be appropriate to hasten recovery in chil
Article 1476203515148
APPENDIX 23: A DEBIT/CREDIT ACCOUNTING SYSTEM
#cfa-level-1 #reading-23-financial-reporting-mechanics
The main section of this reading presented a basic accounting system represented as a spreadsheet. An alternative system that underlies most manual and electronic accounting systems uses debits and credits. Both a spreadsheet and a debit/credit system are based on the basic accounting equation: Assets = Liabilities + Owners’ equity Early generations of accountants desired a system for recording transactions that maintained the balance of the accounting equation and avoided the use of negative numbers (which could lead to errors in recording). The system can be illustrated with T-accounts for every account involved in recording transactions. The T-account is so named for its shape: T-Account Debit Credit The left-hand side of the T-account is called a “debit,” and the right-hand side is termed a “credit.” The names should not be construed as denoting value. A debit is not better than a credit and vice versa. Debit simply means the left side of the T-account, and credit simply means t
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
APPENDIX 23: A DEBIT/CREDIT ACCOUNTING SYSTEM
The main section of this reading presented a basic accounting system represented as a spreadsheet. An alternative system that underlies most manual and electronic accounting systems uses debits and credits. Both a spreadsheet and a debit/credit system are based on the basic accounting equation: Assets = Liabilities + Owners’ equity Early generations of accountants
Flashcard 1476205874444
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itAn alternative system that underlies most manual and electronic accounting systems uses debits and credits.
Original toplevel document
APPENDIX 23: A DEBIT/CREDIT ACCOUNTING SYSTEMThe main section of this reading presented a basic accounting system represented as a spreadsheet. An alternative system that underlies most manual and electronic accounting systems uses debits and credits. Both a spreadsheet and a debit/credit system are based on the basic accounting equation: Assets = Liabilities + Owners’ equity Early generations of accountants
Flashcard 1476207447308
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
APPENDIX 23: A DEBIT/CREDIT ACCOUNTING SYSTEM
ad> The main section of this reading presented a basic accounting system represented as a spreadsheet. An alternative system that underlies most manual and electronic accounting systems uses debits and credits. Both a spreadsheet and a debit/credit system are based on the basic accounting equation: Assets = Liabilities + Owners’ equity Early generations of accountants desired a system for recording transactions that maintained the balance of the accounting equation and avoided the use of negative numbers
ad> The main section of this reading presented a basic accounting system represented as a spreadsheet. An alternative system that underlies most manual and electronic accounting systems uses debits and credits. Both a spreadsheet and a debit/credit system are based on the basic accounting equation: Assets = Liabilities + Owners’ equity Early generations of accountants desired a system for recording transactions that maintained the balance of the accounting equation and avoided the use of negative numbers
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
APPENDIX 23: A DEBIT/CREDIT ACCOUNTING SYSTEM
tem that underlies most manual and electronic accounting systems uses debits and credits. Both a spreadsheet and a debit/credit system are based on the basic accounting equation: Assets = Liabilities + Owners’ equity <span>Early generations of accountants desired a system for recording transactions that maintained the balance of the accounting equation and avoided the use of negative numbers (which could lead to errors in recording). The system can be illustrated with T-accounts for every account involved in recording transactions. The T-account is so named for its shape: T-Account Debit Credit &#
Flashcard 1476210855180
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itEarly generations of accountants desired a system for recording transactions that maintained the balance of the accounting equation and avoided the use of negative numbers (which could lead to errors in recording).
Original toplevel document
APPENDIX 23: A DEBIT/CREDIT ACCOUNTING SYSTEMtem that underlies most manual and electronic accounting systems uses debits and credits. Both a spreadsheet and a debit/credit system are based on the basic accounting equation: Assets = Liabilities + Owners’ equity <span>Early generations of accountants desired a system for recording transactions that maintained the balance of the accounting equation and avoided the use of negative numbers (which could lead to errors in recording). The system can be illustrated with T-accounts for every account involved in recording transactions. The T-account is so named for its shape: T-Account Debit Credit &#
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
APPENDIX 23: A DEBIT/CREDIT ACCOUNTING SYSTEM
e numbers (which could lead to errors in recording). The system can be illustrated with T-accounts for every account involved in recording transactions. The T-account is so named for its shape: T-Account Debit Credit <span>The left-hand side of the T-account is called a “debit,” and the right-hand side is termed a “credit.” The names should not be construed as denoting value. A debit is not better than a credit and vice versa. Debit simply means the left side of the T-account, and credit simply means the r
Flashcard 1476213476620
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itThe left-hand side of the T-account is called a “debit,” and the right-hand side is termed a “credit.”
