Edited, memorised or added to reading queue
on 30-Oct-2016 (Sun)
Do you want BuboFlash to help you learning these things? Click here to log in or create user.

| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |


| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Legal Identity of the Bond Issuer and its Legal Form
3.1.1. Legal Identity of the Bond Issuer and its Legal Form The legal obligation to make the contractual payments is assigned to the bond issuer. The issuer is identified in the indenture by its legal name. For a sovereign bond, the legal issuer is usually the office responsible for managing the national budget, such as HM Treasury (Her Majesty’s Treasury) in the United Kingdom. The legal
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Subject 2. Types and characteristics of equity securities
Common Shares Common shares represent ownership shares in a corporation. The two most important characteristics of common shares are: Residual claim means the shareholders are the last in line of all those who have a claim on the assets or income of the corporation. Limited liability means that the greatest amount shareholders can lose in event of failure of the corporation is the original investment. Each share of voting common stock entitles its owner to one vote on any matters of corporate governance that are put to a vote at the corporation's annual meeting. Shareholders who do not attend the annual meeting can vote by proxy, empowering another party to vote in their name. Statutory voting, also known as straight voting, is a procedure of voting for a company's directors in which each shareholders is entitled to one vote per share. For example, if you owne
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Subject 2. Types and characteristics of equity securities
e vote on any matters of corporate governance that are put to a vote at the corporation's annual meeting. Shareholders who do not attend the annual meeting can vote by proxy, empowering another party to vote in their name. <span>Statutory voting, also known as straight voting, is a procedure of voting for a company's directors in which each shareholders is entitled to one vote per share. For example, if you owned 100 shares, you would have 100 votes. Cumulative voting is another procedure of voting for a company's directors. Each shareholder is entitled one vote per share times the number of directors to be elected. For example, if y
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Covenants
3.1.5. Covenants Bond covenants are legally enforceable rules that borrowers and lenders agree on at the time of a new bond issue. An indenture will frequently include affirmative (or positive) and negative covenants. Affirmative covenants enumerate what issuers are required to do, whereas negative covenants specify what issuers are prohibited from doing. <body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Open it
es abound about how poorly these companies managed risk. Such stories are great attention grabbers and a real boon for the media, but they often miss the point that risk management does not guarantee that large losses will not occur. Rather, <span>risk management is the process by which an organization or individual defines the level of risk it wishes to take, measures the level of risk it is taking, and adjusts the latter to equal the former. Risk management never offers a guarantee that large losses will not occur, and it does not eliminate the possibility of total failure. To do so would typically require that the amount of risk taken be so small that the organization would be effectively constrained from pursuing its primary objectives. Risk taking is inh
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Parent (intermediate) annotation
Open itt necessarily when cash is received, and expenses are reported when incurred, not necessarily when paid. The cash flow statement presents another aspect of performance: the ability of a company to generate cash flow from running its business. <span>Ideally, for an established company, the analyst would like to see that the primary source of cash flow is from operating activities as opposed to investing or financing activities.<span><body><html>
Original toplevel document
Open itmethod of reporting cash flows from operating activities discloses major classes of gross cash receipts and gross cash payments. Examples of such classes are cash received from customers and cash paid to suppliers and employees. <span>The indirect method emphasizes the different perspectives of the income statement and cash flow statement. On the income statement, income is reported when earned, not necessarily when cash is received, and expenses are reported when incurred, not necessarily when paid. The cash flow statement presents another aspect of performance: the ability of a company to generate cash flow from running its business. Ideally, for an established company, the analyst would like to see that the primary source of cash flow is from operating activities as opposed to investing or financing activities. The sum of the net cash flows from operating, investing, and financing activities and the effect of exchange rates on cash equals the net change in cash during the fiscal year. For Volks
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |


| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1409984892172
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx of pregnancy: Positive Signs
perienced examiner • Demonstration of a fetus by ultrasound: intrauterine sac visible by 5 weeks amenorrhea, fetal pole at 6 weeks, fetal cardiac activity at 7-8 weeks (transvaginal ultrasound) • Positive pregnancy test: presence of <span>β-hCG; the serum is positive by 9 days post conception; plasma levels double every 48 hours to a maximum at 8-10 weeks gestation when it plateaus (if there are abnormalities in how the β-hCG
Flashcard 1410054622476


| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410110721292
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Ultrasound Tests in Pregnancy
Ultrasound-using Tests in pregnancy: 1. FTS 2. Complete OB scan (aka 18-20wk scan or anatomy scan) 3. growth 4. BPP 5. Doppler flow studies (umbilica a, middle cerebral a, uterine aa) 6. Third trimester s
Flashcard 1410112294156
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Ultrasound Tests in Pregnancy
Ultrasound-using Tests in pregnancy: 1. FTS 2. Complete OB scan (aka 18-20wk scan or anatomy scan) 3. growth 4. BPP 5. Doppler flow studies (umbilica a, middle cerebral a, uterine aa) 6. Third trimester scan
Flashcard 1410113867020
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Ultrasound Tests in Pregnancy
Ultrasound-using Tests in pregnancy: 1. FTS 2. Complete OB scan (aka 18-20wk scan or anatomy scan) 3. growth 4. BPP 5. Doppler flow studies (umbilica a, middle cerebral a, uterine aa) 6. Third trimester scan
Flashcard 1410115439884
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Ultrasound Tests in Pregnancy
Ultrasound-using Tests in pregnancy: 1. FTS 2. Complete OB scan (aka 18-20wk scan or anatomy scan) 3. growth 4. BPP 5. Doppler flow studies (umbilica a, middle cerebral a, uterine aa) 6. Third trimester scan
Flashcard 1410117012748
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Ultrasound Tests in Pregnancy
Ultrasound-using Tests in pregnancy: 1. FTS 2. Complete OB scan (aka 18-20wk scan or anatomy scan) 3. growth 4. BPP 5. Doppler flow studies (umbilica a, middle cerebral a, uterine aa) 6. Third trimester scan
Flashcard 1410118585612
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Ultrasound Tests in Pregnancy
><head>Ultrasound-using Tests in pregnancy: 1. FTS 2. Complete OB scan (aka 18-20wk scan or anatomy scan) 3. growth 4. BPP 5. Doppler flow studies (umbilica a, middle cerebral a, uterine aa) 6. Third trimester scan<html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410121731340
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First trimester scan
FTS: • Useful for: accurately establishing dates, to determine viability, to R/O ectopic pregnancy, to determine number of fetuses and in multiple pregnancy to establish chorionicity • Many people will have this for measurement o
Flashcard 1410123304204
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First trimester scan
FTS: • Useful for: accurately establishing dates, to determine viability, to R/O ectopic pregnancy, to determine number of fetuses and in multiple pregnancy to establish chorionicity • Many people will have this for measurement of the fetal nuchal trans
Flashcard 1410124877068
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First trimester scan
FTS: • Useful for: accurately establishing dates, to determine viability, to R/O ectopic pregnancy, to determine number of fetuses and in multiple pregnancy to establish chorionicity • Many people will have this for measurement of the fetal nuchal translucency (NT) as part of th
Flashcard 1410126449932
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First trimester scan
FTS: • Useful for: accurately establishing dates, to determine viability, to R/O ectopic pregnancy, to determine number of fetuses and in multiple pregnancy to establish chorionicity • Many people will have this for measurement of the fetal nuchal translucency (NT) as part of their prenatal genetic screening a
Flashcard 1410128022796
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First trimester scan
FTS: • Useful for: accurately establishing dates, to determine viability, to R/O ectopic pregnancy, to determine number of fetuses and in multiple pregnancy to establish chorionicity • Many people will have this for measurement of the fetal nuchal translucency (NT) as part of their prenatal genetic screening at 11-14 weeks [First Trimester Screen (FTS), Integra
Flashcard 1410129595660
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First trimester scan
S: • Useful for: accurately establishing dates, to determine viability, to R/O ectopic pregnancy, to determine number of fetuses and in multiple pregnancy to establish chorionicity • Many people will have this for measurement of the <span>fetal nuchal translucency (NT) as part of their prenatal genetic screening at 11-14 weeks [First Trimester Screen (FTS), Integrated Prenatal Screen (IPS)]<span><body><html>
Flashcard 1410131168524
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First trimester scan
o R/O ectopic pregnancy, to determine number of fetuses and in multiple pregnancy to establish chorionicity • Many people will have this for measurement of the fetal nuchal translucency (NT) as part of their prenatal genetic screening at <span>11-14 weeks [First Trimester Screen (FTS), Integrated Prenatal Screen (IPS)]<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410134838540
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
The complete OB scan, aka 18-20 wk scan/anatomy scan
The Complete Obstetrical Scan (AKA Anatomy Scan) • Should be offered to all pregnant women as a screen for placental, fetal, and pregnancy problems • Ideally carried out between 18-20 wks • Complete scan should establish that there is a live, structurally normal intrauterine fetus, normal amniotic fluid volume, locate the placenta and establish that it is clear
Flashcard 1410136411404
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
The complete OB scan, aka 18-20 wk scan/anatomy scan
ete Obstetrical Scan (AKA Anatomy Scan) • Should be offered to all pregnant women as a screen for placental, fetal, and pregnancy problems • Ideally carried out between 18-20 wks • Complete scan should establish that there is a <span>live, structurally normal intrauterine fetus, normal amniotic fluid volume, locate the placenta and establish that it is clear of the internal os, and identify any uterine and adnexal abnormalities (fibroids, bands, septae,
Flashcard 1410137984268
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
The complete OB scan, aka 18-20 wk scan/anatomy scan
be offered to all pregnant women as a screen for placental, fetal, and pregnancy problems • Ideally carried out between 18-20 wks • Complete scan should establish that there is a live, structurally normal intrauterine fetus, normal <span>amniotic fluid volume, locate the placenta and establish that it is clear of the internal os, and identify any uterine and adnexal abnormalities (fibroids, bands, septae, short cervix, ovarian masses)
Flashcard 1410139557132
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
The complete OB scan, aka 18-20 wk scan/anatomy scan
as a screen for placental, fetal, and pregnancy problems • Ideally carried out between 18-20 wks • Complete scan should establish that there is a live, structurally normal intrauterine fetus, normal amniotic fluid volume, locate the <span>placenta and establish that it is clear of the internal os, and identify any uterine and adnexal abnormalities (fibroids, bands, septae, short cervix, ovarian masses)<span><body><html>
Flashcard 1410141129996
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
The complete OB scan, aka 18-20 wk scan/anatomy scan
problems • Ideally carried out between 18-20 wks • Complete scan should establish that there is a live, structurally normal intrauterine fetus, normal amniotic fluid volume, locate the placenta and establish that it is clear of the <span>internal os, and identify any uterine and adnexal abnormalities (fibroids, bands, septae, short cervix, ovarian masses)<span><body><html>
Flashcard 1410142702860
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
The complete OB scan, aka 18-20 wk scan/anatomy scan
ed out between 18-20 wks • Complete scan should establish that there is a live, structurally normal intrauterine fetus, normal amniotic fluid volume, locate the placenta and establish that it is clear of the internal os, and identify any <span>uterine and adnexal abnormalities (fibroids, bands, septae, short cervix, ovarian masses)<span><body><html>
Flashcard 1410144275724
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
The complete OB scan, aka 18-20 wk scan/anatomy scan
plete scan should establish that there is a live, structurally normal intrauterine fetus, normal amniotic fluid volume, locate the placenta and establish that it is clear of the internal os, and identify any uterine and adnexal abnormalities (<span>fibroids, bands, septae, short cervix, ovarian masses)<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410147159308
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Checking fetal growth with US
Fetal Growth • A healthy fetus should follow established growth curves which exist for estimated fetal weight (EFW), fetal abdominal circumference (AC), biparietal diameter (BPD), femur length (FL), etc. • Ultrasound estimation of fetal size/weight should NOT be repeated more often than q 2 week
Flashcard 1410148732172
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Checking fetal growth with US
Fetal Growth • A healthy fetus should follow established growth curves which exist for estimated fetal weight (EFW), fetal abdominal circumference (AC), biparietal diameter (BPD), femur length (FL), etc. • Ultrasound estimation of fetal size/weight should NOT be repeated more often than q 2 weeks for a reliable trend • A fetu
Flashcard 1410150305036
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Checking fetal growth with US
Fetal Growth • A healthy fetus should follow established growth curves which exist for estimated fetal weight (EFW), fetal abdominal circumference (AC), biparietal diameter (BPD), femur length (FL), etc. • Ultrasound estimation of fetal size/weight should NOT be repeated more often than q 2 weeks for a reliable trend • A fetus growing below the 10th ce
Flashcard 1410151877900
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Checking fetal growth with US
Fetal Growth • A healthy fetus should follow established growth curves which exist for estimated fetal weight (EFW), fetal abdominal circumference (AC), biparietal diameter (BPD), femur length (FL), etc. • Ultrasound estimation of fetal size/weight should NOT be repeated more often than q 2 weeks for a reliable trend • A fetus growing below the 10th centile or falling of
Flashcard 1410153450764
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Checking fetal growth with US
shed growth curves which exist for estimated fetal weight (EFW), fetal abdominal circumference (AC), biparietal diameter (BPD), femur length (FL), etc. • Ultrasound estimation of fetal size/weight should NOT be repeated more often than q <span>2 weeks for a reliable trend • A fetus growing below the 10th centile or falling off its growth curve may indicate fetal abnormality or compromise, requires more intensive monitoring
Flashcard 1410155023628
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Checking fetal growth with US
), fetal abdominal circumference (AC), biparietal diameter (BPD), femur length (FL), etc. • Ultrasound estimation of fetal size/weight should NOT be repeated more often than q 2 weeks for a reliable trend • A fetus growing below the <span>10th centile or falling off its growth curve may indicate fetal abnormality or compromise, requires more intensive monitoring and may require early delivery • Consider ethnicity – spe
Flashcard 1410156596492
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Checking fetal growth with US
(BPD), femur length (FL), etc. • Ultrasound estimation of fetal size/weight should NOT be repeated more often than q 2 weeks for a reliable trend • A fetus growing below the 10th centile or falling off its growth curve may indicate <span>fetal abnormality or compromise, requires more intensive monitoring and may require early delivery • Consider ethnicity – specific growth curves; twin-specific growth curves<span><body><html>
Flashcard 1410158169356
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Checking fetal growth with US
ion of fetal size/weight should NOT be repeated more often than q 2 weeks for a reliable trend • A fetus growing below the 10th centile or falling off its growth curve may indicate fetal abnormality or compromise, requires more intensive <span>monitoring and may require early delivery • Consider ethnicity – specific growth curves; twin-specific growth curves<span><body><html>
Flashcard 1410159742220
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Checking fetal growth with US
ould NOT be repeated more often than q 2 weeks for a reliable trend • A fetus growing below the 10th centile or falling off its growth curve may indicate fetal abnormality or compromise, requires more intensive monitoring and may require <span>early delivery • Consider ethnicity – specific growth curves; twin-specific growth curves<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410162625804
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
BPP
Biophysical Profile (BPP) • Ultrasound study of fetal gross body movement, tone, “breathing” movements, amniotic fluid volume • Each factor given a score of 2 if present, 0 if not present or decreased • Satisfactory score is 8 • Ultrasound para
Flashcard 1410164198668
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
BPP
Biophysical Profile (BPP) • Ultrasound study of fetal gross body movement, tone, “breathing” movements, amniotic fluid volume • Each factor given a score of 2 if present, 0 if not present or decreased • Satisfactory score is 8 • Ultrasound parameters
Flashcard 1410165771532
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
BPP
Biophysical Profile (BPP) • Ultrasound study of fetal gross body movement, tone, “breathing” movements, amniotic fluid volume • Each factor given a score of 2 if present, 0 if not present or decreased • Satisfactory score is 8 • Ultrasound parameters must be seen within a
Flashcard 1410167344396
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
BPP
Biophysical Profile (BPP) • Ultrasound study of fetal gross body movement, tone, “breathing” movements, amniotic fluid volume • Each factor given a score of 2 if present, 0 if not present or decreased • Satisfactory score is 8 • Ultrasound parameters must be seen within a 30-minute study: -
Flashcard 1410168917260
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
BPP
of fetal gross body movement, tone, “breathing” movements, amniotic fluid volume • Each factor given a score of 2 if present, 0 if not present or decreased • Satisfactory score is 8 • Ultrasound parameters must be seen within a <span>30-minute study: ----1 . Gross Body Movement: 3 discrete body or limb movements ----2 . Fetal Tone: one episode of active extension with return to flexion of limb or trunk (hand o
Flashcard 1410170490124
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
BPP
ements, amniotic fluid volume • Each factor given a score of 2 if present, 0 if not present or decreased • Satisfactory score is 8 • Ultrasound parameters must be seen within a 30-minute study: ----1 . Gross Body Movement: <span>3 discrete body or limb movements ----2 . Fetal Tone: one episode of active extension with return to flexion of limb or trunk (hand opening and closing also acceptable) ----3 .
Flashcard 1410172062988
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
BPP
sent, 0 if not present or decreased • Satisfactory score is 8 • Ultrasound parameters must be seen within a 30-minute study: ----1 . Gross Body Movement: 3 discrete body or limb movements ----2 . Fetal Tone: one episode of <span>active extension with return to flexion of limb or trunk (hand opening and closing also acceptable) ----3 . Breathing Movements: one 30-second episode of fetal breathing movement (fetal diaphragm or kidneys seen to move up and down, chest wall or abdomen in and out) ----4 .
Flashcard 1410173635852
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
BPP
; ----1 . Gross Body Movement: 3 discrete body or limb movements ----2 . Fetal Tone: one episode of active extension with return to flexion of limb or trunk (hand opening and closing also acceptable) ----3 . Breathing Movements: one <span>30-second episode of fetal breathing movement (fetal diaphragm or kidneys seen to move up and down, chest wall or abdomen in and out) ----4 . Amniotic Fluid (AF): single pocket of 2cm
Flashcard 1410175208716
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
BPP
or limb movements ----2 . Fetal Tone: one episode of active extension with return to flexion of limb or trunk (hand opening and closing also acceptable) ----3 . Breathing Movements: one 30-second episode of fetal breathing movement (<span>fetal diaphragm or kidneys seen to move up and down, chest wall or abdomen in and out) ----4 . Amniotic Fluid (AF): single pocket of 2cm x 2cm adequate for BPP Note that fetus may still have oligohydramnios with a BPP of 8/8. <span><body><html>
Flashcard 1410176781580
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
BPP
ng also acceptable) ----3 . Breathing Movements: one 30-second episode of fetal breathing movement (fetal diaphragm or kidneys seen to move up and down, chest wall or abdomen in and out) ----4 . Amniotic Fluid (AF): single pocket of <span>2cm x 2cm adequate for BPP Note that fetus may still have oligohydramnios with a BPP of 8/8. <span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410180189452
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
third trimester scan
Third trimester scan • some obstetricians order routine third trimester ultrasound around 32 weeks • currently, the cost/benefit is unproven • reserve ultrasound in third trimester for specific indications: growth, position, re-assessment of identified problems (e.g.
Flashcard 1410181762316
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
third trimester scan
ad>Third trimester scan • some obstetricians order routine third trimester ultrasound around 32 weeks • currently, the cost/benefit is unproven • reserve ultrasound in third trimester for specific indications: growth, position, re-assessment of identified problems (e.g. placenta if marginal or previa at 20 weeks, fetal pelviectasis)<html>
Flashcard 1410183335180
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
third trimester scan
>Third trimester scan • some obstetricians order routine third trimester ultrasound around 32 weeks • currently, the cost/benefit is unproven • reserve ultrasound in third trimester for specific indications: growth, position, re-assessment of identified problems (e.g. placenta if marginal or previa at 20 weeks, fetal pelviectasis)<body><html>
Flashcard 1410184908044
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
third trimester scan
icians order routine third trimester ultrasound around 32 weeks • currently, the cost/benefit is unproven • reserve ultrasound in third trimester for specific indications: growth, position, re-assessment of identified problems (e.g. <span>placenta if marginal or previa at 20 weeks, fetal pelviectasis)<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410187791628
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine prenatal care
Routine prenatal care schedule: • First visit ~ 8-12 weeks • Every 4 weeks until 28 weeks gestation • Every 2 weeks from 28-36 weeks gestation • Every week from 36 weeks to delivery • NIPT may be offered from approxima
Flashcard 1410189364492
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine prenatal care
Routine prenatal care schedule: • First visit ~ 8-12 weeks • Every 4 weeks until 28 weeks gestation • Every 2 weeks from 28-36 weeks gestation • Every week from 36 weeks to delivery • NIPT may be offered from approximately 10 weeks on
Flashcard 1410190937356
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine prenatal care
Routine prenatal care schedule: • First visit ~ 8-12 weeks • Every 4 weeks until 28 weeks gestation • Every 2 weeks from 28-36 weeks gestation • Every week from 36 weeks to delivery • NIPT may be offered from approximately 10 weeks on • 11-14 wks: I
Flashcard 1410192510220
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine prenatal care
Routine prenatal care schedule: • First visit ~ 8-12 weeks • Every 4 weeks until 28 weeks gestation • Every 2 weeks from 28-36 weeks gestation • Every week from 36 weeks to delivery • NIPT may be offered from approximately 10 weeks on • 11-14 wks: IPS Part I or FTS if desired
Flashcard 1410194083084
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine prenatal care
Routine prenatal care schedule: • First visit ~ 8-12 weeks • Every 4 weeks until 28 weeks gestation • Every 2 weeks from 28-36 weeks gestation • Every week from 36 weeks to delivery • NIPT may be offered from approximately 10 weeks on • 11-14 wks: IPS Part I or FTS if desired • 15-20 wks: IP
Flashcard 1410195655948
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine prenatal care
Routine prenatal care schedule: • First visit ~ 8-12 weeks • Every 4 weeks until 28 weeks gestation • Every 2 weeks from 28-36 weeks gestation • Every week from 36 weeks to delivery • NIPT may be offered from approximately 10 weeks on • 11-14 wks: IPS Part I or FTS if desired • 15-20 wks: IPS Part II or Maternal serum alpha-fetoprot
Flashcard 1410197228812
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine prenatal care
Routine prenatal care schedule: • First visit ~ 8-12 weeks • Every 4 weeks until 28 weeks gestation • Every 2 weeks from 28-36 weeks gestation • Every week from 36 weeks to delivery • NIPT may be offered from approximately 10 weeks on • 11-14 wks: IPS Part I or FTS if desired • 15-20 wks: IPS Part II or Maternal serum alpha-
Flashcard 1410198801676
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine prenatal care
ne prenatal care schedule: • First visit ~ 8-12 weeks • Every 4 weeks until 28 weeks gestation • Every 2 weeks from 28-36 weeks gestation • Every week from 36 weeks to delivery • NIPT may be offered from approximately <span>10 weeks on • 11-14 wks: IPS Part I or FTS if desired • 15-20 wks: IPS Part II or Maternal serum alpha-fetoprotein or Quad screen if want genetic screening and not tested in firs
Flashcard 1410200374540
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine prenatal care
; • First visit ~ 8-12 weeks • Every 4 weeks until 28 weeks gestation • Every 2 weeks from 28-36 weeks gestation • Every week from 36 weeks to delivery • NIPT may be offered from approximately 10 weeks on • 11-14 wks: <span>IPS Part I or FTS if desired • 15-20 wks: IPS Part II or Maternal serum alpha-fetoprotein or Quad screen if want genetic screening and not tested in first trimester • 18-20 wks: Anatomy ultraso
Flashcard 1410201947404
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine prenatal care
hedule: • First visit ~ 8-12 weeks • Every 4 weeks until 28 weeks gestation • Every 2 weeks from 28-36 weeks gestation • Every week from 36 weeks to delivery • NIPT may be offered from approximately 10 weeks on • <span>11-14 wks: IPS Part I or FTS if desired • 15-20 wks: IPS Part II or Maternal serum alpha-fetoprotein or Quad screen if want genetic screening and not tested in first trimester • 18-
Flashcard 1410203520268
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine prenatal care
Every 4 weeks until 28 weeks gestation • Every 2 weeks from 28-36 weeks gestation • Every week from 36 weeks to delivery • NIPT may be offered from approximately 10 weeks on • 11-14 wks: IPS Part I or FTS if desired • <span>15-20 wks: IPS Part II or Maternal serum alpha-fetoprotein or Quad screen if want genetic screening and not tested in first trimester • 18-20 wks: Anatomy ultrasound • 27-29 wks: Or
Flashcard 1410205093132
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine prenatal care
ks until 28 weeks gestation • Every 2 weeks from 28-36 weeks gestation • Every week from 36 weeks to delivery • NIPT may be offered from approximately 10 weeks on • 11-14 wks: IPS Part I or FTS if desired • 15-20 wks: <span>IPS Part II or Maternal serum alpha-fetoprotein or Quad screen if want genetic screening and not tested in first trimester • 18-20 wks: Anatomy ultrasound • 27-29 wks: Oral glucose challe
Flashcard 1410207452428
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine prenatal care
ks gestation • Every 2 weeks from 28-36 weeks gestation • Every week from 36 weeks to delivery • NIPT may be offered from approximately 10 weeks on • 11-14 wks: IPS Part I or FTS if desired • 15-20 wks: IPS Part II or <span>Quad screen if want genetic screening and not tested in first trimester • 18-20 wks: Anatomy ultrasound • 27-29 wks: Oral glucose challenge test, Rh immune globulin (RhIG/Rhogam) for Rh negative patients, CBC • 36 wks: vagino-rectal swab for
Flashcard 1410209025292
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine prenatal care
from 36 weeks to delivery • NIPT may be offered from approximately 10 weeks on • 11-14 wks: IPS Part I or FTS if desired • 15-20 wks: IPS Part II or Quad screen if want genetic screening and not tested in first trimester • <span>18-20 wks: Anatomy ultrasound • 27-29 wks: Oral glucose challenge test, Rh immune globulin (RhIG/Rhogam) for Rh negative patients, CBC • 36 wks: vagino-rectal swab for Group B strep
Flashcard 1410210598156
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine prenatal care
ks to delivery • NIPT may be offered from approximately 10 weeks on • 11-14 wks: IPS Part I or FTS if desired • 15-20 wks: IPS Part II or Quad screen if want genetic screening and not tested in first trimester • 18-20 wks: <span>Anatomy ultrasound • 27-29 wks: Oral glucose challenge test, Rh immune globulin (RhIG/Rhogam) for Rh negative patients, CBC • 36 wks: vagino-rectal swab for Group B streptococcus • 40+ wks:
Flashcard 1410212171020
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine prenatal care
may be offered from approximately 10 weeks on • 11-14 wks: IPS Part I or FTS if desired • 15-20 wks: IPS Part II or Quad screen if want genetic screening and not tested in first trimester • 18-20 wks: Anatomy ultrasound • <span>27-29 wks: Oral glucose challenge test, Rh immune globulin (RhIG/Rhogam) for Rh negative patients, CBC • 36 wks: vagino-rectal swab for Group B streptococcus • 40+ wks: weekly bioph
Flashcard 1410213743884
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine prenatal care
ered from approximately 10 weeks on • 11-14 wks: IPS Part I or FTS if desired • 15-20 wks: IPS Part II or Quad screen if want genetic screening and not tested in first trimester • 18-20 wks: Anatomy ultrasound • 27-29 wks: <span>Oral glucose challenge test, Rh immune globulin (RhIG/Rhogam) for Rh negative patients, CBC • 36 wks: vagino-rectal swab for Group B streptococcus • 40+ wks: weekly biophysical profile for post-date
Flashcard 1410215316748
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine prenatal care
eks on • 11-14 wks: IPS Part I or FTS if desired • 15-20 wks: IPS Part II or Quad screen if want genetic screening and not tested in first trimester • 18-20 wks: Anatomy ultrasound • 27-29 wks: Oral glucose challenge test, <span>Rh immune globulin (RhIG/Rhogam) for Rh negative patients, CBC • 36 wks: vagino-rectal swab for Group B streptococcus • 40+ wks: weekly biophysical profile for post-dates • Should be delivered prior to 42 weeks (plan IOL at 41+3
Flashcard 1410216889612
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine prenatal care
• 15-20 wks: IPS Part II or Quad screen if want genetic screening and not tested in first trimester • 18-20 wks: Anatomy ultrasound • 27-29 wks: Oral glucose challenge test, Rh immune globulin (RhIG/Rhogam) for Rh negative patients, <span>CBC • 36 wks: vagino-rectal swab for Group B streptococcus • 40+ wks: weekly biophysical profile for post-dates • Should be delivered prior to 42 weeks (plan IOL at 41+3)</sp
Flashcard 1410218462476
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine prenatal care
: IPS Part II or Quad screen if want genetic screening and not tested in first trimester • 18-20 wks: Anatomy ultrasound • 27-29 wks: Oral glucose challenge test, Rh immune globulin (RhIG/Rhogam) for Rh negative patients, CBC • <span>36 wks: vagino-rectal swab for Group B streptococcus • 40+ wks: weekly biophysical profile for post-dates • Should be delivered prior to 42 weeks (plan IOL at 41+3)<span>
Flashcard 1410220035340
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine prenatal care
want genetic screening and not tested in first trimester • 18-20 wks: Anatomy ultrasound • 27-29 wks: Oral glucose challenge test, Rh immune globulin (RhIG/Rhogam) for Rh negative patients, CBC • 36 wks: vagino-rectal swab for <span>Group B streptococcus • 40+ wks: weekly biophysical profile for post-dates • Should be delivered prior to 42 weeks (plan IOL at 41+3)<span><body><html>
Flashcard 1410221608204
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine prenatal care
ot tested in first trimester • 18-20 wks: Anatomy ultrasound • 27-29 wks: Oral glucose challenge test, Rh immune globulin (RhIG/Rhogam) for Rh negative patients, CBC • 36 wks: vagino-rectal swab for Group B streptococcus • <span>40+ wks: weekly biophysical profile for post-dates • Should be delivered prior to 42 weeks (plan IOL at 41+3)<span><body><html>
Flashcard 1410223181068
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine prenatal care
st trimester • 18-20 wks: Anatomy ultrasound • 27-29 wks: Oral glucose challenge test, Rh immune globulin (RhIG/Rhogam) for Rh negative patients, CBC • 36 wks: vagino-rectal swab for Group B streptococcus • 40+ wks: weekly <span>biophysical profile for post-dates • Should be delivered prior to 42 weeks (plan IOL at 41+3)<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410228161804
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Testing for GDM
Testing for GDM: • Current standard of care is to investigate all pregnancies with oral glucose challenge test Glucose Challenge Test (GCT): • no preparation required and no fasting prior to test needed • 50g oral glucose load is given • wait one hour after drink with
Flashcard 1410230521100
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Testing for GDM
pan>Testing for GDM: • Current standard of care is to investigate all pregnancies with oral glucose challenge test Glucose Challenge Test (GCT): • no preparation required and no fasting prior to test needed • 50g oral glucose load is given • wait one hour after drink with no eating or drinking during this time, then draw blood for glucose test • blood glucose <7.8 is considered a n
Flashcard 1410232093964
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Testing for GDM
tandard of care is to investigate all pregnancies with oral glucose challenge test Glucose Challenge Test (GCT): • no preparation required and no fasting prior to test needed • 50g oral glucose load is given • wait <span>one hour after drink with no eating or drinking during this time, then draw blood for glucose test • blood glucose <7.8 is considered a negative screen • if result is 11.1 mmol
Flashcard 1410233666828
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Testing for GDM
• no preparation required and no fasting prior to test needed • 50g oral glucose load is given • wait one hour after drink with no eating or drinking during this time, then draw blood for glucose test • blood glucose <<span>7.8 is considered a negative screen • if result is 11.1 mmol/L, gestation diabetes is present • if value is between 7.8 and 11.0, follow with glucose tolerance test Gl
Flashcard 1410235239692
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Testing for GDM
test needed • 50g oral glucose load is given • wait one hour after drink with no eating or drinking during this time, then draw blood for glucose test • blood glucose <7.8 is considered a negative screen • if result is <span>11.1 mmol/L, gestation diabetes is present • if value is between 7.8 and 11.0, follow with glucose tolerance test Glucose Tolerance Test (GTT): • patient must fast fro
Flashcard 1410236812556
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Testing for GDM
r after drink with no eating or drinking during this time, then draw blood for glucose test • blood glucose <7.8 is considered a negative screen • if result is 11.1 mmol/L, gestation diabetes is present • if value is between <span>7.8 and 11.0, follow with glucose tolerance test Glucose Tolerance Test (GTT): • patient must fast from night before • fasting blood sugar drawn in the morning • 75g oral
Flashcard 1410238385420
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Testing for GDM
ation diabetes is present • if value is between 7.8 and 11.0, follow with glucose tolerance test Glucose Tolerance Test (GTT): • patient must fast from night before • fasting blood sugar drawn in the morning • <span>75g oral glucose load is given • blood is drawn again 1 and then 2 hours after the drink is completed • Abnormal for 75g 2-hour GTT: ---1 . FBS ≥ 5.3 mmol/L ---2 . 1-ho
Flashcard 1410239958284
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Testing for GDM
d 11.0, follow with glucose tolerance test Glucose Tolerance Test (GTT): • patient must fast from night before • fasting blood sugar drawn in the morning • 75g oral glucose load is given • blood is drawn again <span>1 and then 2 hours after the drink is completed • Abnormal for 75g 2-hour GTT: ---1 . FBS ≥ 5.3 mmol/L ---2 . 1-hour ≥ 10.6 mmol/L ---3 . 2-hour ≥ 9.0 mmol/L • one abnormal
Flashcard 1410241531148
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Testing for GDM
ust fast from night before • fasting blood sugar drawn in the morning • 75g oral glucose load is given • blood is drawn again 1 and then 2 hours after the drink is completed • Abnormal for 75g 2-hour GTT: ---1 . FBS ≥ <span>5.3 mmol/L ---2 . 1-hour ≥ 10.6 mmol/L ---3 . 2-hour ≥ 9.0 mmol/L • one abnormal value = GDM Postpartum: • Ensure postpartum follow-up: pts with GDM should have a
Flashcard 1410243104012
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Testing for GDM
• fasting blood sugar drawn in the morning • 75g oral glucose load is given • blood is drawn again 1 and then 2 hours after the drink is completed • Abnormal for 75g 2-hour GTT: ---1 . FBS ≥ 5.3 mmol/L ---2 . 1-hour ≥ <span>10.6 mmol/L ---3 . 2-hour ≥ 9.0 mmol/L • one abnormal value = GDM Postpartum: • Ensure postpartum follow-up: pts with GDM should have a GTT between 6wks and 6 months po
Flashcard 1410244676876
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Testing for GDM
e morning • 75g oral glucose load is given • blood is drawn again 1 and then 2 hours after the drink is completed • Abnormal for 75g 2-hour GTT: ---1 . FBS ≥ 5.3 mmol/L ---2 . 1-hour ≥ 10.6 mmol/L ---3 . 2-hour ≥ <span>9.0 mmol/L • one abnormal value = GDM Postpartum: • Ensure postpartum follow-up: pts with GDM should have a GTT between 6wks and 6 months postpartum, with appropriate follo
Flashcard 1410246249740
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Testing for GDM
al for 75g 2-hour GTT: ---1 . FBS ≥ 5.3 mmol/L ---2 . 1-hour ≥ 10.6 mmol/L ---3 . 2-hour ≥ 9.0 mmol/L • one abnormal value = GDM Postpartum: • Ensure postpartum follow-up: pts with GDM should have a GTT between <span>6wks and 6 months postpartum, with appropriate follow-up with endocrinology or their family doctor • Patients with GDM have a very high risk of developing future DMII: may be impetus to improve diet
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410249133324
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Rhogam
Rh Immune Globulin (Rhogam, RhIG) • Indicated if mother is Rh negative and has no Rh antibodies • Given at 28 weeks or whenever there is possibility of feto-maternal hemorrhage (e.g. spontaneous abortion, termination, ectopic, CVS/amniocentesis, antep
Flashcard 1410250706188
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Rhogam
Rh Immune Globulin (Rhogam, RhIG) • Indicated if mother is Rh negative and has no Rh antibodies • Given at 28 weeks or whenever there is possibility of feto-maternal hemorrhage (e.g. spontaneous abortion, termination, ectopic, CVS/amniocentesis, antepartum hemorrhage, postpar
Flashcard 1410252279052
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Rhogam