Original toplevel document
APPENDIX 23: A DEBIT/CREDIT ACCOUNTING SYSTEMe numbers (which could lead to errors in recording). The system can be illustrated with T-accounts for every account involved in recording transactions. The T-account is so named for its shape: T-Account Debit Credit <span>The left-hand side of the T-account is called a “debit,” and the right-hand side is termed a “credit.” The names should not be construed as denoting value. A debit is not better than a credit and vice versa. Debit simply means the left side of the T-account, and credit simply means the r
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
APPENDIX 23: A DEBIT/CREDIT ACCOUNTING SYSTEM
T-account is so named for its shape: T-Account Debit Credit The left-hand side of the T-account is called a “debit,” and the right-hand side is termed a “credit.” The names should not be construed as denoting value. <span>A debit is not better than a credit and vice versa. Debit simply means the left side of the T-account, and credit simply means the right side. Traditionally, debit is abbreviated as “DR,” whereas credit is abbreviated “CR.” The T-account is also related to the balance sheet and accounting equation as follows: Bala
Flashcard 1476217408780
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
APPENDIX 23: A DEBIT/CREDIT ACCOUNTING SYSTEM
T-account is so named for its shape: T-Account Debit Credit The left-hand side of the T-account is called a “debit,” and the right-hand side is termed a “credit.” The names should not be construed as denoting value. <span>A debit is not better than a credit and vice versa. Debit simply means the left side of the T-account, and credit simply means the right side. Traditionally, debit is abbreviated as “DR,” whereas credit is abbreviated “CR.” The T-account is also related to the balance sheet and accounting equation as follows: Bal
T-account is so named for its shape: T-Account Debit Credit The left-hand side of the T-account is called a “debit,” and the right-hand side is termed a “credit.” The names should not be construed as denoting value. <span>A debit is not better than a credit and vice versa. Debit simply means the left side of the T-account, and credit simply means the right side. Traditionally, debit is abbreviated as “DR,” whereas credit is abbreviated “CR.” The T-account is also related to the balance sheet and accounting equation as follows: Bal
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
APPENDIX 23: A DEBIT/CREDIT ACCOUNTING SYSTEM
raditionally, debit is abbreviated as “DR,” whereas credit is abbreviated “CR.” The T-account is also related to the balance sheet and accounting equation as follows: Balance Sheet Assets Liabilities Owners’ Equity <span>Assets are referred to as the left side of the balance sheet (and accounting equation) and hence are on the left side of the T-account. Assets are, therefore, recorded with a debit balance. In other words, to record an increase in an asset, an entry is made to the left-hand side of a T-account. A decrease to an asset is recorded on the right side of a T-account. Liabiliti
Flashcard 1476221603084
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itAssets are referred to as the left side of the T-account. Assets are, therefore, recorded with a debit balance
Original toplevel document
APPENDIX 23: A DEBIT/CREDIT ACCOUNTING SYSTEMraditionally, debit is abbreviated as “DR,” whereas credit is abbreviated “CR.” The T-account is also related to the balance sheet and accounting equation as follows: Balance Sheet Assets Liabilities Owners’ Equity <span>Assets are referred to as the left side of the balance sheet (and accounting equation) and hence are on the left side of the T-account. Assets are, therefore, recorded with a debit balance. In other words, to record an increase in an asset, an entry is made to the left-hand side of a T-account. A decrease to an asset is recorded on the right side of a T-account. Liabiliti
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
APPENDIX 23: A DEBIT/CREDIT ACCOUNTING SYSTEM
lities Owners’ Equity Assets are referred to as the left side of the balance sheet (and accounting equation) and hence are on the left side of the T-account. Assets are, therefore, recorded with a debit balance. In other words, <span>to record an increase in an asset, an entry is made to the left-hand side of a T-account. A decrease to an asset is recorded on the right side of a T-account. Liabilities and owners’ equity are referred to as the right side of the balance sheet (and accounting equation). Inc
Flashcard 1476224224524
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itto record an increase in an asset, an entry is made to the left-hand side of a T-account.
Original toplevel document
APPENDIX 23: A DEBIT/CREDIT ACCOUNTING SYSTEMlities Owners’ Equity Assets are referred to as the left side of the balance sheet (and accounting equation) and hence are on the left side of the T-account. Assets are, therefore, recorded with a debit balance. In other words, <span>to record an increase in an asset, an entry is made to the left-hand side of a T-account. A decrease to an asset is recorded on the right side of a T-account. Liabilities and owners’ equity are referred to as the right side of the balance sheet (and accounting equation). Inc
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
APPENDIX 23: A DEBIT/CREDIT ACCOUNTING SYSTEM
e sheet (and accounting equation) and hence are on the left side of the T-account. Assets are, therefore, recorded with a debit balance. In other words, to record an increase in an asset, an entry is made to the left-hand side of a T-account. <span>A decrease to an asset is recorded on the right side of a T-account. Liabilities and owners’ equity are referred to as the right side of the balance sheet (and accounting equation). Increases to liabilities and owners’ equity are recorded on the right si
Flashcard 1476226845964
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itA decrease to an asset is recorded on the right side of a T-account.