Rh Immune Globulin (Rhogam, RhIG) • Indicated if mother is Rh negative and has no Rh antibodies • Given at 28 weeks or whenever there is possibility of feto-maternal hemorrhage (e.g. spontaneous abortion, termination, ectopic, CVS/amniocentesis, antepartum hemorrhage, postpartum) • Protect
Flashcard 1410253851916
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Rhogam
Rh Immune Globulin (Rhogam, RhIG) • Indicated if mother is Rh negative and has no Rh antibodies • Given at 28 weeks or whenever there is possibility of feto-maternal hemorrhage (e.g. spontaneous abortion, termination, ectopic, CVS/amniocentesis, antepartum hemorrhage, postpartum) • Protection lasts approximately 12 weeks • During this time, patient’s
Flashcard 1410255424780
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Rhogam
Rh Immune Globulin (Rhogam, RhIG) • Indicated if mother is Rh negative and has no Rh antibodies • Given at 28 weeks or whenever there is possibility of feto-maternal hemorrhage (e.g. spontaneous abortion, termination, ectopic, CVS/amniocentesis, antepartum hemorrhage, postpartum) • Protection lasts approximately 12 weeks • During this time, patient’s antibody screen will be positive • Consider testing the father: if father Rh negative as well the
Flashcard 1410256997644
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Rhogam
Rh antibodies • Given at 28 weeks or whenever there is possibility of feto-maternal hemorrhage (e.g. spontaneous abortion, termination, ectopic, CVS/amniocentesis, antepartum hemorrhage, postpartum) • Protection lasts approximately <span>12 weeks • During this time, patient’s antibody screen will be positive • Consider testing the father: if father Rh negative as well then baby must be Rh negative and Rhogam will
Flashcard 1410258570508
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Rhogam
neous abortion, termination, ectopic, CVS/amniocentesis, antepartum hemorrhage, postpartum) • Protection lasts approximately 12 weeks • During this time, patient’s antibody screen will be positive • Consider testing the father: <span>if father Rh negative as well then baby must be Rh negative and Rhogam will not be required • Ensure patient understands the potential severity of alloimmunization. She must be certain as to paternity if declining RhIG - if in doubt, give anyway • Rhogam is an IgG an
Flashcard 1410260143372
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Rhogam
e positive • Consider testing the father: if father Rh negative as well then baby must be Rh negative and Rhogam will not be required • Ensure patient understands the potential severity of alloimmunization. She must be certain as to <span>paternity if declining RhIG - if in doubt, give anyway • Rhogam is an IgG antibody, which prevents mother from mounting an immune response to any Rh positive fetal red blood cells in the mat
Flashcard 1410261716236
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Rhogam
l then baby must be Rh negative and Rhogam will not be required • Ensure patient understands the potential severity of alloimmunization. She must be certain as to paternity if declining RhIG - if in doubt, give anyway • Rhogam is an <span>IgG antibody, which prevents mother from mounting an immune response to any Rh positive fetal red blood cells in the maternal circulation during pregnancy • Dose is 300 mcg given intra
Flashcard 1410263289100
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Rhogam
e patient understands the potential severity of alloimmunization. She must be certain as to paternity if declining RhIG - if in doubt, give anyway • Rhogam is an IgG antibody, which prevents mother from mounting an immune response to any <span>Rh positive fetal red blood cells in the maternal circulation during pregnancy • Dose is 300 mcg given intramuscularly at 28 weeks’ gestation: standard dose is sufficient to protect against ~25 mls of fetal blood&#
Flashcard 1410264861964
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Rhogam
ternity if declining RhIG - if in doubt, give anyway • Rhogam is an IgG antibody, which prevents mother from mounting an immune response to any Rh positive fetal red blood cells in the maternal circulation during pregnancy • Dose is <span>300 mcg given intramuscularly at 28 weeks’ gestation: standard dose is sufficient to protect against ~25 mls of fetal blood • Do Betke-Kleihauer test and adjust dose if suspect larger feto
Flashcard 1410266434828
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Rhogam
doubt, give anyway • Rhogam is an IgG antibody, which prevents mother from mounting an immune response to any Rh positive fetal red blood cells in the maternal circulation during pregnancy • Dose is 300 mcg given intramuscularly at <span>28 weeks’ gestation: standard dose is sufficient to protect against ~25 mls of fetal blood • Do Betke-Kleihauer test and adjust dose if suspect larger feto-maternal hemorrhage •
Flashcard 1410268007692
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Rhogam
mother from mounting an immune response to any Rh positive fetal red blood cells in the maternal circulation during pregnancy • Dose is 300 mcg given intramuscularly at 28 weeks’ gestation: standard dose is sufficient to protect against ~<span>25 mls of fetal blood • Do Betke-Kleihauer test and adjust dose if suspect larger feto-maternal hemorrhage • The blood group and antibody screen (G&S) ordered at the first an
Flashcard 1410271677708
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Rhogam
ks’ gestation: standard dose is sufficient to protect against ~25 mls of fetal blood • Do Betke-Kleihauer test and adjust dose if suspect larger feto-maternal hemorrhage • The blood group and antibody screen (G&S) ordered at the <span>first antenatal visit will identify if mother already has Rh antibodies - Rhogam not given to patients already alloimmunized<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410274561292
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
GBS status
Group B Streptococcus (GBS) status: • Done at 36 weeks (earlier if threatened preterm labour) • Single combined culture from vagina and anorectal area - patient may do own swab after instruction • If positive, antibiotic pro
Flashcard 1410276134156
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
GBS status
body>Group B Streptococcus (GBS) status: • Done at 36 weeks (earlier if threatened preterm labour) • Single combined culture from vagina and anorectal area - patient may do own swab after instruction • If positive, antibiotic prophylaxis given in labour to reduce risk of neonatal GBS infection • If negative, swab within 5 weeks of delivery, no antibiotics in labour unless indicated for maternal pyrexia, etc. •
Flashcard 1410277707020
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
GBS status
our) • Single combined culture from vagina and anorectal area - patient may do own swab after instruction • If positive, antibiotic prophylaxis given in labour to reduce risk of neonatal GBS infection • If negative, swab within <span>5 weeks of delivery, no antibiotics in labour unless indicated for maternal pyrexia, etc. • If any GBS bacteriuria during pregnancy, treat as GBS positive (indicator of heavy coloniz
Flashcard 1410279279884
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
GBS status
uction • If positive, antibiotic prophylaxis given in labour to reduce risk of neonatal GBS infection • If negative, swab within 5 weeks of delivery, no antibiotics in labour unless indicated for maternal pyrexia, etc. • If any <span>GBS bacteriuria during pregnancy, treat as GBS positive (indicator of heavy colonization, no need to do vaginal-rectal swab) • This is NOT a maternal infection: about 10-30% of women are carriers
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410282425612
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine Investigations at First Visit
Routine Investigations at First Visit: • CBC • Rubella status • Hepatitis B Surface Antigen • VDRL (Syphilis) • Blood Group and Rh status, Antibody Screen (to check for red blood cell antibodies) • Urinaly
Flashcard 1410283998476
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine Investigations at First Visit
Routine Investigations at First Visit: • CBC • Rubella status • Hepatitis B Surface Antigen • VDRL (Syphilis) • Blood Group and Rh status, Antibody Screen (to check for red blood cell antibodies) • Urinalysis (Routine an
Flashcard 1410285571340
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine Investigations at First Visit
Routine Investigations at First Visit: • CBC • Rubella status • Hepatitis B Surface Antigen • VDRL (Syphilis) • Blood Group and Rh status, Antibody Screen (to check for red blood cell antibodies) • Urinalysis (Routine and Microscopic) • Mid-
Flashcard 1410287144204
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine Investigations at First Visit
Routine Investigations at First Visit: • CBC • Rubella status • Hepatitis B Surface Antigen • VDRL (Syphilis) • Blood Group and Rh status, Antibody Screen (to check for red blood cell antibodies) • Urinalysis (Routine and Microscopic) • Mid-Stream Urine (MSU) for culture and sens
Flashcard 1410288717068
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine Investigations at First Visit
Routine Investigations at First Visit: • CBC • Rubella status • Hepatitis B Surface Antigen • VDRL (Syphilis) • Blood Group and Rh status, Antibody Screen (to check for red blood cell antibodies) • Urinalysis (Routine and Microscopic) • Mid-Stream Urine (MSU) for culture and sensitivity (2-7% or women hav
Flashcard 1410290289932
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine Investigations at First Visit
y>Routine Investigations at First Visit: • CBC • Rubella status • Hepatitis B Surface Antigen • VDRL (Syphilis) • Blood Group and Rh status, Antibody Screen (to check for red blood cell antibodies) • Urinalysis (Routine and Microscopic) • Mid-Stream Urine (MSU) for culture and sensitivity (2-7% or women have asymptomatic bacteriuria) • Pap smear, if due • Cervical cultures or urine screen for Gonorrhea a
Flashcard 1410291862796
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine Investigations at First Visit
t Visit: • CBC • Rubella status • Hepatitis B Surface Antigen • VDRL (Syphilis) • Blood Group and Rh status, Antibody Screen (to check for red blood cell antibodies) • Urinalysis (Routine and Microscopic) • <span>Mid-Stream Urine (MSU) for culture and sensitivity (2-7% or women have asymptomatic bacteriuria) • Pap smear, if due • Cervical cultures or urine screen for Gonorrhea and Chlamydia • TSH routin
Flashcard 1410293435660
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine Investigations at First Visit
; • Blood Group and Rh status, Antibody Screen (to check for red blood cell antibodies) • Urinalysis (Routine and Microscopic) • Mid-Stream Urine (MSU) for culture and sensitivity (2-7% or women have asymptomatic bacteriuria) • <span>Pap smear, if due • Cervical cultures or urine screen for Gonorrhea and Chlamydia • TSH routinely done by many OBs; TSH often physiologically depressed in early pregnancy, value of rout
Flashcard 1410295008524
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine Investigations at First Visit
d blood cell antibodies) • Urinalysis (Routine and Microscopic) • Mid-Stream Urine (MSU) for culture and sensitivity (2-7% or women have asymptomatic bacteriuria) • Pap smear, if due • Cervical cultures or urine screen for <span>Gonorrhea and Chlamydia • TSH routinely done by many OBs; TSH often physiologically depressed in early pregnancy, value of routine TSH screening is currently in doubt (2015 ACOG Guideline recommended agai
Flashcard 1410296581388
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine Investigations at First Visit
atus, Antibody Screen (to check for red blood cell antibodies) • Urinalysis (Routine and Microscopic) • Mid-Stream Urine (MSU) for culture and sensitivity (2-7% or women have asymptomatic bacteriuria) • Pap smear, if due • <span>Cervical cultures or urine screen for Gonorrhea and Chlamydia • TSH routinely done by many OBs; TSH often physiologically depressed in early pregnancy, value of routine TSH screening is currently in doubt (2015 ACO
Flashcard 1410298154252
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine Investigations at First Visit
cultures or urine screen for Gonorrhea and Chlamydia • TSH routinely done by many OBs; TSH often physiologically depressed in early pregnancy, value of routine TSH screening is currently in doubt (2015 ACOG Guideline recommended against <span>routine screening of asymptomatic women)<span><body><html>
Flashcard 1410299727116
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Routine Investigations at First Visit
ine (MSU) for culture and sensitivity (2-7% or women have asymptomatic bacteriuria) • Pap smear, if due • Cervical cultures or urine screen for Gonorrhea and Chlamydia • TSH routinely done by many OBs; TSH often physiologically <span>depressed in early pregnancy, value of routine TSH screening is currently in doubt (2015 ACOG Guideline recommended against routine screening of asymptomatic women)<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410301824268
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410305232140
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Consented investigations - HIV
tions in pregnancy - HIV • Long-term maternal outcomes are better if HIV+ status is known and treated • Known HIV+ status allows people to practice safer sex and protect partners (if uninfected) • Dramatically decreased risk of <span>vertical transmission to fetus if optimally treated in pregnancy (from 25% to 2%) • Breastfeeding contraindicated • Diagnosis of HIV+ status can impact current and previous partner(s), family, abil
Flashcard 1410306805004
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Consented investigations - HIV
known and treated • Known HIV+ status allows people to practice safer sex and protect partners (if uninfected) • Dramatically decreased risk of vertical transmission to fetus if optimally treated in pregnancy (from 25% to 2%) • <span>Breastfeeding contraindicated • Diagnosis of HIV+ status can impact current and previous partner(s), family, ability to obtain health and life insurance<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410309688588
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Consented investigations - Hep C
Consented investigations in pregnancy - Hep C • If positive for HIV, Hepatitis B or other risk factors (blood transfusion prior to 1984 and untested, current or previous partner with known infection, intravenous drug use, sex trade workers, extensive pi
Flashcard 1410311261452
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Consented investigations - Hep C
Consented investigations in pregnancy - Hep C • If positive for HIV, Hepatitis B or other risk factors (blood transfusion prior to 1984 and untested, current or previous partner with known infection, intravenous drug use, sex trade workers, extensive piercing or tat
Flashcard 1410312834316
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Consented investigations - Hep C
Consented investigations in pregnancy - Hep C • If positive for HIV, Hepatitis B or other risk factors (blood transfusion prior to 1984 and untested, current or previous partner with known infection, intravenous drug use, sex trade workers, extensive piercing or tattooing) • No vaccine or cure but appropriate treatment and Counselling can result in better outcomes • Vertical transmission rate low (5%) • Diagnosis of HepC+ status can impact
Flashcard 1410314407180
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Consented investigations - Hep C
#13; • If positive for HIV, Hepatitis B or other risk factors (blood transfusion prior to 1984 and untested, current or previous partner with known infection, intravenous drug use, sex trade workers, extensive piercing or tattooing) • No <span>vaccine or cure but appropriate treatment and Counselling can result in better outcomes • Vertical transmission rate low (5%) • Diagnosis of HepC+ status can impact current and previous partn
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410317290764
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Consented investigations - herpes simplex
Consented investigations in pregnancy - Herpes Simplex • If visible vulvar ulcers • Treatment during pregnancy can shorten outbreaks • Prophylaxis can be given in third trimester to decrease need for Cesarean section (due to active outbreak at the time of l
Flashcard 1410318863628
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Consented investigations - herpes simplex
Consented investigations in pregnancy - Herpes Simplex • If visible vulvar ulcers • Treatment during pregnancy can shorten outbreaks • Prophylaxis can be given in third trimester to decrease need for Cesarean section (due to active outbreak at the time of labour)
Flashcard 1410320436492
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Consented investigations - herpes simplex
Consented investigations in pregnancy - Herpes Simplex • If visible vulvar ulcers • Treatment during pregnancy can shorten outbreaks • Prophylaxis can be given in third trimester to decrease need for Cesarean section (due to active outbreak at the time of labour)
Flashcard 1410322009356
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Consented investigations - herpes simplex
n>Consented investigations in pregnancy - Herpes Simplex • If visible vulvar ulcers • Treatment during pregnancy can shorten outbreaks • Prophylaxis can be given in third trimester to decrease need for Cesarean section (due to <span>active outbreak at the time of labour)<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410324892940
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Other investigations to consider in pregnancy
Other investigations to consider in pregnancy: • Varicella zoster titre (if no clear history of childhood infection) • Toxoplasmosis (house pets, gardeners) • Parvovirus B19 (primary school teachers, daycare workers) • Early GCT/ GTT if
Flashcard 1410326465804
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Other investigations to consider in pregnancy
Other investigations to consider in pregnancy: • Varicella zoster titre (if no clear history of childhood infection) • Toxoplasmosis (house pets, gardeners) • Parvovirus B19 (primary school teachers, daycare workers) • Early GCT/ GTT if: ---• previously large infant ---• obesity ---• previous
Flashcard 1410328038668
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Other investigations to consider in pregnancy
Other investigations to consider in pregnancy: • Varicella zoster titre (if no clear history of childhood infection) • Toxoplasmosis (house pets, gardeners) • Parvovirus B19 (primary school teachers, daycare workers) • Early GCT/ GTT if: ---• previously large infant ---• obesity ---• previous gestational diabetes • Sickle cell scree
Flashcard 1410329611532
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Other investigations to consider in pregnancy
regnancy: • Varicella zoster titre (if no clear history of childhood infection) • Toxoplasmosis (house pets, gardeners) • Parvovirus B19 (primary school teachers, daycare workers) • Early GCT/ GTT if: ---• previously <span>large infant ---• obesity ---• previous gestational diabetes • Sickle cell screen/hemoglobin electrophoresis/Ashkenazi panel depending on ethnic background, history • Hemoglobin
Flashcard 1410331184396
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Other investigations to consider in pregnancy
ella zoster titre (if no clear history of childhood infection) • Toxoplasmosis (house pets, gardeners) • Parvovirus B19 (primary school teachers, daycare workers) • Early GCT/ GTT if: ---• previously large infant ---• <span>obesity ---• previous gestational diabetes • Sickle cell screen/hemoglobin electrophoresis/Ashkenazi panel depending on ethnic background, history • Hemoglobin A1C (pre-gestation
Flashcard 1410332757260
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Other investigations to consider in pregnancy
ear history of childhood infection) • Toxoplasmosis (house pets, gardeners) • Parvovirus B19 (primary school teachers, daycare workers) • Early GCT/ GTT if: ---• previously large infant ---• obesity ---• previous <span>gestational diabetes • Sickle cell screen/hemoglobin electrophoresis/Ashkenazi panel depending on ethnic background, history • Hemoglobin A1C (pre-gestational diabetic patients) • TB (family
Flashcard 1410334330124
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Other investigations to consider in pregnancy
workers) • Early GCT/ GTT if: ---• previously large infant ---• obesity ---• previous gestational diabetes • Sickle cell screen/hemoglobin electrophoresis/Ashkenazi panel depending on ethnic background, history • <span>Hemoglobin A1C (pre-gestational diabetic patients) • TB (family or household contact, symptoms, homeless)<span><body><html>
Flashcard 1410335902988
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Other investigations to consider in pregnancy
rge infant ---• obesity ---• previous gestational diabetes • Sickle cell screen/hemoglobin electrophoresis/Ashkenazi panel depending on ethnic background, history • Hemoglobin A1C (pre-gestational diabetic patients) • <span>TB (family or household contact, symptoms, homeless)<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410338000140
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410341670156
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410346126604
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
NIPT
NIPT (Non-Invasive Prenatal Testing): • Peripheral blood test which analyzes cell-free fetal DNA in the maternal circulation • Screens abnormalities of chromosomes 21, 18, 13, X and Y • Very high detection rate for Down Syndrome (>99%), as well as Trisomy 18 and 13 whe
Flashcard 1410347699468
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
NIPT
NIPT (Non-Invasive Prenatal Testing): • Peripheral blood test which analyzes cell-free fetal DNA in the maternal circulation • Screens abnormalities of chromosomes 21, 18, 13, X and Y • Very high detection rate for Down Syndrome (>99%), as well as Trisomy 18 and 13 when validated in high-risk pregnancies • Applicable for singleton and uncomplicated twin
Flashcard 1410349272332
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
NIPT
of chromosomes 21, 18, 13, X and Y • Very high detection rate for Down Syndrome (>99%), as well as Trisomy 18 and 13 when validated in high-risk pregnancies • Applicable for singleton and uncomplicated twin pregnancies from about <span>10 weeks • Cost approx. $500 - Ontario Ministry of Health will cover cost for women aged 40 and over, or with positive screening tests or other major risk factors.<span></body
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410352155916
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
CVS - invasive diagnostic testing
Chorionic Villus Sampling (CVS): • 10-14 wks • Placental biopsy via transcervical or transabdominal approach • Preliminary results for very high risk patients may be available in a few days [by fluorescence in-situ h
Flashcard 1410353728780
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
CVS - invasive diagnostic testing
Chorionic Villus Sampling (CVS): • 10-14 wks • Placental biopsy via transcervical or transabdominal approach • Preliminary results for very high risk patients may be available in a few days [by fluorescence in-situ hybridization (“FISH”)
Flashcard 1410355301644
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
CVS - invasive diagnostic testing
al or transabdominal approach • Preliminary results for very high risk patients may be available in a few days [by fluorescence in-situ hybridization (“FISH”) analysis or QF-PCR (polymerase chain reaction)]; microarray may be done • <span>Early termination of affected pregnancies can be offered (psychological and physical advantages) • Procedure related pregnancy loss rate 1-2% • Slightly higher rate of cell culture failure than
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410358185228
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
amniocentesis
Amniocentesis : • Normally 15 to 20 weeks but in special circumstances may be done at any time after 15 weeks • Collection of amniotic fluid transabdominally under ultrasound guidance • Karyotype of fetal cells
Flashcard 1410359758092
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
amniocentesis
Amniocentesis : • Normally 15 to 20 weeks but in special circumstances may be done at any time after 15 weeks • Collection of amniotic fluid transabdominally under ultrasound guidance • Karyotype of fetal cells obtained from amniotic fluid – FISH or QF-PCR analysis results in 2-3 days, full karyotype from cell culture and microarray may
Flashcard 1410361330956
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
amniocentesis
ead><head>Amniocentesis : • Normally 15 to 20 weeks but in special circumstances may be done at any time after 15 weeks • Collection of amniotic fluid transabdominally under ultrasound guidance • Karyotype of fetal cells obtained from amniotic fluid – FISH or QF-PCR analysis results in 2-3 days, full karyotype from cell culture and microarray may be done • Pregnancy loss rate traditionally quoted a
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410364214540
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First prenatal visit
First prenatal visit • Standard records (Ontario Ministry of Health Antenatal Records 1 and 2) • Pregnancy considered in trimesters (three in total, each 12 to 14 weeks in length) • Each pregnancy should be assigned a risk category (see reverse side of AN forms) to ensu
Flashcard 1410365787404
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First prenatal visit
First prenatal visit • Standard records (Ontario Ministry of Health Antenatal Records 1 and 2) • Pregnancy considered in trimesters (three in total, each 12 to 14 weeks in length) • Each pregnancy should be assigned a risk category (see reverse side of AN forms) to ensure appropriate investigations, surveillance and management<
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410368670988
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
antenatal visit history
First Prenatal Visit History 1. History of Present Pregnancy: • LMP: first day of last normal period • Determine EDC (estimated date of confinement) 2. Past Obstetrical History: • All Ob/Gyn histories include a summary of G
Flashcard 1410370243852
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
antenatal visit history
First Prenatal Visit History 1. History of Present Pregnancy: • LMP: first day of last normal period • Determine EDC (estimated date of confinement) 2. Past Obstetrical History: • All Ob/Gyn histories include a summary of G and P • For more complicated patients, can further categorize into GTPAL: G: any pregnancy (include losses, ectopic, mole,
Flashcard 1410371816716
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
antenatal visit history
on, sex, birth weight, gestational age at delivery, mode of delivery (vaginal – assisted or spontaneous; Cesarean – low segment or classical); were there any antepartum, intrapartum or postpartum complications and/or fetal anomalies. 3. <span>Past Medical and Surgical History 4. Family History: genetic diseases, congenital malformations, consanguinity 5. Medications, Allergies 6. Social History: smoking, alcohol, recreational drugs, home
Flashcard 1410373389580
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
antenatal visit history
delivery, mode of delivery (vaginal – assisted or spontaneous; Cesarean – low segment or classical); were there any antepartum, intrapartum or postpartum complications and/or fetal anomalies. 3. Past Medical and Surgical History 4. <span>Family History: genetic diseases, congenital malformations, consanguinity 5. Medications, Allergies 6. Social History: smoking, alcohol, recreational drugs, home environment 7. Re
Flashcard 1410374962444
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
antenatal visit history
t or classical); were there any antepartum, intrapartum or postpartum complications and/or fetal anomalies. 3. Past Medical and Surgical History 4. Family History: genetic diseases, congenital malformations, consanguinity 5. <span>Medications, Allergies 6. Social History: smoking, alcohol, recreational drugs, home environment 7. Review of Systems (tailor to patient)<span><body><html>
Flashcard 1410376535308
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
antenatal visit history
ntepartum, intrapartum or postpartum complications and/or fetal anomalies. 3. Past Medical and Surgical History 4. Family History: genetic diseases, congenital malformations, consanguinity 5. Medications, Allergies 6. <span>Social History: smoking, alcohol, recreational drugs, home environment 7. Review of Systems (tailor to patient)<span><body><html>
Flashcard 1410378108172
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
antenatal visit history
3. Past Medical and Surgical History 4. Family History: genetic diseases, congenital malformations, consanguinity 5. Medications, Allergies 6. Social History: smoking, alcohol, recreational drugs, home environment 7. <span>Review of Systems (tailor to patient)<span><body><html>
Flashcard 1410379681036
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
antenatal visit history
First Prenatal Visit History 1. History of Present Pregnancy: • LMP: first day of last normal period • Determine EDC (estimated date of confinement) 2. Past Obstetrical History: • All Ob/Gyn histories include a summary of G and P • For more complicated patients, c
Flashcard 1410381253900
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
antenatal visit history
First Prenatal Visit History 1. History of Present Pregnancy: • LMP: first day of last normal period • Determine EDC (estimated date of confinement) 2. Past Obstetrical History: • All Ob/Gyn histories include a summary of G and P • For more complicated patients, can further categorize into GTPAL: G: any pregnan
Flashcard 1410382826764
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
antenatal visit history
natal Visit History 1. History of Present Pregnancy: • LMP: first day of last normal period • Determine EDC (estimated date of confinement) 2. Past Obstetrical History: • All Ob/Gyn histories include a summary of <span>G and P • For more complicated patients, can further categorize into GTPAL: G: any pregnancy (include losses, ectopic, mole, current) T: term – infants delivered after 37 complet
Flashcard 1410384399628
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
antenatal visit history
ment) 2. Past Obstetrical History: • All Ob/Gyn histories include a summary of G and P • For more complicated patients, can further categorize into GTPAL: G: any pregnancy (include losses, ectopic, mole, current) T: <span>term – infants delivered after 37 completed weeks P: preterm – infants delivered 20 - 36+6 weeks A: abortions – pregnancy loss prior to 20 weeks and/or fetus weighing <500 grams L: live – number of currently living ch
Flashcard 1410385972492
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
antenatal visit history
n histories include a summary of G and P • For more complicated patients, can further categorize into GTPAL: G: any pregnancy (include losses, ectopic, mole, current) T: term – infants delivered after 37 completed weeks P: <span>preterm – infants delivered 20 - 36+6 weeks A: abortions – pregnancy loss prior to 20 weeks and/or fetus weighing <500 grams L: live – number of currently living children • If pregnancy loss prior to 20 weeks, i
Flashcard 1410387545356
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
antenatal visit history
more complicated patients, can further categorize into GTPAL: G: any pregnancy (include losses, ectopic, mole, current) T: term – infants delivered after 37 completed weeks P: preterm – infants delivered 20 - 36+6 weeks A: <span>abortions – pregnancy loss prior to 20 weeks and/or fetus weighing <500 grams L: live – number of currently living children • If pregnancy loss prior to 20 weeks, inquire: ---• how did loss happen (did they have a termination? or bleed and cramp? d
Flashcard 1410389118220
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
antenatal visit history
ude losses, ectopic, mole, current) T: term – infants delivered after 37 completed weeks P: preterm – infants delivered 20 - 36+6 weeks A: abortions – pregnancy loss prior to 20 weeks and/or fetus weighing <500 grams L: <span>live – number of currently living children • If pregnancy loss prior to 20 weeks, inquire: ---• how did loss happen (did they have a termination? or bleed and cramp? did they feels pressure and have PPROM?) - different
Flashcard 1410390691084
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
antenatal visit history
ed 20 - 36+6 weeks A: abortions – pregnancy loss prior to 20 weeks and/or fetus weighing <500 grams L: live – number of currently living children • If pregnancy loss prior to 20 weeks, inquire: ---• how did loss happen (<span>did they have a termination? or bleed and cramp? did they feels pressure and have PPROM?) - differentiate between causes such as therapeutic abortion, spontaneous abortion, fetal anomaly, maternal issues (incompetent cervix) ---• was a surgical procedure required such
Flashcard 1410392263948
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
antenatal visit history
of currently living children • If pregnancy loss prior to 20 weeks, inquire: ---• how did loss happen (did they have a termination? or bleed and cramp? did they feels pressure and have PPROM?) - differentiate between causes such as <span>therapeutic abortion, spontaneous abortion, fetal anomaly, maternal issues (incompetent cervix) ---• was a surgical procedure required such as a D and C (Dilatation and Curettage) or D and E (Dilatation and Evacuation) ---• was medical intervention required such as misop
Flashcard 1410393836812
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
antenatal visit history
d and cramp? did they feels pressure and have PPROM?) - differentiate between causes such as therapeutic abortion, spontaneous abortion, fetal anomaly, maternal issues (incompetent cervix) ---• was a surgical procedure required such as a <span>D and C (Dilatation and Curettage) or D and E (Dilatation and Evacuation) ---• was medical intervention required such as misoprostol (for missed abortion or blighted ovum) • If pregnancy loss after 20 weeks, inquire: ---• date of delivery, loca
Flashcard 1410395409676
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
antenatal visit history
abortion, fetal anomaly, maternal issues (incompetent cervix) ---• was a surgical procedure required such as a D and C (Dilatation and Curettage) or D and E (Dilatation and Evacuation) ---• was medical intervention required such as <span>misoprostol (for missed abortion or blighted ovum) • If pregnancy loss after 20 weeks, inquire: ---• date of delivery, location, sex, birth weight, gestational age at delivery, mode of delivery (vaginal – assisted or spontaneo
Flashcard 1410396982540
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
antenatal visit history
as a D and C (Dilatation and Curettage) or D and E (Dilatation and Evacuation) ---• was medical intervention required such as misoprostol (for missed abortion or blighted ovum) • If pregnancy loss after 20 weeks, inquire: ---• <span>date of delivery, location, sex, birth weight, gestational age at delivery, mode of delivery (vaginal – assisted or spontaneous; Cesarean – low segment or classical); were there any antepartum, intrapartum or postpartum complications and/or fetal anomalies. 3. Past Medical and Surgical History 4. Family History: genetic diseases, congeni
Flashcard 1410398555404
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
antenatal visit history
• If pregnancy loss after 20 weeks, inquire: ---• date of delivery, location, sex, birth weight, gestational age at delivery, mode of delivery (vaginal – assisted or spontaneous; Cesarean – low segment or classical); were there any <span>antepartum, intrapartum or postpartum complications and/or fetal anomalies. 3. Past Medical and Surgical History 4. Family History: genetic diseases, congenital malformations, consanguinity 5. Medications, Allergies 6. Social History:
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410431061260
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410432634124
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410434206988
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410435779852
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410471169292
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First Prenatal Visit Physical Exam
First Prenatal Visit Physical Examination 1. General : Vital signs, Weight (calculate BMI) 2. Head and Neck : • thyroid exam • chloasma • gums/mucous membranes: hyperemic/swollen; epulis of pregnancy 3. Chest : • consider anatomic and physiolog
Flashcard 1410472742156
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First Prenatal Visit Physical Exam
First Prenatal Visit Physical Examination 1. General : Vital signs, Weight (calculate BMI) 2. Head and Neck : • thyroid exam • chloasma • gums/mucous membranes: hyperemic/swollen; epulis of pregnancy 3. Chest : • consider anatomic and physiologic effects of pregnancy • elevated
Flashcard 1410474315020
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First Prenatal Visit Physical Exam
First Prenatal Visit Physical Examination 1. General : Vital signs, Weight (calculate BMI) 2. Head and Neck : • thyroid exam • chloasma • gums/mucous membranes: hyperemic/swollen; epulis of pregnancy 3. Chest : • consider anatomic and physiologic effects of pregnancy • elevated diaphragm 4. He
Flashcard 1410475887884
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First Prenatal Visit Physical Exam
t (calculate BMI) 2. Head and Neck : • thyroid exam • chloasma • gums/mucous membranes: hyperemic/swollen; epulis of pregnancy 3. Chest : • consider anatomic and physiologic effects of pregnancy • elevated <span>diaphragm 4. Heart : • increased heart rate • murmurs: flow versus possible pathologic • if murmur is pathologic, consider maternal tolerance of pregnancy, echocardiogram, ne
Flashcard 1410477460748
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First Prenatal Visit Physical Exam
First Prenatal Visit Physical Examination 1. General : Vital signs, Weight (calculate BMI) 2. Head and Neck : • thyroid exam • chloasma • gums/mucous membranes: hyperemic/swollen; epulis of pregnancy 3. Chest : • consider anatomic and physiologic effects of pregnancy • elevated diaphragm 4. Heart : • increased heart rate • murmurs: flow versus possibl
Flashcard 1410479820044
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First Prenatal Visit Physical Exam
Vital signs, Weight (calculate BMI) 2. Head and Neck : • thyroid exam • chloasma • gums/mucous membranes: hyperemic/swollen; epulis of pregnancy 3. Chest : • elevated diaphragm 4. Heart : • increased <span>heart rate • murmurs: flow versus possible pathologic 5. Breast : • leakage • physiologic changes 6. Abdomen : • striae • linea nigra • rectus diastasis&#
Flashcard 1410481392908
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First Prenatal Visit Physical Exam
; • chloasma • gums/mucous membranes: hyperemic/swollen; epulis of pregnancy 3. Chest : • elevated diaphragm 4. Heart : • increased heart rate • murmurs: flow versus possible pathologic 5. Breast : • <span>leakage • physiologic changes 6. Abdomen : • striae • linea nigra • rectus diastasis • uterus 7. Pelvic Examination : • External Genitalia Inspection:&
Flashcard 1410482965772
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First Prenatal Visit Physical Exam
epulis of pregnancy 3. Chest : • elevated diaphragm 4. Heart : • increased heart rate • murmurs: flow versus possible pathologic 5. Breast : • leakage • physiologic changes 6. Abdomen : • <span>striae • linea nigra • rectus diastasis • uterus 7. Pelvic Examination : • External Genitalia Inspection: ---• lesions: condyloma, ulcers, varicosities ---•
Flashcard 1410484538636
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First Prenatal Visit Physical Exam
gnancy 3. Chest : • elevated diaphragm 4. Heart : • increased heart rate • murmurs: flow versus possible pathologic 5. Breast : • leakage • physiologic changes 6. Abdomen : • striae • <span>linea nigra • rectus diastasis • uterus 7. Pelvic Examination : • External Genitalia Inspection: ---• lesions: condyloma, ulcers, varicosities ---• previous surgeries
Flashcard 1410486111500
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First Prenatal Visit Physical Exam
st : • elevated diaphragm 4. Heart : • increased heart rate • murmurs: flow versus possible pathologic 5. Breast : • leakage • physiologic changes 6. Abdomen : • striae • linea nigra • <span>rectus diastasis • uterus 7. Pelvic Examination : • External Genitalia Inspection: ---• lesions: condyloma, ulcers, varicosities ---• previous surgeries: female genital mutilat
Flashcard 1410487684364
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First Prenatal Visit Physical Exam
; • External Genitalia Inspection: ---• lesions: condyloma, ulcers, varicosities ---• previous surgeries: female genital mutilation • Internal Genitalia: ---• Speculum Exam • Inspection: ---• Vagina: ------• <span>Chadwick’s sign (bluish discoloration) ------• vaginitis (yeast is common) ---• Cervix: ------• Ectropion ------• Polyps • Cultures: ---• Chlamydial culture is take
Flashcard 1410489257228
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First Prenatal Visit Physical Exam
: condyloma, ulcers, varicosities ---• previous surgeries: female genital mutilation • Internal Genitalia: ---• Speculum Exam • Inspection: ---• Vagina: ------• Chadwick’s sign (bluish discoloration) ------• <span>vaginitis (yeast is common) ---• Cervix: ------• Ectropion ------• Polyps • Cultures: ---• Chlamydial culture is taken from just inside the external os ---• Gonorr
Flashcard 1410490830092
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First Prenatal Visit Physical Exam
, ulcers, varicosities ---• previous surgeries: female genital mutilation • Internal Genitalia: ---• Speculum Exam • Inspection: ---• Vagina: ------• Chadwick’s sign (bluish discoloration) ------• vaginitis (<span>yeast is common) ---• Cervix: ------• Ectropion ------• Polyps • Cultures: ---• Chlamydial culture is taken from just inside the external os ---• Gonorrheal cu
Flashcard 1410492402956
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First Prenatal Visit Physical Exam
ies: female genital mutilation • Internal Genitalia: ---• Speculum Exam • Inspection: ---• Vagina: ------• Chadwick’s sign (bluish discoloration) ------• vaginitis (yeast is common) ---• Cervix: ------• <span>Ectropion ------• Polyps • Cultures: ---• Chlamydial culture is taken from just inside the external os ---• Gonorrheal culture from os/cervix • Pap: ---• Do not us
Flashcard 1410493975820
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First Prenatal Visit Physical Exam
ilation • Internal Genitalia: ---• Speculum Exam • Inspection: ---• Vagina: ------• Chadwick’s sign (bluish discoloration) ------• vaginitis (yeast is common) ---• Cervix: ------• Ectropion ------• <span>Polyps • Cultures: ---• Chlamydial culture is taken from just inside the external os ---• Gonorrheal culture from os/cervix • Pap: ---• Do not use intracervical brus
Flashcard 1410497121548
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First Prenatal Visit Physical Exam
h discoloration) ------• vaginitis (yeast is common) ---• Cervix: ------• Ectropion ------• Polyps • Cultures: ---• Chlamydial culture is taken from just inside the external os ---• Gonorrheal culture from <span>os/cervix • Pap: ---• Do not use intracervical brush during pregnancy - spatula or external brush only • The cervix is often friable during pregnancy and may bleed from Pap - reass
Flashcard 1410498694412
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First Prenatal Visit Physical Exam
ast is common) ---• Cervix: ------• Ectropion ------• Polyps • Cultures: ---• Chlamydial culture is taken from just inside the external os ---• Gonorrheal culture from os/cervix • Pap: ---• Do not use <span>intracervical brush during pregnancy - spatula or external brush only • The cervix is often friable during pregnancy and may bleed from Pap - reassure patient that you are nowhere near the pregn
Flashcard 1410500267276
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First Prenatal Visit Physical Exam
e cervix is often friable during pregnancy and may bleed from Pap - reassure patient that you are nowhere near the pregnancy and that spotting is normal after a Pap smear in pregnancy • Bimanual Examination: ---• largely replaced by <span>first trimester ultrasound. ---• Cervix: Hegar’s sign (softening) • Uterus ---• size (ensure it is consistent with dates) ---• shape (expect it to be symmetrically enlarged) ---• consiste
Flashcard 1410501840140
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First Prenatal Visit Physical Exam
may bleed from Pap - reassure patient that you are nowhere near the pregnancy and that spotting is normal after a Pap smear in pregnancy • Bimanual Examination: ---• largely replaced by first trimester ultrasound. ---• Cervix: <span>Hegar’s sign (softening) • Uterus ---• size (ensure it is consistent with dates) ---• shape (expect it to be symmetrically enlarged) ---• consistency (expect soft) ---•
Flashcard 1410503413004
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First Prenatal Visit Physical Exam
m Pap - reassure patient that you are nowhere near the pregnancy and that spotting is normal after a Pap smear in pregnancy • Bimanual Examination: ---• largely replaced by first trimester ultrasound. ---• Cervix: Hegar’s sign (<span>softening) • Uterus ---• size (ensure it is consistent with dates) ---• shape (expect it to be symmetrically enlarged) ---• consistency (expect soft) ---• if the uterus i
Flashcard 1410504985868
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First Prenatal Visit Physical Exam
pregnancy and that spotting is normal after a Pap smear in pregnancy • Bimanual Examination: ---• largely replaced by first trimester ultrasound. ---• Cervix: Hegar’s sign (softening) • Uterus ---• size (ensure it is <span>consistent with dates) ---• shape (expect it to be symmetrically enlarged) ---• consistency (expect soft) ---• if the uterus is firm, smaller than expected, irregularly enlarged, then reconsid
Flashcard 1410506558732
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First Prenatal Visit Physical Exam
in pregnancy • Bimanual Examination: ---• largely replaced by first trimester ultrasound. ---• Cervix: Hegar’s sign (softening) • Uterus ---• size (ensure it is consistent with dates) ---• shape (expect it to be <span>symmetrically enlarged) ---• consistency (expect soft) ---• if the uterus is firm, smaller than expected, irregularly enlarged, then reconsider dates, viability, uterine anomaly, ectopic pr
Flashcard 1410508131596
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First Prenatal Visit Physical Exam
argely replaced by first trimester ultrasound. ---• Cervix: Hegar’s sign (softening) • Uterus ---• size (ensure it is consistent with dates) ---• shape (expect it to be symmetrically enlarged) ---• consistency (expect <span>soft) ---• if the uterus is firm, smaller than expected, irregularly enlarged, then reconsider dates, viability, uterine anomaly, ectopic pregnancy • Adnexa: masses, their size, s
Flashcard 1410509704460
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First Prenatal Visit Physical Exam
r ultrasound. ---• Cervix: Hegar’s sign (softening) • Uterus ---• size (ensure it is consistent with dates) ---• shape (expect it to be symmetrically enlarged) ---• consistency (expect soft) ---• if the uterus is <span>firm, smaller than expected, irregularly enlarged, then reconsider dates, viability, uterine anomaly, ectopic pregnancy • Adnexa: masses, their size, shape, consistency, mobility, tenderness • Bony pelvis (clinical pelvimetr
Flashcard 1410511277324
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First Prenatal Visit Physical Exam
rus ---• size (ensure it is consistent with dates) ---• shape (expect it to be symmetrically enlarged) ---• consistency (expect soft) ---• if the uterus is firm, smaller than expected, irregularly enlarged, then reconsider <span>dates, viability, uterine anomaly, ectopic pregnancy • Adnexa: masses, their size, shape, consistency, mobility, tenderness • Bony pelvis (clinical pelvimetry to assess adequacy of pelvis for labour): ---• Type of pelvis:&
Flashcard 1410512850188
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First Prenatal Visit Physical Exam
pe (expect it to be symmetrically enlarged) ---• consistency (expect soft) ---• if the uterus is firm, smaller than expected, irregularly enlarged, then reconsider dates, viability, uterine anomaly, ectopic pregnancy • Adnexa: <span>masses, their size, shape, consistency, mobility, tenderness • Bony pelvis (clinical pelvimetry to assess adequacy of pelvis for labour): ---• Type of pelvis: ------• gynecoid ------• android ------• anthropoid -----
Flashcard 1410515209484
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
First Prenatal Visit Physical Exam
he uterus is firm, smaller than expected, irregularly enlarged, then reconsider dates, viability, uterine anomaly, ectopic pregnancy • Adnexa: masses, their size, shape, consistency, mobility, tenderness 8. Extremities : check for <span>edema and varicosities<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410519403788
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
follow up antenatal visits - hx
Follow-up Antenatal Visits History: • General well-being • Specific concerns • New developments • Fetal activity
Flashcard 1410520976652
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
follow up antenatal visits - hx
Follow-up Antenatal Visits History: • General well-being • Specific concerns • New developments • Fetal activity
Flashcard 1410524122380
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
follow up antenatal visits - hx
Follow-up Antenatal Visits History: • General well-being • Specific concerns • New developments • Fetal activity
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410527005964
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
follow up antenatal visits - p/e
Follow-up Antenatal Visits Physical: • Weight • Blood pressure • Uterine size (symphysis-fundal height, is it compatible with dates, enlarging appropriately) • Auscultate fetal heart (audible with handheld doppler or
Flashcard 1410528578828
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
follow up antenatal visits - p/e
Follow-up Antenatal Visits Physical: • Weight • Blood pressure • Uterine size (symphysis-fundal height, is it compatible with dates, enlarging appropriately) • Auscultate fetal heart (audible with handheld doppler or “doptone” from early
Flashcard 1410530151692
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
follow up antenatal visits - p/e
Follow-up Antenatal Visits Physical: • Weight • Blood pressure • Uterine size (symphysis-fundal height, is it compatible with dates, enlarging appropriately) • Auscultate fetal heart (audible with handheld doppler or “doptone” from early T2 (~15-16 week
Flashcard 1410531724556
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
follow up antenatal visits - p/e
Follow-up Antenatal Visits Physical: • Weight • Blood pressure • Uterine size (symphysis-fundal height, is it compatible with dates, enlarging appropriately) • Auscultate fetal heart (audible with handheld doppler or “doptone” from early T2 (~15-16 weeks) • After 30-32 w
Flashcard 1410533297420
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
follow up antenatal visits - p/e
Follow-up Antenatal Visits Physical: • Weight • Blood pressure • Uterine size (symphysis-fundal height, is it compatible with dates, enlarging appropriately) • Auscultate fetal heart (audible with handheld doppler or “doptone” from early T2 (~15-16 weeks) • After 30-32 weeks - Leopold’s maneuvers: ---• Presentation ---• Lie ---• Location of small
Flashcard 1410534870284
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
follow up antenatal visits - p/e
atal Visits Physical: • Weight • Blood pressure • Uterine size (symphysis-fundal height, is it compatible with dates, enlarging appropriately) • Auscultate fetal heart (audible with handheld doppler or “doptone” from early <span>T2 (~15-16 weeks) • After 30-32 weeks - Leopold’s maneuvers: ---• Presentation ---• Lie ---• Location of small fetal parts ---• Presence of engagement (in late T3 primigra
Flashcard 1410536443148
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
follow up antenatal visits - p/e
ight • Blood pressure • Uterine size (symphysis-fundal height, is it compatible with dates, enlarging appropriately) • Auscultate fetal heart (audible with handheld doppler or “doptone” from early T2 (~15-16 weeks) • After <span>30-32 weeks - Leopold’s maneuvers: ---• Presentation ---• Lie ---• Location of small fetal parts ---• Presence of engagement (in late T3 primigravidas)<span></body
Flashcard 1410538016012
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
follow up antenatal visits - p/e
ood pressure • Uterine size (symphysis-fundal height, is it compatible with dates, enlarging appropriately) • Auscultate fetal heart (audible with handheld doppler or “doptone” from early T2 (~15-16 weeks) • After 30-32 weeks - <span>Leopold’s maneuvers: ---• Presentation ---• Lie ---• Location of small fetal parts ---• Presence of engagement (in late T3 primigravidas)<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410545093900
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
follow up antenatal visits - labs
Follow up Antenatal Visits Lab: • Urinalysis by dip stick if elevated BP • Proteinuria may indicate the presence of gestational hypertension with proteinuria. May also be seen in UTIs or renal disease. Trace to 1+ protein fairly commonly seen and needs
Flashcard 1410546666764
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
follow up antenatal visits - labs
Follow up Antenatal Visits Lab: • Urinalysis by dip stick if elevated BP • Proteinuria may indicate the presence of gestational hypertension with proteinuria. May also be seen in UTIs or renal disease. Trace to 1+ protein fairly commonly seen and needs to be judged in clinical context.
Flashcard 1410548239628
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
follow up antenatal visits - labs
Follow up Antenatal Visits Lab: • Urinalysis by dip stick if elevated BP • Proteinuria may indicate the presence of gestational hypertension with proteinuria. May also be seen in UTIs or renal disease. Trace to 1+ protein fairly commonly seen and needs to be judged in clinical context.
Flashcard 1410549812492
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
follow up antenatal visits - labs
Follow up Antenatal Visits Lab: • Urinalysis by dip stick if elevated BP • Proteinuria may indicate the presence of gestational hypertension with proteinuria. May also be seen in UTIs or renal disease. Trace to 1+ protein fairly commonly seen and needs to be judged in clinical context.<html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410552696076
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - GI
Physiologic Changes of pregnancy - Gastro-intestinal: • Progesterone acts as a smooth muscle relaxant resulting in: ---• Constipation from decreased GI motility ---• Reflux due to decreased GE sphincter tone, delayed gastric emptying and increased intra-abdominal pressure
Flashcard 1410554268940
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - GI
Physiologic Changes of pregnancy - Gastro-intestinal: • Progesterone acts as a smooth muscle relaxant resulting in: ---• Constipation from decreased GI motility ---• Reflux due to decreased GE sphincter tone, delayed gastric emptying and increased intra-abdominal pressure ---• Gallbladder stasis
Flashcard 1410555841804
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - GI
Physiologic Changes of pregnancy - Gastro-intestinal: • Progesterone acts as a smooth muscle relaxant resulting in: ---• Constipation from decreased GI motility ---• Reflux due to decreased GE sphincter tone, delayed gastric emptying and increased intra-abdominal pressure ---• Gallbladder stasis
Flashcard 1410557414668
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - GI
13; • Progesterone acts as a smooth muscle relaxant resulting in: ---• Constipation from decreased GI motility ---• Reflux due to decreased GE sphincter tone, delayed gastric emptying and increased intra-abdominal pressure ---• <span>Gallbladder stasis<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410560298252
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - skin
Physiologic Changes of pregnancy - Skin: • Pigment changes: darkening of areola, linea nigra, chloasma • Spider nevi • Palmar erythema • Changes in moles • Proliferation of skin tags
Flashcard 1410561871116
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - skin
Physiologic Changes of pregnancy - Skin: • Pigment changes: darkening of areola, linea nigra, chloasma • Spider nevi • Palmar erythema • Changes in moles • Proliferation of skin tags
Flashcard 1410563443980
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - skin
Physiologic Changes of pregnancy - Skin: • Pigment changes: darkening of areola, linea nigra, chloasma • Spider nevi • Palmar erythema • Changes in moles • Proliferation of skin tags
Flashcard 1410565016844
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - skin
Physiologic Changes of pregnancy - Skin: • Pigment changes: darkening of areola, linea nigra, chloasma • Spider nevi • Palmar erythema • Changes in moles • Proliferation of skin tags
Flashcard 1410566589708
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - skin
Physiologic Changes of pregnancy - Skin: • Pigment changes: darkening of areola, linea nigra, chloasma • Spider nevi • Palmar erythema • Changes in moles • Proliferation of skin tags
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410569473292
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - hematologic
Physiologic Changes of pregnancy - Hematologic: • ↑ plasma volume • ↑ red blood cell mass (less than plasma resulting in an apparent decrease in Hb and HCT) • ↑ WBC count • ↑ most coagulation proteins (fibrinogen, not factor XIII
Flashcard 1410571046156
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - hematologic
Physiologic Changes of pregnancy - Hematologic: • ↑ plasma volume • ↑ red blood cell mass (less than plasma resulting in an apparent decrease in Hb and HCT) • ↑ WBC count • ↑ most coagulation proteins (fibrinogen, not factor XIII); important with respect to de
Flashcard 1410572619020
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - hematologic
Physiologic Changes of pregnancy - Hematologic: • ↑ plasma volume • ↑ red blood cell mass (less than plasma resulting in an apparent decrease in Hb and HCT) • ↑ WBC count • ↑ most coagulation proteins (fibrinogen, not factor XIII); important with respect to development of DVT • ↑ transport proteins leading to increase in the
Flashcard 1410574191884
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - hematologic
Physiologic Changes of pregnancy - Hematologic: • ↑ plasma volume • ↑ red blood cell mass (less than plasma resulting in an apparent decrease in Hb and HCT) • ↑ WBC count • ↑ most coagulation proteins (fibrinogen, not factor XIII); important with respect to development of DVT • ↑ transport proteins leading to increase in the total levels
Flashcard 1410575764748
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - hematologic
Physiologic Changes of pregnancy - Hematologic: • ↑ plasma volume • ↑ red blood cell mass (less than plasma resulting in an apparent decrease in Hb and HCT) • ↑ WBC count • ↑ most coagulation proteins (fibrinogen, not factor XIII); important with respect to development of DVT • ↑ transport proteins leading to increase in the total levels of those hormones and minerals t
Flashcard 1410577337612
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - hematologic
3; • ↑ plasma volume • ↑ red blood cell mass (less than plasma resulting in an apparent decrease in Hb and HCT) • ↑ WBC count • ↑ most coagulation proteins (fibrinogen, not factor XIII); important with respect to development of <span>DVT • ↑ transport proteins leading to increase in the total levels of those hormones and minerals they bind • ↓ total protein (largely dilutional) • ↓ serum albumin</s
Flashcard 1410578910476
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - hematologic
volume • ↑ red blood cell mass (less than plasma resulting in an apparent decrease in Hb and HCT) • ↑ WBC count • ↑ most coagulation proteins (fibrinogen, not factor XIII); important with respect to development of DVT • ↑ <span>transport proteins leading to increase in the total levels of those hormones and minerals they bind • ↓ total protein (largely dilutional) • ↓ serum albumin<span><body><html>
Flashcard 1410580483340
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - hematologic
C count • ↑ most coagulation proteins (fibrinogen, not factor XIII); important with respect to development of DVT • ↑ transport proteins leading to increase in the total levels of those hormones and minerals they bind • ↓ total <span>protein (largely dilutional) • ↓ serum albumin<span><body><html>
Flashcard 1410582056204
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - hematologic
fibrinogen, not factor XIII); important with respect to development of DVT • ↑ transport proteins leading to increase in the total levels of those hormones and minerals they bind • ↓ total protein (largely dilutional) • ↓ serum <span>albumin<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410584939788
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - renal
Physiologic Changes of pregnancy - Renal: • Slight decrease in BUN and Creatinine • ↑ renal blood flow (RBF) • ↑ GFR • Anatomic changes related to the effects of progesterone lead to dilatation of the ureters and renal pelvis (R>L) • Glycosuria
Flashcard 1410586512652
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - renal
Physiologic Changes of pregnancy - Renal: • Slight decrease in BUN and Creatinine • ↑ renal blood flow (RBF) • ↑ GFR • Anatomic changes related to the effects of progesterone lead to dilatation of the ureters and renal pelvis (R>L) • Glycosuria may be the result of these chan
Flashcard 1410588085516
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - renal
Physiologic Changes of pregnancy - Renal: • Slight decrease in BUN and Creatinine • ↑ renal blood flow (RBF) • ↑ GFR • Anatomic changes related to the effects of progesterone lead to dilatation of the ureters and renal pelvis (R>L) • Glycosuria may be the result of these changes as the RB
Flashcard 1410589658380
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - renal
ead>Physiologic Changes of pregnancy - Renal: • Slight decrease in BUN and Creatinine • ↑ renal blood flow (RBF) • ↑ GFR • Anatomic changes related to the effects of progesterone lead to dilatation of the ureters and renal pelvis (R>L) • Glycosuria may be the result of these changes as the RBF increase exceeds that of the GFR preventing reabsorption as per the non-pregnant state • Diagnosis of gesta
Flashcard 1410591231244
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - renal
of pregnancy - Renal: • Slight decrease in BUN and Creatinine • ↑ renal blood flow (RBF) • ↑ GFR • Anatomic changes related to the effects of progesterone lead to dilatation of the ureters and renal pelvis (R>L) • <span>Glycosuria may be the result of these changes as the RBF increase exceeds that of the GFR preventing reabsorption as per the non-pregnant state • Diagnosis of gestational diabetes mellitus sh
Flashcard 1410592804108
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - renal
13; • Glycosuria may be the result of these changes as the RBF increase exceeds that of the GFR preventing reabsorption as per the non-pregnant state • Diagnosis of gestational diabetes mellitus should be made from blood studies not from <span>glycosuria<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410595687692
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - CV
Physiologic Changes of pregnancy - Cardiovascular: • ↑ cardiac output • ↑ heart rate • ↑ blood volume • ↓ BP due to decreased total peripheral resistance from the progesterone effect on vascular smooth muscle • ↓ venous return due to:&
Flashcard 1410597260556
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - CV
Physiologic Changes of pregnancy - Cardiovascular: • ↑ cardiac output • ↑ heart rate • ↑ blood volume • ↓ BP due to decreased total peripheral resistance from the progesterone effect on vascular smooth muscle • ↓ venous return due to: ---• large uter
Flashcard 1410598833420
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - CV
Physiologic Changes of pregnancy - Cardiovascular: • ↑ cardiac output • ↑ heart rate • ↑ blood volume • ↓ BP due to decreased total peripheral resistance from the progesterone effect on vascular smooth muscle • ↓ venous return due to: ---• large uterus compressing the inf
Flashcard 1410600406284
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - CV
Physiologic Changes of pregnancy - Cardiovascular: • ↑ cardiac output • ↑ heart rate • ↑ blood volume • ↓ BP due to decreased total peripheral resistance from the progesterone effect on vascular smooth muscle • ↓ venous return due to: ---• large uterus compressing the inferior vena c
Flashcard 1410601979148
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - CV
Physiologic Changes of pregnancy - Cardiovascular: • ↑ cardiac output • ↑ heart rate • ↑ blood volume • ↓ BP due to decreased total peripheral resistance from the progesterone effect on vascular smooth muscle • ↓ venous return due to: ---• large uterus compressing the inferior vena cava ---• (supine) hypotension ---• Venous distention caus
Flashcard 1410603552012
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - CV
nancy - Cardiovascular: • ↑ cardiac output • ↑ heart rate • ↑ blood volume • ↓ BP due to decreased total peripheral resistance from the progesterone effect on vascular smooth muscle • ↓ venous return due to: ---• <span>large uterus compressing the inferior vena cava ---• (supine) hypotension ---• Venous distention causing lower extremity edema, varicosities, hemorrhoids and vulvar varicosities</sp
Flashcard 1410605124876
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - CV
• ↑ blood volume • ↓ BP due to decreased total peripheral resistance from the progesterone effect on vascular smooth muscle • ↓ venous return due to: ---• large uterus compressing the inferior vena cava ---• (supine) <span>hypotension ---• Venous distention causing lower extremity edema, varicosities, hemorrhoids and vulvar varicosities<span><body><html>
Flashcard 1410606697740
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - CV
sed total peripheral resistance from the progesterone effect on vascular smooth muscle • ↓ venous return due to: ---• large uterus compressing the inferior vena cava ---• (supine) hypotension ---• Venous distention causing <span>lower extremity edema, varicosities, hemorrhoids and vulvar varicosities<span><body><html>
Flashcard 1410608270604
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Physiologic Changes of pregnancy - CV
• ↓ BP due to decreased total peripheral resistance from the progesterone effect on vascular smooth muscle • ↓ venous return due to: ---• large uterus compressing the inferior vena cava ---• (supine) hypotension ---• <span>Venous distention causing lower extremity edema, varicosities, hemorrhoids and vulvar varicosities<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410611154188
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Endocrine: • ↑ size of thyroid gland • ↑ basal metabolic rate • ↑ total thyroid hormone (secondary to increased thyroid binding globulin) • free T4 and TSH as per non-pregnant state • ↑ total and
Flashcard 1410612727052
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Endocrine: • ↑ size of thyroid gland • ↑ basal metabolic rate • ↑ total thyroid hormone (secondary to increased thyroid binding globulin) • free T4 and TSH as per non-pregnant state • ↑ total and free cortisol • ↓ total ca
Flashcard 1410614299916
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Endocrine: • ↑ size of thyroid gland • ↑ basal metabolic rate • ↑ total thyroid hormone (secondary to increased thyroid binding globulin) • free T4 and TSH as per non-pregnant state • ↑ total and free cortisol • ↓ total calcium secondary to decreased serum a
Flashcard 1410616659212
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Endocrine: • ↑ size of thyroid gland • ↑ basal metabolic rate • ↑ total thyroid hormone (secondary to increased thyroid binding globulin) • ↑ total and free cortisol • ↓ total calcium secondary to decreased serum albumin • ↑ PTH: ---• increased bone resorption ---• increased gut absorption ---• unchanged free calcium •
Flashcard 1410618232076
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Endocrine: • ↑ size of thyroid gland • ↑ basal metabolic rate • ↑ total thyroid hormone (secondary to increased thyroid binding globulin) • ↑ total and free cortisol • ↓ total calcium secondary to decreased serum albumin • ↑ PTH: ---• increased bone resorption ---• increased gut absorption ---• unchanged free calcium • Increased bone turnover
Flashcard 1410619804940
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
span>Endocrine: • ↑ size of thyroid gland • ↑ basal metabolic rate • ↑ total thyroid hormone (secondary to increased thyroid binding globulin) • ↑ total and free cortisol • ↓ total calcium secondary to decreased serum albumin • ↑ PTH: ---• increased bone resorption ---• increased gut absorption ---• unchanged free calcium • Increased bone turnover with no loss of density due to estro
Flashcard 1410621377804
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
land • ↑ basal metabolic rate • ↑ total thyroid hormone (secondary to increased thyroid binding globulin) • ↑ total and free cortisol • ↓ total calcium secondary to decreased serum albumin • ↑ PTH: ---• increased <span>bone resorption ---• increased gut absorption ---• unchanged free calcium • Increased bone turnover with no loss of density due to estrogen’s inhibition of resorption • Diabetogenic
Flashcard 1410622950668
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
13; • ↑ total thyroid hormone (secondary to increased thyroid binding globulin) • ↑ total and free cortisol • ↓ total calcium secondary to decreased serum albumin • ↑ PTH: ---• increased bone resorption ---• increased <span>gut absorption ---• unchanged free calcium • Increased bone turnover with no loss of density due to estrogen’s inhibition of resorption • Diabetogenic tendencies: increased serum cortis
Flashcard 1410624523532
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
ol • ↓ total calcium secondary to decreased serum albumin • ↑ PTH: ---• increased bone resorption ---• increased gut absorption ---• unchanged free calcium • Increased bone turnover with no loss of density due to <span>estrogen’s inhibition of resorption • Diabetogenic tendencies: increased serum cortisol and increased insulin resistance<span><body><html>
Flashcard 1410626096396
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
13; ---• increased bone resorption ---• increased gut absorption ---• unchanged free calcium • Increased bone turnover with no loss of density due to estrogen’s inhibition of resorption • Diabetogenic tendencies: increased <span>serum cortisol and increased insulin resistance<span><body><html>
Flashcard 1410627669260
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
ption ---• increased gut absorption ---• unchanged free calcium • Increased bone turnover with no loss of density due to estrogen’s inhibition of resorption • Diabetogenic tendencies: increased serum cortisol and increased <span>insulin resistance<span><body><html>

| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410634747148
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Pharm Management of NVP
-remember to r/o other causes of N&V -weigh frequently, assess lvl of hydration, test urine for ketones -pharm management: diclectin (doxylamine/pyridoxine) is standard of care, 2-4 tabs daily but can incre
Flashcard 1410636320012
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Pharm Management of NVP
-remember to r/o other causes of N&V -weigh frequently, assess lvl of hydration, test urine for ketones -pharm management: diclectin (doxylamine/pyridoxine) is standard of care, 2-4 tabs daily but can increase to 8</sp
Flashcard 1410637892876
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Pharm Management of NVP
-remember to r/o other causes of N&V -weigh frequently, assess lvl of hydration, test urine for ketones -pharm management: diclectin (doxylamine/pyridoxine) is standard of care, 2-4 tabs daily but can increase to 8
Flashcard 1410639465740
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Pharm Management of NVP
-remember to r/o other causes of N&V -weigh frequently, assess lvl of hydration, test urine for ketones -pharm management: diclectin (doxylamine/pyridoxine) is standard of care, 2-4 tabs daily but can increase to 8
Flashcard 1410641038604
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Pharm Management of NVP
-remember to r/o other causes of N&V -weigh frequently, assess lvl of hydration, test urine for ketones -pharm management: diclectin (doxylamine/pyridoxine) is standard of care, 2-4 tabs daily but can increase to 8
Flashcard 1410642611468
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Pharm Management of NVP
pan>-remember to r/o other causes of N&V -weigh frequently, assess lvl of hydration, test urine for ketones -pharm management: diclectin (doxylamine/pyridoxine) is standard of care, 2-4 tabs daily but can increase to 8<span><body><html>
Flashcard 1410644184332