Original toplevel document
APPENDIX 23: A DEBIT/CREDIT ACCOUNTING SYSTEMe sheet (and accounting equation) and hence are on the left side of the T-account. Assets are, therefore, recorded with a debit balance. In other words, to record an increase in an asset, an entry is made to the left-hand side of a T-account. <span>A decrease to an asset is recorded on the right side of a T-account. Liabilities and owners’ equity are referred to as the right side of the balance sheet (and accounting equation). Increases to liabilities and owners’ equity are recorded on the right si
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
APPENDIX 23: A DEBIT/CREDIT ACCOUNTING SYSTEM
he T-account. Assets are, therefore, recorded with a debit balance. In other words, to record an increase in an asset, an entry is made to the left-hand side of a T-account. A decrease to an asset is recorded on the right side of a T-account. <span>Liabilities and owners’ equity are referred to as the right side of the balance sheet (and accounting equation). Increases to liabilities and owners’ equity are recorded on the right side of a T-account; decreases to liabilities and owners’ equity are recorded on the left side. At an
Flashcard 1476231040268
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itLiabilities and owners’ equity are referred to as the right side of the balance sheet (and accounting equation)
Original toplevel document
APPENDIX 23: A DEBIT/CREDIT ACCOUNTING SYSTEMhe T-account. Assets are, therefore, recorded with a debit balance. In other words, to record an increase in an asset, an entry is made to the left-hand side of a T-account. A decrease to an asset is recorded on the right side of a T-account. <span>Liabilities and owners’ equity are referred to as the right side of the balance sheet (and accounting equation). Increases to liabilities and owners’ equity are recorded on the right side of a T-account; decreases to liabilities and owners’ equity are recorded on the left side. At an
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
APPENDIX 23: A DEBIT/CREDIT ACCOUNTING SYSTEM
sset, an entry is made to the left-hand side of a T-account. A decrease to an asset is recorded on the right side of a T-account. Liabilities and owners’ equity are referred to as the right side of the balance sheet (and accounting equation). <span>Increases to liabilities and owners’ equity are recorded on the right side of a T-account; decreases to liabilities and owners’ equity are recorded on the left side. At any point in time, the balance in an account is determined by summing all the amounts on the left side of the account, summing all the amounts on the right side of the a
Flashcard 1476233661708
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itIncreases to liabilities and owners’ equity are recorded on the right side of a T-account; decreases to liabilities and owners’ equity are recorded on the left side.
Original toplevel document
APPENDIX 23: A DEBIT/CREDIT ACCOUNTING SYSTEMsset, an entry is made to the left-hand side of a T-account. A decrease to an asset is recorded on the right side of a T-account. Liabilities and owners’ equity are referred to as the right side of the balance sheet (and accounting equation). <span>Increases to liabilities and owners’ equity are recorded on the right side of a T-account; decreases to liabilities and owners’ equity are recorded on the left side. At any point in time, the balance in an account is determined by summing all the amounts on the left side of the account, summing all the amounts on the right side of the a
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
APPENDIX 23: A DEBIT/CREDIT ACCOUNTING SYSTEM
the right side of the balance sheet (and accounting equation). Increases to liabilities and owners’ equity are recorded on the right side of a T-account; decreases to liabilities and owners’ equity are recorded on the left side. <span>At any point in time, the balance in an account is determined by summing all the amounts on the left side of the account, summing all the amounts on the right side of the account, and calculating the difference. If the sum of amounts on the left side of the account is greater than the sum of amounts on the right side of the account, the account has a debit balance equal to the difference. If the sum of amounts on the right side of the account is greater than the sum of amounts on the left side of the account, the account has a credit balance. A T-account is created for each asset account, liability account, and owners’ equity account. The collection of these T-accounts at the beginning of the year for a fictitio
Flashcard 1476237069580
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itIncreases to liabilities and owners’ equity are recorded on the right side of a T-account; decreases to liabilities and owners’ equity are recorded on the left side.