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410648378636

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410652572940

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410657553676

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410661747980

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410665942284

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410695826700

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410725973260
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Nutrition in pregnancy
Nutrition in pregnancy: • Prenatal vitamin (PNV) supplementation recommended (Materna, PregVit) • Supplementation not always essential as long as the diet is meeting calcium, iron and folic acid needs • Appropriate intake is
Flashcard 1410727546124
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Nutrition in pregnancy
Nutrition in pregnancy: • Prenatal vitamin (PNV) supplementation recommended (Materna, PregVit) • Supplementation not always essential as long as the diet is meeting calcium, iron and folic acid needs • Appropriate intake is recommended (not necessary to “eat for two”)&
Flashcard 1410729118988
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Nutrition in pregnancy
Nutrition in pregnancy: • Prenatal vitamin (PNV) supplementation recommended (Materna, PregVit) • Supplementation not always essential as long as the diet is meeting calcium, iron and folic acid needs • Appropriate intake is recommended (not necessary to “eat for two”) Canada’s Food Guide suggests the following: • 3 to 4 servings of milk per day • Increase
Flashcard 1410730691852
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Nutrition in pregnancy
• Supplementation not always essential as long as the diet is meeting calcium, iron and folic acid needs • Appropriate intake is recommended (not necessary to “eat for two”) Canada’s Food Guide suggests the following: • <span>3 to 4 servings of milk per day • Increase intake by 100kCal per day in first trimester, 300 kCal/day in second and third trimester and by 450kCal/day when lactating • Well rounded,
Flashcard 1410732264716
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Nutrition in pregnancy
e diet is meeting calcium, iron and folic acid needs • Appropriate intake is recommended (not necessary to “eat for two”) Canada’s Food Guide suggests the following: • 3 to 4 servings of milk per day • Increase intake by <span>100kCal per day in first trimester, 300 kCal/day in second and third trimester and by 450kCal/day when lactating • Well rounded, include variety of food • Special attention should
Flashcard 1410733837580
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Nutrition in pregnancy
folic acid needs • Appropriate intake is recommended (not necessary to “eat for two”) Canada’s Food Guide suggests the following: • 3 to 4 servings of milk per day • Increase intake by 100kCal per day in first trimester, <span>300 kCal/day in second and third trimester and by 450kCal/day when lactating • Well rounded, include variety of food • Special attention should be given to folate, calcium, vitami
Flashcard 1410735410444
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Nutrition in pregnancy
mmended (not necessary to “eat for two”) Canada’s Food Guide suggests the following: • 3 to 4 servings of milk per day • Increase intake by 100kCal per day in first trimester, 300 kCal/day in second and third trimester and by <span>450kCal/day when lactating • Well rounded, include variety of food • Special attention should be given to folate, calcium, vitamin D, iron and essential fatty acid intakes, becaus
Flashcard 1410736983308
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Nutrition in pregnancy
f milk per day • Increase intake by 100kCal per day in first trimester, 300 kCal/day in second and third trimester and by 450kCal/day when lactating • Well rounded, include variety of food • Special attention should be given to <span>folate, calcium, vitamin D, iron and essential fatty acid intakes, because there is potential for inadequate intakes in some groups of women (vegetarian, lactose intolerant, low BMI, NVP, poor socio-economic status, teen pregnancy).</sp
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410739866892
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Pregnancy weight gain
Optimal weight gain in pregnancy: • Inadequate maternal weight gain has been associated with growth restriction and prematurity • Excessive maternal weight gain has been associated with development of GDM and large-for-gestational-age babies • It is NOT recommended to try to lose weight during pregnanc
Flashcard 1410743012620
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Pregnancy weight gain
>Optimal weight gain in pregnancy: • Inadequate maternal weight gain has been associated with growth restriction and prematurity • Excessive maternal weight gain has been associated with development of GDM and large-for-gestational-age babies • It is NOT recommended to try to lose weight during pregnancy • A rough guideline for appropriate weight gain is 1-3.5 kg (2-8 lbs) in the first trimester, then one pound per
Flashcard 1410744585484
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Pregnancy weight gain
#13; • Excessive maternal weight gain has been associated with development of GDM and large-for-gestational-age babies • It is NOT recommended to try to lose weight during pregnancy • A rough guideline for appropriate weight gain is <span>1-3.5 kg (2-8 lbs) in the first trimester, then one pound per week to delivery. • Current recommendations for optimal weight gain depend on maternal prepregnancy body mass index (BMI)<span></
Flashcard 1410746158348
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Pregnancy weight gain
ssociated with development of GDM and large-for-gestational-age babies • It is NOT recommended to try to lose weight during pregnancy • A rough guideline for appropriate weight gain is 1-3.5 kg (2-8 lbs) in the first trimester, then <span>one pound per week to delivery. • Current recommendations for optimal weight gain depend on maternal prepregnancy body mass index (BMI)<span><body><html>
Flashcard 1410749828364


| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410754022668

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410758216972
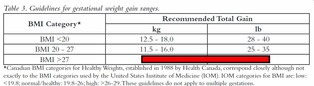
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410762411276
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410764246284
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410766081292
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410767916300
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410769751308
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410771586316
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410773421324
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410775256332
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410778402060
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
immunization in pregnancy
If a woman is rubella non-immune in pregnancy, give MMR vaccine immediately postpartum
Flashcard 1410779974924
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
immunization in pregnancy
If a woman is rubella non-immune in pregnancy, give MMR vaccine immediately postpartum
Flashcard 1410781547788
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
immunization in pregnancy
If a woman is rubella non-immune in pregnancy, give MMR vaccine immediately postpartum
Flashcard 1410785742092


| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410791771404
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410793606412