Original toplevel document
APPENDIX 23: A DEBIT/CREDIT ACCOUNTING SYSTEMsset, an entry is made to the left-hand side of a T-account. A decrease to an asset is recorded on the right side of a T-account. Liabilities and owners’ equity are referred to as the right side of the balance sheet (and accounting equation). <span>Increases to liabilities and owners’ equity are recorded on the right side of a T-account; decreases to liabilities and owners’ equity are recorded on the left side. At any point in time, the balance in an account is determined by summing all the amounts on the left side of the account, summing all the amounts on the right side of the a
Flashcard 1476239428876
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itAt any point in time, the balance in an account is determined by summing all the amounts on the left side of the account, summing all the amounts on the right side of the account, and calculating the difference. If the sum of amounts on the left side of the account is greater than the sum of amounts on the right side of the account, the account has a debit balance equal to the difference. If t
Original toplevel document
APPENDIX 23: A DEBIT/CREDIT ACCOUNTING SYSTEMthe right side of the balance sheet (and accounting equation). Increases to liabilities and owners’ equity are recorded on the right side of a T-account; decreases to liabilities and owners’ equity are recorded on the left side. <span>At any point in time, the balance in an account is determined by summing all the amounts on the left side of the account, summing all the amounts on the right side of the account, and calculating the difference. If the sum of amounts on the left side of the account is greater than the sum of amounts on the right side of the account, the account has a debit balance equal to the difference. If the sum of amounts on the right side of the account is greater than the sum of amounts on the left side of the account, the account has a credit balance. A T-account is created for each asset account, liability account, and owners’ equity account. The collection of these T-accounts at the beginning of the year for a fictitio
Flashcard 1476241788172
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open ithe account, summing all the amounts on the right side of the account, and calculating the difference. If the sum of amounts on the left side of the account is greater than the sum of amounts on the right side of the account, the account has a <span>debit balance equal to the difference. If the sum of amounts on the right side of the account is greater than the sum of amounts on the left side of the account, the account has a credit balance. <span><
Original toplevel document
APPENDIX 23: A DEBIT/CREDIT ACCOUNTING SYSTEMthe right side of the balance sheet (and accounting equation). Increases to liabilities and owners’ equity are recorded on the right side of a T-account; decreases to liabilities and owners’ equity are recorded on the left side. <span>At any point in time, the balance in an account is determined by summing all the amounts on the left side of the account, summing all the amounts on the right side of the account, and calculating the difference. If the sum of amounts on the left side of the account is greater than the sum of amounts on the right side of the account, the account has a debit balance equal to the difference. If the sum of amounts on the right side of the account is greater than the sum of amounts on the left side of the account, the account has a credit balance. A T-account is created for each asset account, liability account, and owners’ equity account. The collection of these T-accounts at the beginning of the year for a fictitio
Flashcard 1476244147468
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itof amounts on the right side of the account, the account has a debit balance equal to the difference. If the sum of amounts on the right side of the account is greater than the sum of amounts on the left side of the account, the account has a <span>credit balance. <span><body><html>
Original toplevel document
APPENDIX 23: A DEBIT/CREDIT ACCOUNTING SYSTEMthe right side of the balance sheet (and accounting equation). Increases to liabilities and owners’ equity are recorded on the right side of a T-account; decreases to liabilities and owners’ equity are recorded on the left side. <span>At any point in time, the balance in an account is determined by summing all the amounts on the left side of the account, summing all the amounts on the right side of the account, and calculating the difference. If the sum of amounts on the left side of the account is greater than the sum of amounts on the right side of the account, the account has a debit balance equal to the difference. If the sum of amounts on the right side of the account is greater than the sum of amounts on the left side of the account, the account has a credit balance. A T-account is created for each asset account, liability account, and owners’ equity account. The collection of these T-accounts at the beginning of the year for a fictitio
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
APPENDIX 23: A DEBIT/CREDIT ACCOUNTING SYSTEM
of the account, the account has a debit balance equal to the difference. If the sum of amounts on the right side of the account is greater than the sum of amounts on the left side of the account, the account has a credit balance. <span>A T-account is created for each asset account, liability account, and owners’ equity account. The collection of these T-accounts at the beginning of the year for a fictitious company, Investment Advisers, Ltd. (IAL), is presented in Exhibit 1. Each balance sheet T-account is ter
Flashcard 1476247555340
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Parent (intermediate) annotation
Open itA T-account is created for each asset account, liability account, and owners’ equity account.
Original toplevel document
APPENDIX 23: A DEBIT/CREDIT ACCOUNTING SYSTEMof the account, the account has a debit balance equal to the difference. If the sum of amounts on the right side of the account is greater than the sum of amounts on the left side of the account, the account has a credit balance. <span>A T-account is created for each asset account, liability account, and owners’ equity account. The collection of these T-accounts at the beginning of the year for a fictitious company, Investment Advisers, Ltd. (IAL), is presented in Exhibit 1. Each balance sheet T-account is ter