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410798325004

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410800160012

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410806713612

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410808548620

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410815888652

| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410818772236
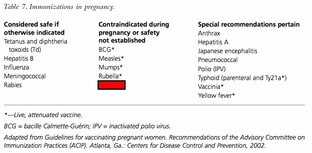
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410824277260
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410826112268
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410827947276
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410831093004
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
travel in pregnancy
Increased risk of DVT with prolonged immobility (long drives or flights) in pregnancy: • Move about during flight • Maintain good fluid intake • Avoid diuretics (caffeine) • Seek medical attention if leg swelling, pain, or chest pain/SOB after travel • Consider com
Flashcard 1410832665868
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
travel in pregnancy
Increased risk of DVT with prolonged immobility (long drives or flights) in pregnancy: • Move about during flight • Maintain good fluid intake • Avoid diuretics (caffeine) • Seek medical attention if leg swelling, pain, or chest pain/SOB after travel • Consider compression stockings
Flashcard 1410834238732
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
travel in pregnancy
Increased risk of DVT with prolonged immobility (long drives or flights) in pregnancy: • Move about during flight • Maintain good fluid intake • Avoid diuretics (caffeine) • Seek medical attention if leg swelling, pain, or chest pain/SOB after travel • Consider compression stockings
Flashcard 1410835811596
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
travel in pregnancy
head>Increased risk of DVT with prolonged immobility (long drives or flights) in pregnancy: • Move about during flight • Maintain good fluid intake • Avoid diuretics (caffeine) • Seek medical attention if leg swelling, pain, or chest pain/SOB after travel • Consider compression stockings<html>
Flashcard 1410837384460
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
travel in pregnancy
ity (long drives or flights) in pregnancy: • Move about during flight • Maintain good fluid intake • Avoid diuretics (caffeine) • Seek medical attention if leg swelling, pain, or chest pain/SOB after travel • Consider <span>compression stockings<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410842627340
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Early Vaginal Bleeding in pregnancy
Early Vaginal Bleeding • Not uncommon • Ultrasound after 7-8 weeks generally reassuring of viability • Avoid intercourse • Consider re-adjustment of activities (but bedrest not proven to prevent miscarriage)
Flashcard 1410844200204
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Early Vaginal Bleeding in pregnancy
Early Vaginal Bleeding • Not uncommon • Ultrasound after 7-8 weeks generally reassuring of viability • Avoid intercourse • Consider re-adjustment of activities (but bedrest not proven to prevent miscarriage)
Flashcard 1410845773068
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Early Vaginal Bleeding in pregnancy
Early Vaginal Bleeding • Not uncommon • Ultrasound after 7-8 weeks generally reassuring of viability • Avoid intercourse • Consider re-adjustment of activities (but bedrest not proven to prevent miscarriage)
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410851278092
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
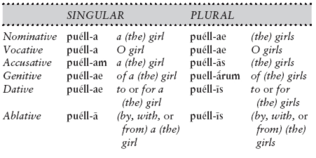
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410857045260
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
contraindicated meds
Contraindicated prescription meds: • ACE inhibitors: renal defects, IUGR, oligohydramnios • Tetracycline: stains teeth, may affect long bone development • Retinoids (Accutane): major human teratogen - craniofacial, cardiac, thy
Flashcard 1410859404556
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
contraindicated meds
Contraindicated prescription meds: • ACE inhibitors: renal defects, IUGR, oligohydramnios • Tetracycline: stains teeth, may affect long bone development • Retinoids (Accutane): major human teratogen - craniofacial, cardiac, thymic, and CNS malformations • Diet
Flashcard 1410861501708
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
contraindicated meds
Contraindicated prescription meds: • ACE inhibitors: renal defects, IUGR, oligohydramnios • Tetracycline: stains teeth, may affect long bone development • Retinoids (Accutane): major human teratogen - craniofacial, cardiac, thymic, and CNS malformations • Diethylstilbesterol (DES
Flashcard 1410863074572
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
contraindicated meds
Contraindicated prescription meds: • ACE inhibitors: renal defects, IUGR, oligohydramnios • Tetracycline: stains teeth, may affect long bone development • Retinoids (Accutane): major human teratogen - craniofacial, cardiac, thymic, and CNS malformations • Diethylstilbesterol (DES): historical risk: female genital tract structu
Flashcard 1410864647436
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
contraindicated meds
Contraindicated prescription meds: • ACE inhibitors: renal defects, IUGR, oligohydramnios • Tetracycline: stains teeth, may affect long bone development • Retinoids (Accutane): major human teratogen - craniofacial, cardiac, thymic, and CNS malformations • Diethylstilbesterol (DES): historical risk: female genital tract structural abnormalities, clear cel
Flashcard 1410866220300
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
contraindicated meds
d><head>Contraindicated prescription meds: • ACE inhibitors: renal defects, IUGR, oligohydramnios • Tetracycline: stains teeth, may affect long bone development • Retinoids (Accutane): major human teratogen - craniofacial, cardiac, thymic, and CNS malformations • Diethylstilbesterol (DES): historical risk: female genital tract structural abnormalities, clear cell carcinoma<html>
Flashcard 1410867793164
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
contraindicated meds
: • ACE inhibitors: renal defects, IUGR, oligohydramnios • Tetracycline: stains teeth, may affect long bone development • Retinoids (Accutane): major human teratogen - craniofacial, cardiac, thymic, and CNS malformations • <span>Diethylstilbesterol (DES): historical risk: female genital tract structural abnormalities, clear cell carcinoma<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410874346764
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
relatively contraindicated meds
Prescription meds in pregnancy - weight benefit v risk, consider change: • Anticonvulsants: most proven associations are ONTD, hydantoin syndrome (IUGR, mental retardation, facial and other anomalies). Other associations: congenital cardiac defects, limb-reduction defects, an
Flashcard 1410875919628
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
relatively contraindicated meds
Prescription meds in pregnancy - weight benefit v risk, consider change: • Anticonvulsants: most proven associations are ONTD, hydantoin syndrome (IUGR, mental retardation, facial and other anomalies). Other associations: congenital cardiac defects, limb-reduction defects, and other skeletal anomalies • Lithium (Ebstein’s anomaly) • Warfarin: pregnancy loss, warfarin embryo
Flashcard 1410878016780
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
relatively contraindicated meds
• Anticonvulsants: most proven associations are ONTD, hydantoin syndrome (IUGR, mental retardation, facial and other anomalies). Other associations: congenital cardiac defects, limb-reduction defects, and other skeletal anomalies • <span>Lithium (Ebstein’s anomaly) • Warfarin: pregnancy loss, warfarin embryopathy (nasal hypoplasia, epiphyseal stippling, optic atrophy, intra-cranial bleeds)<span><body><html>
Flashcard 1410879589644
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
relatively contraindicated meds
n associations are ONTD, hydantoin syndrome (IUGR, mental retardation, facial and other anomalies). Other associations: congenital cardiac defects, limb-reduction defects, and other skeletal anomalies • Lithium (Ebstein’s anomaly) • <span>Warfarin: pregnancy loss, warfarin embryopathy (nasal hypoplasia, epiphyseal stippling, optic atrophy, intra-cranial bleeds)<span><body><html>
Flashcard 1410881162508
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
relatively contraindicated meds
ions are ONTD, hydantoin syndrome (IUGR, mental retardation, facial and other anomalies). Other associations: congenital cardiac defects, limb-reduction defects, and other skeletal anomalies • Lithium (Ebstein’s anomaly) • Warfarin: <span>pregnancy loss, warfarin embryopathy (nasal hypoplasia, epiphyseal stippling, optic atrophy, intra-cranial bleeds)<span><body><html>
Flashcard 1410883259660
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410885094668
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410886929676
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410888764684
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410891386124
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
meds in breastfeeding
Maternal meds in breastfeeding: • Generally safe: penicillin, aminoglycosides, cephalosporins, combination OCP (may decrease milk supply), DepoProvera • Avoid: tetracycline, antineoplastics, some immunosuppressives, Accutane</b
Flashcard 1410892958988
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
meds in breastfeeding
Maternal meds in breastfeeding: • Generally safe: penicillin, aminoglycosides, cephalosporins, combination OCP (may decrease milk supply), DepoProvera • Avoid: tetracycline, antineoplastics, some immunosuppressives, Accutane
Flashcard 1410894531852
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
meds in breastfeeding
Maternal meds in breastfeeding: • Generally safe: penicillin, aminoglycosides, cephalosporins, combination OCP (may decrease milk supply), DepoProvera • Avoid: tetracycline, antineoplastics, some immunosuppressives, Accutane
Flashcard 1410896104716
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
meds in breastfeeding
Maternal meds in breastfeeding: • Generally safe: penicillin, aminoglycosides, cephalosporins, combination OCP (may decrease milk supply), DepoProvera • Avoid: tetracycline, antineoplastics, some immunosuppressives, Accutane
Flashcard 1410897677580
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
meds in breastfeeding
Maternal meds in breastfeeding: • Generally safe: penicillin, aminoglycosides, cephalosporins, combination OCP (may decrease milk supply), DepoProvera • Avoid: tetracycline, antineoplastics, some immunosuppressives, Accutane
Flashcard 1410899250444
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
meds in breastfeeding
Maternal meds in breastfeeding: • Generally safe: penicillin, aminoglycosides, cephalosporins, combination OCP (may decrease milk supply), DepoProvera • Avoid: tetracycline, antineoplastics, some immunosuppressives, Accutane
Flashcard 1410900823308
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
meds in breastfeeding
Maternal meds in breastfeeding: • Generally safe: penicillin, aminoglycosides, cephalosporins, combination OCP (may decrease milk supply), DepoProvera • Avoid: tetracycline, antineoplastics, some immunosuppressives, Accutane
Flashcard 1410902396172
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
meds in breastfeeding
Maternal meds in breastfeeding: • Generally safe: penicillin, aminoglycosides, cephalosporins, combination OCP (may decrease milk supply), DepoProvera • Avoid: tetracycline, antineoplastics, some immunosuppressives, Accutane
Flashcard 1410903969036
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
meds in breastfeeding
body>Maternal meds in breastfeeding: • Generally safe: penicillin, aminoglycosides, cephalosporins, combination OCP (may decrease milk supply), DepoProvera • Avoid: tetracycline, antineoplastics, some immunosuppressives, Accutane<body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410907901196
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Flashcard 1410912357644
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
constipation
Constipation in pregnancy: • Dietary adjustments (adequate fluids, fibre) • Reconsider/reduce prenatal vitamins (folate needs to be continued till >12 wks) • Stool softeners/fibre supplement (Colace, Metamucil) PRN
Flashcard 1410913930508
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
constipation
Constipation in pregnancy: • Dietary adjustments (adequate fluids, fibre) • Reconsider/reduce prenatal vitamins (folate needs to be continued till >12 wks) • Stool softeners/fibre supplement (Colace, Metamucil) PRN
Flashcard 1410915503372
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
constipation
Constipation in pregnancy: • Dietary adjustments (adequate fluids, fibre) • Reconsider/reduce prenatal vitamins (folate needs to be continued till >12 wks) • Stool softeners/fibre supplement (Colace, Metamucil) PRN
Flashcard 1410917076236
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
constipation
Constipation in pregnancy: • Dietary adjustments (adequate fluids, fibre) • Reconsider/reduce prenatal vitamins (folate needs to be continued till >12 wks) • Stool softeners/fibre supplement (Colace, Metamucil) PRN
Flashcard 1410918649100
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
constipation
l>Constipation in pregnancy: • Dietary adjustments (adequate fluids, fibre) • Reconsider/reduce prenatal vitamins (folate needs to be continued till >12 wks) • Stool softeners/fibre supplement (Colace, Metamucil) PRN<html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410921532684
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
hemorrhoids
Hemorrhoids in pregnancy: • Avoid straining • Avoid constipation • Cream or suppositories if symptomatic (Anusol) - available with topical steroid and with topical analgesic • Sitz baths, Tucks pads</
Flashcard 1410923105548
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
hemorrhoids
Hemorrhoids in pregnancy: • Avoid straining • Avoid constipation • Cream or suppositories if symptomatic (Anusol) - available with topical steroid and with topical analgesic • Sitz baths, Tucks pads
Flashcard 1410924678412
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
hemorrhoids
Hemorrhoids in pregnancy: • Avoid straining • Avoid constipation • Cream or suppositories if symptomatic (Anusol) - available with topical steroid and with topical analgesic • Sitz baths, Tucks pads
Flashcard 1410926251276
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
hemorrhoids
Hemorrhoids in pregnancy: • Avoid straining • Avoid constipation • Cream or suppositories if symptomatic (Anusol) - available with topical steroid and with topical analgesic • Sitz baths, Tucks pads
Flashcard 1410927824140
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
hemorrhoids
Hemorrhoids in pregnancy: • Avoid straining • Avoid constipation • Cream or suppositories if symptomatic (Anusol) - available with topical steroid and with topical analgesic • Sitz baths, Tucks pads
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410930707724
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
vaginitis - yeast
Yeast vaginitis in pregnancy: • Common due to high estrogen environment • Treat locally with antifungal agents if symptomatic (Monistat, Canesten - preferable not to use the plastic applicator, use finger) • May recur or require prolon
Flashcard 1410932280588
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
vaginitis - yeast
Yeast vaginitis in pregnancy: • Common due to high estrogen environment • Treat locally with antifungal agents if symptomatic (Monistat, Canesten - preferable not to use the plastic applicator, use finger) • May recur or require prolonged course of therapy • Oral fluconazole if
Flashcard 1410933853452
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
vaginitis - yeast
Yeast vaginitis in pregnancy: • Common due to high estrogen environment • Treat locally with antifungal agents if symptomatic (Monistat, Canesten - preferable not to use the plastic applicator, use finger) • May recur or require prolonged course of therapy • Oral fluconazole if all else fails (class C)</bo
Flashcard 1410935426316
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
vaginitis - yeast
on due to high estrogen environment • Treat locally with antifungal agents if symptomatic (Monistat, Canesten - preferable not to use the plastic applicator, use finger) • May recur or require prolonged course of therapy • Oral <span>fluconazole if all else fails (class C)<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410938309900
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
vaginitis - bacterial
Bacterial Vaginosis - vaginitis in pregnancy: • Need to treat is controversial • Treat if previous preterm labour or risk factors for preterm labour • Treat with oral or vaginal flagyl
Flashcard 1410939882764
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
vaginitis - bacterial
Bacterial Vaginosis - vaginitis in pregnancy: • Need to treat is controversial • Treat if previous preterm labour or risk factors for preterm labour • Treat with oral or vaginal flagyl
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410942766348
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
urinary freq
Urinary Frequency in pregnancy • Common symptom throughout pregnancy • Rule out urinary tract infection • If culture is positive, treat with appropriate antibiotic • Use macrodantin, ampicillin, septra; avoid sulpha, tetracycline • Reculture as indicated
Flashcard 1410944339212
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
urinary freq
Urinary Frequency in pregnancy • Common symptom throughout pregnancy • Rule out urinary tract infection • If culture is positive, treat with appropriate antibiotic • Use macrodantin, ampicillin, septra; avoid sulpha, tetracycline • Reculture as indicated
Flashcard 1410945912076
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
urinary freq
y>Urinary Frequency in pregnancy • Common symptom throughout pregnancy • Rule out urinary tract infection • If culture is positive, treat with appropriate antibiotic • Use macrodantin, ampicillin, septra; avoid sulpha, tetracycline • Reculture as indicated<body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410948795660
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
hand numbness
Numbness of hands in preg. • Carpal tunnel syndrome most common cause (compression of median nerve) • Wrist splints or steroid injections may be of benefit • Decrease aggravating factors (prolonged computer work) • Most re
Flashcard 1410950368524
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
hand numbness
Numbness of hands in preg. • Carpal tunnel syndrome most common cause (compression of median nerve) • Wrist splints or steroid injections may be of benefit • Decrease aggravating factors (prolonged computer work) • Most resolve after pregnancy - if not, surgery may be required
Flashcard 1410951941388
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
hand numbness
• Carpal tunnel syndrome most common cause (compression of median nerve) • Wrist splints or steroid injections may be of benefit • Decrease aggravating factors (prolonged computer work) • Most resolve after pregnancy - if not, <span>surgery may be required<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410954824972
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
sleep disturbance
Sleep Disturbances in preg. • Anxiety, abdominal pain, fetal movement, physical changes, abdominal enlargement, ligament laxity, urinary frequency, use of unnatural sleep positions all contribute • Consider naps, sleep
Flashcard 1410956397836
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
sleep disturbance
Sleep Disturbances in preg. • Anxiety, abdominal pain, fetal movement, physical changes, abdominal enlargement, ligament laxity, urinary frequency, use of unnatural sleep positions all contribute • Consider naps, sleep in chair,
Flashcard 1410957970700
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
sleep disturbance
Sleep Disturbances in preg. • Anxiety, abdominal pain, fetal movement, physical changes, abdominal enlargement, ligament laxity, urinary frequency, use of unnatural sleep positions all contribute • Consider naps, sleep in chair, body pillows, modific
Flashcard 1410959543564
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
sleep disturbance
Sleep Disturbances in preg. • Anxiety, abdominal pain, fetal movement, physical changes, abdominal enlargement, ligament laxity, urinary frequency, use of unnatural sleep positions all contribute • Consider naps, sleep in chair, body pillows, modification of responsibilities • Encourage sleeping on lef
Flashcard 1410961116428
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
sleep disturbance
Sleep Disturbances in preg. • Anxiety, abdominal pain, fetal movement, physical changes, abdominal enlargement, ligament laxity, urinary frequency, use of unnatural sleep positions all contribute • Consider naps, sleep in chair, body pillows, modification of responsibilities • Encourage sleeping on left side/uterine wedg
Flashcard 1410962689292
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
sleep disturbance
Sleep Disturbances in preg. • Anxiety, abdominal pain, fetal movement, physical changes, abdominal enlargement, ligament laxity, urinary frequency, use of unnatural sleep positions all contribute • Consider naps, sleep in chair, body pillows, modification of responsibilities • Encourage sleeping on left side/uterine wedge to maximize uteroplacental blood
Flashcard 1410964262156
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
sleep disturbance
><head>Sleep Disturbances in preg. • Anxiety, abdominal pain, fetal movement, physical changes, abdominal enlargement, ligament laxity, urinary frequency, use of unnatural sleep positions all contribute • Consider naps, sleep in chair, body pillows, modification of responsibilities • Encourage sleeping on left side/uterine wedge to maximize uteroplacental blood flow • Not generally recommended to treat with sleeping pills (sedatives, anxiolytics) as most
Flashcard 1410965835020
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
sleep disturbance
fetal movement, physical changes, abdominal enlargement, ligament laxity, urinary frequency, use of unnatural sleep positions all contribute • Consider naps, sleep in chair, body pillows, modification of responsibilities • Encourage <span>sleeping on left side/uterine wedge to maximize uteroplacental blood flow • Not generally recommended to treat with sleeping pills (sedatives, anxiolytics) as most are habit forming<span><body><html>
Flashcard 1410967670028
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
sleep disturbance
rgement, ligament laxity, urinary frequency, use of unnatural sleep positions all contribute • Consider naps, sleep in chair, body pillows, modification of responsibilities • Encourage sleeping on left side/uterine wedge to maximize <span>uteroplacental blood flow • Not generally recommended to treat with sleeping pills (sedatives, anxiolytics) as most are habit forming<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410970553612
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
edema
Edema in preg. • Common normal experience • Rule out pathology such as pre-eclampsia, deep venous thrombosis (DVT), congestive heart failure (peripartum cardiomyopathy, women with previous cardiac history) • Consider compression stockings or support pantyhose • Elevate lower extremities above level of heart • Avoid standing for long periods
Flashcard 1410972126476
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
edema
span>Edema in preg. • Common normal experience • Rule out pathology such as pre-eclampsia, deep venous thrombosis (DVT), congestive heart failure (peripartum cardiomyopathy, women with previous cardiac history) • Consider compression stockings or support pantyhose • Elevate lower extremities above level of heart • Avoid standing for long periods<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410975010060
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
headache
Headaches in preg. • Common especially early to mid T2 • Rule out pathology: check BP, blood sugar • Use of analgesia as indicated, acetaminophen preferred • Adequate rest • Severe unremitting headaches need to be invest
Flashcard 1410976582924
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
headache
Headaches in preg. • Common especially early to mid T2 • Rule out pathology: check BP, blood sugar • Use of analgesia as indicated, acetaminophen preferred • Adequate rest • Severe unremitting headaches need to be investigated as per non pregnant</
Flashcard 1410978155788
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
headache
Headaches in preg. • Common especially early to mid T2 • Rule out pathology: check BP, blood sugar • Use of analgesia as indicated, acetaminophen preferred • Adequate rest • Severe unremitting headaches need to be investigated as per non pregnant
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410981039372
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
round ligament pain
Round ligament pain in preg. • Commonly experienced in mid T2 • Pain generally felt in right or left lower aspect of uterus, radiating into the groin and aggravated by movement, shifting, walking, etc. • No specific management: supportiv
Flashcard 1410982612236
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
round ligament pain
Round ligament pain in preg. • Commonly experienced in mid T2 • Pain generally felt in right or left lower aspect of uterus, radiating into the groin and aggravated by movement, shifting, walking, etc. • No specific management: supportive care, rule out other etiologies for pain, adjust position, reassure</h
Flashcard 1410984185100
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
round ligament pain
Round ligament pain in preg. • Commonly experienced in mid T2 • Pain generally felt in right or left lower aspect of uterus, radiating into the groin and aggravated by movement, shifting, walking, etc. • No specific management: <span>supportive care, rule out other etiologies for pain, adjust position, reassure<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1410987068684
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx of labour
Dx of Labour: • Expect irregular, not excessively painful contractions which become more frequent, regular and uncomfortable • Often start in low back and come around to front/lower abdomen • Character may be similar to menstrual cramps • Ultimately generally require moderate to strong contractions every 2-3 minutes (start t
Flashcard 1410988641548
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx of labour
Dx of Labour: • Expect irregular, not excessively painful contractions which become more frequent, regular and uncomfortable • Often start in low back and come around to front/lower abdomen • Character may be similar to menstrual cramps • Ultimately generally require moderate to strong contractions every 2-3 minutes (start to start) lasting 45 to 60 seconds to re
Flashcard 1410990214412
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx of labour
n>Dx of Labour: • Expect irregular, not excessively painful contractions which become more frequent, regular and uncomfortable • Often start in low back and come around to front/lower abdomen • Character may be similar to menstrual cramps • Ultimately generally require moderate to strong contractions every 2-3 minutes (start to start) lasting 45 to 60 seconds to result in expected cervical changes • Often assoc
Flashcard 1410991787276
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx of labour
cessively painful contractions which become more frequent, regular and uncomfortable • Often start in low back and come around to front/lower abdomen • Character may be similar to menstrual cramps • Ultimately generally require <span>moderate to strong contractions every 2-3 minutes (start to start) lasting 45 to 60 seconds to result in expected cervical changes • Often associated with small amount of vaginal loss of blood stained mucous, als
Flashcard 1410993360140
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx of labour
ecome more frequent, regular and uncomfortable • Often start in low back and come around to front/lower abdomen • Character may be similar to menstrual cramps • Ultimately generally require moderate to strong contractions every <span>2-3 minutes (start to start) lasting 45 to 60 seconds to result in expected cervical changes • Often associated with small amount of vaginal loss of blood stained mucous, also called “
Flashcard 1410994933004
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx of labour
mfortable • Often start in low back and come around to front/lower abdomen • Character may be similar to menstrual cramps • Ultimately generally require moderate to strong contractions every 2-3 minutes (start to start) lasting <span>45 to 60 seconds to result in expected cervical changes • Often associated with small amount of vaginal loss of blood stained mucous, also called “bloody show” • 30% of women rupture t
Flashcard 1410996505868
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx of labour
) lasting 45 to 60 seconds to result in expected cervical changes • Often associated with small amount of vaginal loss of blood stained mucous, also called “bloody show” • 30% of women rupture their membranes before the pain starts (<span>prelabour rupture of membranes or PROM) • Ruptured membranes is identified by a gush of fluid and/or ongoing leakage • Amniotic fluid loss is confirmed by Nitrazine test and ferning • Nitrazine paper will turn
Flashcard 1410998078732
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx of labour
ody show” • 30% of women rupture their membranes before the pain starts (prelabour rupture of membranes or PROM) • Ruptured membranes is identified by a gush of fluid and/or ongoing leakage • Amniotic fluid loss is confirmed by <span>Nitrazine test and ferning • Nitrazine paper will turn dark blue when wet with amniotic fluid • Nitrazine test is confirmed by placing a sample of the fluid on a glass slide, allowing it to air dry well
Flashcard 1410999651596
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx of labour
the pain starts (prelabour rupture of membranes or PROM) • Ruptured membranes is identified by a gush of fluid and/or ongoing leakage • Amniotic fluid loss is confirmed by Nitrazine test and ferning • Nitrazine paper will turn <span>dark blue when wet with amniotic fluid • Nitrazine test is confirmed by placing a sample of the fluid on a glass slide, allowing it to air dry well and then examining this under the microsco
Flashcard 1411001224460
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx of labour
ne test is confirmed by placing a sample of the fluid on a glass slide, allowing it to air dry well and then examining this under the microscope for the presence of a “fern-like” pattern • Nitrazine paper can turn blue in the presence of <span>semen, blood and vaginitis so it is not diagnostic of amniotic fluid presence • A positive fern test is diagnostic for the presence of amniotic fluid<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411004108044
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Hospital for Labour
Generally, patient should go to the hospital for labour if: • Regular painful contractions increasing in intensity and frequency • Spontaneous rupture of membranes (SROM) ---• If fluid looks green, go to hospital (meconium could indicate fetal stress) ---• If fluid is excessively bloody ---• If woman is GBS positive (antibiotics will be required) ---• If baby is no
Flashcard 1411005680908
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Hospital for Labour
patient should go to the hospital for labour if: • Regular painful contractions increasing in intensity and frequency • Spontaneous rupture of membranes (SROM) ---• If fluid looks green, go to hospital (meconium could indicate <span>fetal stress) ---• If fluid is excessively bloody ---• If woman is GBS positive (antibiotics will be required) ---• If baby is not in vertex position • If fluid is clear and ther
Flashcard 1411007253772
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Hospital for Labour
: • Regular painful contractions increasing in intensity and frequency • Spontaneous rupture of membranes (SROM) ---• If fluid looks green, go to hospital (meconium could indicate fetal stress) ---• If fluid is excessively <span>bloody ---• If woman is GBS positive (antibiotics will be required) ---• If baby is not in vertex position • If fluid is clear and there are no problems and no contractions, cal
Flashcard 1411008826636
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Hospital for Labour
ractions increasing in intensity and frequency • Spontaneous rupture of membranes (SROM) ---• If fluid looks green, go to hospital (meconium could indicate fetal stress) ---• If fluid is excessively bloody ---• If woman is <span>GBS positive (antibiotics will be required) ---• If baby is not in vertex position • If fluid is clear and there are no problems and no contractions, call in to labour and delivery --
Flashcard 1411010399500
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Hospital for Labour
e of membranes (SROM) ---• If fluid looks green, go to hospital (meconium could indicate fetal stress) ---• If fluid is excessively bloody ---• If woman is GBS positive (antibiotics will be required) ---• If baby is not in <span>vertex position • If fluid is clear and there are no problems and no contractions, call in to labour and delivery ---• Expect onset of labour within 24 hrs in a majority of women
Flashcard 1411011972364
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Hospital for Labour
If woman is GBS positive (antibiotics will be required) ---• If baby is not in vertex position • If fluid is clear and there are no problems and no contractions, call in to labour and delivery ---• Expect onset of labour within <span>24 hrs in a majority of women ---• If labour does not ensue, usually the woman’s labour will be induced (in 12-24 hrs) • Heavy bleeding (not bloody show) is indication to go to h
Flashcard 1411013545228
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Hospital for Labour
id is clear and there are no problems and no contractions, call in to labour and delivery ---• Expect onset of labour within 24 hrs in a majority of women ---• If labour does not ensue, usually the woman’s labour will be induced (in <span>12-24 hrs) • Heavy bleeding (not bloody show) is indication to go to hospital • At any point if uncertain, better to attend hospital (advise women at prenatal visits that it is comm
Flashcard 1411015118092
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Hospital for Labour
e no problems and no contractions, call in to labour and delivery ---• Expect onset of labour within 24 hrs in a majority of women ---• If labour does not ensue, usually the woman’s labour will be induced (in 12-24 hrs) • Heavy <span>bleeding (not bloody show) is indication to go to hospital • At any point if uncertain, better to attend hospital (advise women at prenatal visits that it is common to be sent home from L&D)</span
Flashcard 1411017477388
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411020623116
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
etio of postmenopausal bleeding
Etiology of Postmenopausal Bleeding • Atrophic vulvovaginitis (most common causes) • Exogenous estrogen • Endometrial cancer (15-20%) • Endometrial hyperplasia • Endometrial or cervical polyps • Cervical ectropion • O
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411045264652
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx eval of postmenopausal bleeding
Diagnostic Evaluation Though most women with PMB will have atrophic vulvovaginitis or some other benign underlying cause, all women with PMB should be evaluated to rule out endometrial cancer, since 15-20% of women with this symptom will have the disease. The risk of
Flashcard 1411046837516
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx eval of postmenopausal bleeding
Diagnostic Evaluation Though most women with PMB will have atrophic vulvovaginitis or some other benign underlying cause, all women with PMB should be evaluated to rule out endometrial cancer, since 15-20% of women with this symptom will have the disease. The risk of harbouring endometrial cancer increases with age from a low of 15% in the immediately postmenopausal cohort t
Flashcard 1411048410380
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx eval of postmenopausal bleeding
Diagnostic Evaluation Though most women with PMB will have atrophic vulvovaginitis or some other benign underlying cause, all women with PMB should be evaluated to rule out endometrial cancer, since 15-20% of women with this symptom will have the disease. The risk of harbouring endometrial cancer increases with age from a low of 15% in the immediately postmenopausal cohort to 50% in pati
Flashcard 1411049983244
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx eval of postmenopausal bleeding
me other benign underlying cause, all women with PMB should be evaluated to rule out endometrial cancer, since 15-20% of women with this symptom will have the disease. The risk of harbouring endometrial cancer increases with age from a low of <span>15% in the immediately postmenopausal cohort to 50% in patients 80 years or older. Initial evaluation should include a relevant history and physical examination, which must incl
Flashcard 1411051556108
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx eval of postmenopausal bleeding
PMB should be evaluated to rule out endometrial cancer, since 15-20% of women with this symptom will have the disease. The risk of harbouring endometrial cancer increases with age from a low of 15% in the immediately postmenopausal cohort to <span>50% in patients 80 years or older. Initial evaluation should include a relevant history and physical examination, which must include a pelvic examination. An endometrial biopsy
Flashcard 1411053128972
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx eval of postmenopausal bleeding
valuated to rule out endometrial cancer, since 15-20% of women with this symptom will have the disease. The risk of harbouring endometrial cancer increases with age from a low of 15% in the immediately postmenopausal cohort to 50% in patients <span>80 years or older. Initial evaluation should include a relevant history and physical examination, which must include a pelvic examination. An endometrial biopsy should be perfor
Flashcard 1411054701836
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx eval of postmenopausal bleeding
ometrial cancer increases with age from a low of 15% in the immediately postmenopausal cohort to 50% in patients 80 years or older. Initial evaluation should include a relevant history and physical examination, which must include a <span>pelvic examination. An endometrial biopsy should be performed and any obvious lesion of the cervix or vagina should be biopsied directly. Endocervical curettage (ECC) should be considered if t
Flashcard 1411056274700
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx eval of postmenopausal bleeding
es with age from a low of 15% in the immediately postmenopausal cohort to 50% in patients 80 years or older. Initial evaluation should include a relevant history and physical examination, which must include a pelvic examination. An <span>endometrial biopsy should be performed and any obvious lesion of the cervix or vagina should be biopsied directly. Endocervical curettage (ECC) should be considered if there is clinical concern regarding
Flashcard 1411057847564
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx eval of postmenopausal bleeding
ately postmenopausal cohort to 50% in patients 80 years or older. Initial evaluation should include a relevant history and physical examination, which must include a pelvic examination. An endometrial biopsy should be performed and <span>any obvious lesion of the cervix or vagina should be biopsied directly. Endocervical curettage (ECC) should be considered if there is clinical concern regarding the possibility of cancer within the endocervical canal.
Flashcard 1411059420428
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx eval of postmenopausal bleeding
#13; Initial evaluation should include a relevant history and physical examination, which must include a pelvic examination. An endometrial biopsy should be performed and any obvious lesion of the cervix or vagina should be biopsied directly. <span>Endocervical curettage (ECC) should be considered if there is clinical concern regarding the possibility of cancer within the endocervical canal. Endometrial sampling should be routinely considered for p
Flashcard 1411060993292
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx eval of postmenopausal bleeding
performed and any obvious lesion of the cervix or vagina should be biopsied directly. Endocervical curettage (ECC) should be considered if there is clinical concern regarding the possibility of cancer within the endocervical canal. <span>Endometrial sampling should be routinely considered for patients with PMB to rule out endometrial cancer. Pelvic ultrasound can occasionally be useful as an adjunct to pelvic examination and endo
Flashcard 1411062566156
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx eval of postmenopausal bleeding
Endocervical curettage (ECC) should be considered if there is clinical concern regarding the possibility of cancer within the endocervical canal. Endometrial sampling should be routinely considered for patients with PMB to rule out <span>endometrial cancer. Pelvic ultrasound can occasionally be useful as an adjunct to pelvic examination and endometrial sampling in the evaluation of women with PMB. This test is most useful in wo
Flashcard 1411064139020
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx eval of postmenopausal bleeding
ould be considered if there is clinical concern regarding the possibility of cancer within the endocervical canal. Endometrial sampling should be routinely considered for patients with PMB to rule out endometrial cancer. <span>Pelvic ultrasound can occasionally be useful as an adjunct to pelvic examination and endometrial sampling in the evaluation of women with PMB. This test is most useful in women where adequate endometrial
Flashcard 1411065711884
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx eval of postmenopausal bleeding
possibility of cancer within the endocervical canal. Endometrial sampling should be routinely considered for patients with PMB to rule out endometrial cancer. Pelvic ultrasound can occasionally be useful as an adjunct to <span>pelvic examination and endometrial sampling in the evaluation of women with PMB. This test is most useful in women where adequate endometrial sampling is not feasible without invasive methods (ie D+C +/-
Flashcard 1411067284748
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx eval of postmenopausal bleeding
ithin the endocervical canal. Endometrial sampling should be routinely considered for patients with PMB to rule out endometrial cancer. Pelvic ultrasound can occasionally be useful as an adjunct to pelvic examination and <span>endometrial sampling in the evaluation of women with PMB. This test is most useful in women where adequate endometrial sampling is not feasible without invasive methods (ie D+C +/- hysteroscopy). Ultrasound
Flashcard 1411068857612
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx eval of postmenopausal bleeding
atients with PMB to rule out endometrial cancer. Pelvic ultrasound can occasionally be useful as an adjunct to pelvic examination and endometrial sampling in the evaluation of women with PMB. This test is most useful in women where <span>adequate endometrial sampling is not feasible without invasive methods (ie D+C +/- hysteroscopy). Ultrasound performed using an endovaginal probe can serve two purposes: to rule out the presence of other pelvic path
Flashcard 1411070430476
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx eval of postmenopausal bleeding
examination and endometrial sampling in the evaluation of women with PMB. This test is most useful in women where adequate endometrial sampling is not feasible without invasive methods (ie D+C +/- hysteroscopy). Ultrasound performed using an <span>endovaginal probe can serve two purposes: to rule out the presence of other pelvic pathology not detected on pelvic examination (e.g. ovarian neoplasms) and to directly measure the endometrial thic
Flashcard 1411072003340
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx eval of postmenopausal bleeding
PMB. This test is most useful in women where adequate endometrial sampling is not feasible without invasive methods (ie D+C +/- hysteroscopy). Ultrasound performed using an endovaginal probe can serve two purposes: to rule out the presence of <span>other pelvic pathology not detected on pelvic examination (e.g. ovarian neoplasms) and to directly measure the endometrial thickness as a surrogate for the likelihood of an underlying endometrial carcinoma. An endometrial thickness of 5mm or more is considered abnorma
Flashcard 1411073576204
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx eval of postmenopausal bleeding
hods (ie D+C +/- hysteroscopy). Ultrasound performed using an endovaginal probe can serve two purposes: to rule out the presence of other pelvic pathology not detected on pelvic examination (e.g. ovarian neoplasms) and to directly measure the <span>endometrial thickness as a surrogate for the likelihood of an underlying endometrial carcinoma. An endometrial thickness of 5mm or more is considered abnormal. Although women with a thin endometrium rarely have an underlying type I endometrial cancer, women with type II endometri
Flashcard 1411075149068
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx eval of postmenopausal bleeding
ence of other pelvic pathology not detected on pelvic examination (e.g. ovarian neoplasms) and to directly measure the endometrial thickness as a surrogate for the likelihood of an underlying endometrial carcinoma. An endometrial thickness of <span>5mm or more is considered abnormal. Although women with a thin endometrium rarely have an underlying type I endometrial cancer, women with type II endometrial cancer may have an endometri
Flashcard 1411076721932
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx eval of postmenopausal bleeding
measure the endometrial thickness as a surrogate for the likelihood of an underlying endometrial carcinoma. An endometrial thickness of 5mm or more is considered abnormal. Although women with a thin endometrium rarely have an underlying type <span>I endometrial cancer, women with type II endometrial cancer may have an endometrial thickness less than 5mm. A thickened endometrium is not always indicative of an underlying endometrial
Flashcard 1411078294796
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx eval of postmenopausal bleeding
oma. An endometrial thickness of 5mm or more is considered abnormal. Although women with a thin endometrium rarely have an underlying type I endometrial cancer, women with type II endometrial cancer may have an endometrial thickness less than <span>5mm. A thickened endometrium is not always indicative of an underlying endometrial cancer, as large endometrial polyps, submucous fibroids, characteristic tamoxifen effects (subendothelia
Flashcard 1411079867660
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Dx eval of postmenopausal bleeding
n endometrium rarely have an underlying type I endometrial cancer, women with type II endometrial cancer may have an endometrial thickness less than 5mm. A thickened endometrium is not always indicative of an underlying endometrial cancer, as <span>large endometrial polyps, submucous fibroids, characteristic tamoxifen effects (subendothelial cystic hyperplasia), or adenomyosis may result in an apparent thickened endometrium on ultrasound. As a result of this lack of diagnostic sensitivity and specificity, ultrasound is not acceptable as an alternative to pelv
Flashcard 1411081440524
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411084586252
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
endometrial ca risk factors
Endometrial cancer risk factor: excessive estrogen unopposed by progesterone is associated with most of the clinical risk factors linked to endometrial carcinoma (obesity, nulliparity, early onset menarche, late onset menopause, unoppos
Flashcard 1411086159116
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
endometrial ca risk factors
Endometrial cancer risk factor: excessive estrogen unopposed by progesterone is associated with most of the clinical risk factors linked to endometrial carcinoma (obesity, nulliparity, early onset menarche, late onset menopause, unopposed estrogen replacement th
Flashcard 1411087731980
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
endometrial ca risk factors
Endometrial cancer risk factor: excessive estrogen unopposed by progesterone is associated with most of the clinical risk factors linked to endometrial carcinoma (obesity, nulliparity, early onset menarche, late onset menopause, unopposed estrogen replacement therapy)
Flashcard 1411089304844
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
endometrial ca risk factors
Endometrial cancer risk factor: excessive estrogen unopposed by progesterone is associated with most of the clinical risk factors linked to endometrial carcinoma (obesity, nulliparity, early onset menarche, late onset menopause, unopposed estrogen replacement therapy)
Flashcard 1411090877708
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
endometrial ca risk factors
Endometrial cancer risk factor: excessive estrogen unopposed by progesterone is associated with most of the clinical risk factors linked to endometrial carcinoma (obesity, nulliparity, early onset menarche, late onset menopause, unopposed estrogen replacement therapy)
Flashcard 1411092450572
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
endometrial ca risk factors
Endometrial cancer risk factor: excessive estrogen unopposed by progesterone is associated with most of the clinical risk factors linked to endometrial carcinoma (obesity, nulliparity, early onset menarche, late onset menopause, unopposed estrogen replacement therapy)<html>
Flashcard 1411094023436
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
endometrial ca risk factors
an>Endometrial cancer risk factor: excessive estrogen unopposed by progesterone is associated with most of the clinical risk factors linked to endometrial carcinoma (obesity, nulliparity, early onset menarche, late onset menopause, unopposed estrogen replacement therapy)<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411096907020
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
tamoxifen
Women taking tamoxifen who develop abnormal vaginal bleeding should undergo appropriate evaluation to rule out endometrial cancer, but routine screening is not warranted.
Flashcard 1411098479884
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
tamoxifen
Women taking tamoxifen who develop abnormal vaginal bleeding should undergo appropriate evaluation to rule out endometrial cancer, but routine screening is not warranted.
Flashcard 1411100052748
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
tamoxifen
Women taking tamoxifen who develop abnormal vaginal bleeding should undergo appropriate evaluation to rule out endometrial cancer, but routine screening is not warranted.
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411102936332
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Women who have had at least one full-term pregnancy and those who have taken oral contraceptives have a lower risk of developing endometrial cancer, presumably through reduction of exposure to unopposed estrogen levels</bod
Flashcard 1411104509196
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Women who have had at least one full-term pregnancy and those who have taken oral contraceptives have a lower risk of developing endometrial cancer, presumably through reduction of exposure to unopposed estrogen levels
Flashcard 1411106082060
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Women who have had at least one full-term pregnancy and those who have taken oral contraceptives have a lower risk of developing endometrial cancer, presumably through reduction of exposure to unopposed estrogen levels
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411108965644
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
type 1 endometrial ca
Type I endometrial ca is typically related to unopposed estrogen, either endogenous (obesity or ovarian pathology) or exogenous (unbalanced estrogen supplementation). Women with type I endomet
Flashcard 1411110538508
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
type 1 endometrial ca
Type I endometrial ca is typically related to unopposed estrogen, either endogenous (obesity or ovarian pathology) or exogenous (unbalanced estrogen supplementation). Women with type I endometrial cancers typically have clinical risk factors includin
Flashcard 1411112111372
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
type 1 endometrial ca
Type I endometrial ca is typically related to unopposed estrogen, either endogenous (obesity or ovarian pathology) or exogenous (unbalanced estrogen supplementation). Women with type I endometrial cancers typically have clinical risk factors including obesity, nulliparity, and late onset menopause.
Flashcard 1411113684236
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
type 1 endometrial ca
Type I endometrial ca is typically related to unopposed estrogen, either endogenous (obesity or ovarian pathology) or exogenous (unbalanced estrogen supplementation). Women with type I endometrial cancers typically have clinical risk factors including obesity, nulliparity, and late onset menopause. These tumours are typically diagnosed at an early
Flashcard 1411115257100
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
type 1 endometrial ca
dometrial ca is typically related to unopposed estrogen, either endogenous (obesity or ovarian pathology) or exogenous (unbalanced estrogen supplementation). Women with type I endometrial cancers typically have clinical risk factors including <span>obesity, nulliparity, and late onset menopause. These tumours are typically diagnosed at an early stage because most women experience abnormal vaginal bleeding that is amenable to definitive investigation early during the course of
Flashcard 1411116829964
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
type 1 endometrial ca
arian pathology) or exogenous (unbalanced estrogen supplementation). Women with type I endometrial cancers typically have clinical risk factors including obesity, nulliparity, and late onset menopause. These tumours are typically diagnosed at <span>an early stage because most women experience abnormal vaginal bleeding that is amenable to definitive investigation early during the course of the disease (office endometrial biopsy). Type I end
Flashcard 1411118402828
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
type 1 endometrial ca
ding that is amenable to definitive investigation early during the course of the disease (office endometrial biopsy). Type I endometrial cancers are usually characterized by histology consistent with endometrioid adenocarcinoma that are often <span>well-differentiated and only superficially invasive tumors at diagnosis. The prognosis for women with these tumours is typically excellent since they are often cured with definitive surgery alone.</
Flashcard 1411119975692
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
type 1 endometrial ca
most women experience abnormal vaginal bleeding that is amenable to definitive investigation early during the course of the disease (office endometrial biopsy). Type I endometrial cancers are usually characterized by histology consistent with <span>endometrioid adenocarcinoma that are often well-differentiated and only superficially invasive tumors at diagnosis. The prognosis for women with these tumours is typically excellent since they are often cured with
Flashcard 1411121548556
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
type 1 endometrial ca
nitive investigation early during the course of the disease (office endometrial biopsy). Type I endometrial cancers are usually characterized by histology consistent with endometrioid adenocarcinoma that are often well-differentiated and only <span>superficially invasive tumors at diagnosis. The prognosis for women with these tumours is typically excellent since they are often cured with definitive surgery alone.<span><body><html>
Flashcard 1411123121420
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
type 1 endometrial ca
metrial cancers are usually characterized by histology consistent with endometrioid adenocarcinoma that are often well-differentiated and only superficially invasive tumors at diagnosis. The prognosis for women with these tumours is typically <span>excellent since they are often cured with definitive surgery alone.<span><body><html>
Flashcard 1411124694284
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
type 1 endometrial ca
by histology consistent with endometrioid adenocarcinoma that are often well-differentiated and only superficially invasive tumors at diagnosis. The prognosis for women with these tumours is typically excellent since they are often cured with <span>definitive surgery alone.<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411127577868
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
type 2 endometrial ca
Type II is usually characterized as non-estrogen related, and seem to have a different pathogenesis according to mutation analyses (p53 mutations common). Women with type II cancer are typicall
Flashcard 1411130723596
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
type 2 endometrial ca
Type II endometrial ca is usually characterized as non-estrogen related, and seem to have a different pathogenesis according to mutation analyses (p53 mutations common). Women with type II cancer are typically normal weight, multiparous and may be African A
Flashcard 1411132296460
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
type 2 endometrial ca
l>Type II endometrial ca is usually characterized as non-estrogen related, and seem to have a different pathogenesis according to mutation analyses (p53 mutations common). Women with type II cancer are typically normal weight, multiparous and may be African American. Women with these tumours often present with advanced stage disease or more aggressive underlying histologic subtypes, which may not have abnormal vaginal bleeding early in their course
Flashcard 1411133869324
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
type 2 endometrial ca
ated, and seem to have a different pathogenesis according to mutation analyses (p53 mutations common). Women with type II cancer are typically normal weight, multiparous and may be African American. Women with these tumours often present with <span>advanced stage disease or more aggressive underlying histologic subtypes, which may not have abnormal vaginal bleeding early in their course. The prognosis for type II endometrial carcinoma is t
Flashcard 1411135442188
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
type 2 endometrial ca
ifferent pathogenesis according to mutation analyses (p53 mutations common). Women with type II cancer are typically normal weight, multiparous and may be African American. Women with these tumours often present with advanced stage disease or <span>more aggressive underlying histologic subtypes, which may not have abnormal vaginal bleeding early in their course. The prognosis for type II endometrial carcinoma is typically worse than type I with a poor five-year surviv
Flashcard 1411137015052
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
type 2 endometrial ca
common). Women with type II cancer are typically normal weight, multiparous and may be African American. Women with these tumours often present with advanced stage disease or more aggressive underlying histologic subtypes, which may not have <span>abnormal vaginal bleeding early in their course. The prognosis for type II endometrial carcinoma is typically worse than type I with a poor five-year survival. <span><body><html>
Flashcard 1411138587916
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
type 2 endometrial ca
sent with advanced stage disease or more aggressive underlying histologic subtypes, which may not have abnormal vaginal bleeding early in their course. The prognosis for type II endometrial carcinoma is typically worse than type I with a poor <span>five-year survival. <span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411141995788
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
surgical stage is the most important predictor of survival for patients with endometrial cancer
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411146452236
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
In endometrial ca, only after appropriate staging may optimal recommendations be made regarding the role, if any, for post-operative (adjuvant) radiation and/or chemotherapy.
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411149335820
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Patients with endometrial cancer typically undergo (simple) total hysterectomy, bilateral salpingo-oophorectomy, and surgical staging at the time of definitive primary surgery
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411152219404
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Most patients with stage I endometrial ca require no further therapy, as they have few negative prognostic factors and an excellent prognosis is expected
Flashcard 1411153792268
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Most patients with stage I endometrial ca require no further therapy, as they have few negative prognostic factors and an excellent prognosis is expected
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411157462284
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Patients with stage II endometrial ca typically receive adjuvant radiation therapy that often includes external pelvic radiation and vaginal brachytherapy to reduce the likelihood of disease recurrence within
Flashcard 1411159035148
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Patients with stage II endometrial ca typically receive adjuvant radiation therapy that often includes external pelvic radiation and vaginal brachytherapy to reduce the likelihood of disease recurrence within the pelvis (due to undetected microscopic lymphatic
Flashcard 1411160608012
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Patients with stage II endometrial ca typically receive adjuvant radiation therapy that often includes external pelvic radiation and vaginal brachytherapy to reduce the likelihood of disease recurrence within the pelvis (due to undetected microscopic lymphatic metastases) and the vaginal vault
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411163491596
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
In patients with stage III endometrial ca, treatment is highly individualized based on the particular poor prognostic factors present and typically consists of a combination of radiation therapy (pelvic +/- vagin
Flashcard 1411165064460
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
In patients with stage III endometrial ca, treatment is highly individualized based on the particular poor prognostic factors present and typically consists of a combination of radiation therapy (pelvic +/- vaginal brachytherapy) with either systemic chemotherapy
Flashcard 1411166637324
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
>In patients with stage III endometrial ca, treatment is highly individualized based on the particular poor prognostic factors present and typically consists of a combination of radiation therapy (pelvic +/- vaginal brachytherapy) with either <span>systemic chemotherapy<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411173190924
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Dystocia • In the active phase of the first stage: >4 hours of < 0.5cm/hr cervical dilatation • In the second stage: >1 hour with no fetal descent during active pushing
Flashcard 1411174763788
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Dystocia • In the active phase of the first stage: >4 hours of < 0.5cm/hr cervical dilatation • In the second stage: >1 hour with no fetal descent during active pushing
Flashcard 1411176336652
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Dystocia • In the active phase of the first stage: >4 hours of < 0.5cm/hr cervical dilatation • In the second stage: >1 hour with no fetal descent during active pushing
Flashcard 1411177909516
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Dystocia • In the active phase of the first stage: >4 hours of < 0.5cm/hr cervical dilatation • In the second stage: >1 hour with no fetal descent during active pushing
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411180793100
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
The latent phase of labour is complete and the active phase begins when a primiparous woman reaches 3-4 cms and a multiparous woman reaches 4-5 cms
Flashcard 1411182365964
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
The latent phase of labour is complete and the active phase begins when a primiparous woman reaches 3-4 cms and a multiparous woman reaches 4-5 cms
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411185511692
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Etiology of Dystocia: The 4 P’s 1 . Power • Contractions may be hypotonic or inco-ordinate • Maternal expulsive efforts may be inadequate 2 . Passenger • Fetal position • Fetal attitude • Fetal
Flashcard 1411187084556
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Etiology of Dystocia: The 4 P’s 1 . Power • Contractions may be hypotonic or inco-ordinate • Maternal expulsive efforts may be inadequate 2 . Passenger • Fetal position • Fetal attitude • Fetal size • Fetal anomalies (hydrocephalus) 3 . Passage • Pelvic structure • Soft tissue obstruction (tumors,
Flashcard 1411188657420
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
wer • Contractions may be hypotonic or inco-ordinate • Maternal expulsive efforts may be inadequate 2 . Passenger • Fetal position • Fetal attitude • Fetal size • Fetal anomalies (hydrocephalus) 3 . <span>Passage • Pelvic structure • Soft tissue obstruction (tumors, full bladder/full rectum, vaginal septum) 4 . Psyche • Anxiety • Stress • Pain<span></body
Flashcard 1411190230284
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
enger • Fetal position • Fetal attitude • Fetal size • Fetal anomalies (hydrocephalus) 3 . Passage • Pelvic structure • Soft tissue obstruction (tumors, full bladder/full rectum, vaginal septum) 4 . <span>Psyche • Anxiety • Stress • Pain<span><body><html>
Flashcard 1411191803148
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Etiology of Dystocia: The 4 P’s 1 . Power • Contractions may be hypotonic or inco-ordinate • Maternal expulsive efforts may be inadequate 2 . Passenger • Fetal position • Fetal attitude • Fetal size • Fetal anomalies (hydrocephalus) 3 . P
Flashcard 1411193376012
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Etiology of Dystocia: The 4 P’s 1 . Power • Contractions may be hypotonic or inco-ordinate • Maternal expulsive efforts may be inadequate 2 . Passenger • Fetal position • Fetal attitude • Fetal size • Fetal anomalies (hydrocephalus) 3 . Passage • Pelvic structure • Soft tissue o
Flashcard 1411194948876
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Etiology of Dystocia: The 4 P’s 1 . Power • Contractions may be hypotonic or inco-ordinate • Maternal expulsive efforts may be inadequate 2 . Passenger • Fetal position • Fetal attitude • Fetal size • Fetal anomalies (hydrocephalus) 3 . Passage • Pelvic structure • Soft tissue obstruction (tumors, full bladder/full rectu
Flashcard 1411196521740
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Etiology of Dystocia: The 4 P’s 1 . Power • Contractions may be hypotonic or inco-ordinate • Maternal expulsive efforts may be inadequate 2 . Passenger • Fetal position • Fetal attitude • Fetal size • Fetal anomalies (hydrocephalus) 3 . Passage • Pelvic structure • Soft tissue obstruction (tumors, full bladder/full rectum, vaginal septum)
Flashcard 1411198094604
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
an>Etiology of Dystocia: The 4 P’s 1 . Power • Contractions may be hypotonic or inco-ordinate • Maternal expulsive efforts may be inadequate 2 . Passenger • Fetal position • Fetal attitude • Fetal size • Fetal anomalies (hydrocephalus) 3 . Passage • Pelvic structure • Soft tissue obstruction (tumors, full bladder/full rectum, vaginal septum) 4 . Psyche 
Flashcard 1411199667468
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
of Dystocia: The 4 P’s 1 . Power • Contractions may be hypotonic or inco-ordinate • Maternal expulsive efforts may be inadequate 2 . Passenger • Fetal position • Fetal attitude • Fetal size • Fetal <span>anomalies (hydrocephalus) 3 . Passage • Pelvic structure • Soft tissue obstruction (tumors, full bladder/full rectum, vaginal septum) 4 . Psyche • Anxiety • Stress • Pain</
Flashcard 1411201240332
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
ractions may be hypotonic or inco-ordinate • Maternal expulsive efforts may be inadequate 2 . Passenger • Fetal position • Fetal attitude • Fetal size • Fetal anomalies (hydrocephalus) 3 . Passage • <span>Pelvic structure • Soft tissue obstruction (tumors, full bladder/full rectum, vaginal septum) 4 . Psyche • Anxiety • Stress • Pain<span><body><html>
Flashcard 1411202813196
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
c or inco-ordinate • Maternal expulsive efforts may be inadequate 2 . Passenger • Fetal position • Fetal attitude • Fetal size • Fetal anomalies (hydrocephalus) 3 . Passage • Pelvic structure • <span>Soft tissue obstruction (tumors, full bladder/full rectum, vaginal septum) 4 . Psyche • Anxiety • Stress • Pain<span><body><html>
Flashcard 1411204386060
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
etal position • Fetal attitude • Fetal size • Fetal anomalies (hydrocephalus) 3 . Passage • Pelvic structure • Soft tissue obstruction (tumors, full bladder/full rectum, vaginal septum) 4 . Psyche • <span>Anxiety • Stress • Pain<span><body><html>
Flashcard 1411205958924
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
13; • Fetal attitude • Fetal size • Fetal anomalies (hydrocephalus) 3 . Passage • Pelvic structure • Soft tissue obstruction (tumors, full bladder/full rectum, vaginal septum) 4 . Psyche • Anxiety • <span>Stress • Pain<span><body><html>
Flashcard 1411207531788
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
titude • Fetal size • Fetal anomalies (hydrocephalus) 3 . Passage • Pelvic structure • Soft tissue obstruction (tumors, full bladder/full rectum, vaginal septum) 4 . Psyche • Anxiety • Stress • <span>Pain<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411210415372
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Methods of Prevention of Dystocia • Supportive companion during labour results in faster progress of labour • Have one to one nurse during labour • Maintain ambulation and upright position in labour as much as possible • Mainta
Flashcard 1411211988236
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Methods of Prevention of Dystocia • Supportive companion during labour results in faster progress of labour • Have one to one nurse during labour • Maintain ambulation and upright position in labour as much as possible • Maintain adequate hydration • Do not delay in managing non-progressive active lab
Flashcard 1411213561100
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Methods of Prevention of Dystocia • Supportive companion during labour results in faster progress of labour • Have one to one nurse during labour • Maintain ambulation and upright position in labour as much as possible • Maintain adequate hydration • Do not delay in managing non-progressive active labour with rupture of membranes and oxytocin
Flashcard 1411215133964
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
of Prevention of Dystocia • Supportive companion during labour results in faster progress of labour • Have one to one nurse during labour • Maintain ambulation and upright position in labour as much as possible • Maintain <span>adequate hydration • Do not delay in managing non-progressive active labour with rupture of membranes and oxytocin<span><body><html>
Flashcard 1411216706828
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
progress of labour • Have one to one nurse during labour • Maintain ambulation and upright position in labour as much as possible • Maintain adequate hydration • Do not delay in managing non-progressive active labour with <span>rupture of membranes and oxytocin<span><body><html>
| status | not read | reprioritisations | ||
|---|---|---|---|---|
| last reprioritisation on | suggested re-reading day | |||
| started reading on | finished reading on |
Flashcard 1411219590412
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Important Factors in the Evaluation of the Patient with Abnormal Labour 1 . Review the labour record 2 . Assess maternal status • Vitals • Pain management • Contraction pattern • Membranes: intact vs ruptured • Cervical dilatation and effacement •
Flashcard 1411221163276
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Important Factors in the Evaluation of the Patient with Abnormal Labour 1 . Review the labour record 2 . Assess maternal status • Vitals • Pain management • Contraction pattern • Membranes: intact vs ruptured • Cervical dilatation and effacement • Pelvic architecture 3 . Asse
Flashcard 1411222736140
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Important Factors in the Evaluation of the Patient with Abnormal Labour 1 . Review the labour record 2 . Assess maternal status • Vitals • Pain management • Contraction pattern • Membranes: intact vs ruptured • Cervical dilatation and effacement • Pelvic architecture 3 . Assess fetal status
Flashcard 1411224309004
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Important Factors in the Evaluation of the Patient with Abnormal Labour 1 . Review the labour record 2 . Assess maternal status • Vitals • Pain management • Contraction pattern • Membranes: intact vs ruptured • Cervical dilatation and effacement • Pelvic architecture 3 . Assess fetal status • Fet
Flashcard 1411225881868
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Important Factors in the Evaluation of the Patient with Abnormal Labour 1 . Review the labour record 2 . Assess maternal status • Vitals • Pain management • Contraction pattern • Membranes: intact vs ruptured • Cervical dilatation and effacement • Pelvic architecture 3 . Assess fetal status • Fetal heart • Fetal station&
Flashcard 1411227454732
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
d><head>Important Factors in the Evaluation of the Patient with Abnormal Labour 1 . Review the labour record 2 . Assess maternal status • Vitals • Pain management • Contraction pattern • Membranes: intact vs ruptured • Cervical dilatation and effacement • Pelvic architecture 3 . Assess fetal status • Fetal heart • Fetal station • Fetal presentation and position 4
Flashcard 1411229027596
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
Factors in the Evaluation of the Patient with Abnormal Labour 1 . Review the labour record 2 . Assess maternal status • Vitals • Pain management • Contraction pattern • Membranes: intact vs ruptured • <span>Cervical dilatation and effacement • Pelvic architecture 3 . Assess fetal status • Fetal heart • Fetal station • Fetal presentation and position 4 . Determine best course of action 
Flashcard 1411230600460
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
ith Abnormal Labour 1 . Review the labour record 2 . Assess maternal status • Vitals • Pain management • Contraction pattern • Membranes: intact vs ruptured • Cervical dilatation and effacement • <span>Pelvic architecture 3 . Assess fetal status • Fetal heart • Fetal station • Fetal presentation and position 4 . Determine best course of action • If membranes are not ru
Flashcard 1411232173324
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
the labour record 2 . Assess maternal status • Vitals • Pain management • Contraction pattern • Membranes: intact vs ruptured • Cervical dilatation and effacement • Pelvic architecture 3 . Assess <span>fetal status • Fetal heart • Fetal station • Fetal presentation and position 4 . Determine best course of action • If membranes are not ruptured then do Artificial Rupt
Flashcard 1411233746188
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
2 . Assess maternal status • Vitals • Pain management • Contraction pattern • Membranes: intact vs ruptured • Cervical dilatation and effacement • Pelvic architecture 3 . Assess fetal status • Fetal <span>heart • Fetal station • Fetal presentation and position 4 . Determine best course of action • If membranes are not ruptured then do Artificial Rupture of Membranes (AR
Flashcard 1411235319052
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
l status • Vitals • Pain management • Contraction pattern • Membranes: intact vs ruptured • Cervical dilatation and effacement • Pelvic architecture 3 . Assess fetal status • Fetal heart • Fetal <span>station • Fetal presentation and position 4 . Determine best course of action • If membranes are not ruptured then do Artificial Rupture of Membranes (AROM) • Offer pain
Flashcard 1411236891916
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
ls • Pain management • Contraction pattern • Membranes: intact vs ruptured • Cervical dilatation and effacement • Pelvic architecture 3 . Assess fetal status • Fetal heart • Fetal station • Fetal <span>presentation and position 4 . Determine best course of action • If membranes are not ruptured then do Artificial Rupture of Membranes (AROM) • Offer pain relief: endogenous catecholamines can
Flashcard 1411238464780
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
and effacement • Pelvic architecture 3 . Assess fetal status • Fetal heart • Fetal station • Fetal presentation and position 4 . Determine best course of action • If membranes are not ruptured then do <span>Artificial Rupture of Membranes (AROM) • Offer pain relief: endogenous catecholamines can inhibit uterine contractility. Ensure adequate hydration • Oxytocin infusion to improve uterine contractility • If all
Flashcard 1411240037644
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
al station • Fetal presentation and position 4 . Determine best course of action • If membranes are not ruptured then do Artificial Rupture of Membranes (AROM) • Offer pain relief: endogenous catecholamines can inhibit <span>uterine contractility. Ensure adequate hydration • Oxytocin infusion to improve uterine contractility • If all the above tried consider operative delivery (i.e. CS or assisted vaginal birth if full
Flashcard 1411241610508
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
. Determine best course of action • If membranes are not ruptured then do Artificial Rupture of Membranes (AROM) • Offer pain relief: endogenous catecholamines can inhibit uterine contractility. Ensure adequate hydration • <span>Oxytocin infusion to improve uterine contractility • If all the above tried consider operative delivery (i.e. CS or assisted vaginal birth if fully dilated)<span><body><html>
Flashcard 1411243183372
| status | not learned | measured difficulty | 37% [default] | last interval [days] | |||
|---|---|---|---|---|---|---|---|
| repetition number in this series | 0 | memorised on | scheduled repetition | ||||
| scheduled repetition interval | last repetition or drill |
Open it
cial Rupture of Membranes (AROM) • Offer pain relief: endogenous catecholamines can inhibit uterine contractility. Ensure adequate hydration • Oxytocin infusion to improve uterine contractility • If all the above tried consider <span>operative delivery (i.e. CS or assisted vaginal birth if fully dilated)<span><body><html>